Download presentation
Presentation is loading. Please wait.

1
Ankle Sprain Imitators
Leslie A. Michaud, M.D. Steadman Hawkins Clinic of the Carolinas Primary Care Sports Medicine Fellow

2
Foot and ankle Statistics
1982: NCAA develops the ISS (injury surveillance system) years of ISS data showed that ankle sprains are the most common injury 14.9% of all injuries Compare to ACL 2.6% Concussion 5% 39.7% of high school injuries are foot and ankle Olympic summer games Athens – 22% of injuries were ankle sprains Olympic winter games Salt Lake City – 25% foot and ankle Collegiate basketball - higher rate of grade I ankle sprains in women than men 1. Dick R, Agel J, Marshall SW: National Collegiate Athletic Association Injury Surveillance System commentaries:Introduction and methods. J Athl Train 2007;42(2): 2. Hootman JM, Dick R, Agel J:Epidemiology of collegiate injuries for 15sports: Summary and recommendations for injury prevention initiatives. J AthlTrain 2007;42(2): 3. Borowski LA, Yard EE, Fields SK, Comstock RD: The epidemiology of US high school basketball injuries, 2005- 2007. Am J Sports Med 2008;36(12): 4. Badekas T, Papadakis SA, Vergados N,et al: Foot and ankle injuries during the Athens 2004 Olympic Games. J Foot Ankle Res 2009;2:9. 5. Crim JR: Winter sports injuries: The 2002 Winter Olympics experience and a review of the literature. Magn Reson Imaging Clin N Am 2003;11(2): 6. Hosea TM, Carey CC, Harrer MF: The gender issue: Epidemiology of ankle injuries in athletes who participate in basketball. Clin Orthop Relat Res 2000;372:45-49.
 years of ISS data showed that ankle sprains are the most common injury 14.9% of all injuries. Compare to ACL 2.6% Concussion 5% 39.7% of high school injuries are foot and ankle Olympic summer games Athens – 22% of injuries were ankle sprains Olympic winter games Salt Lake City – 25% foot and ankle. Collegiate basketball - higher rate of grade I ankle sprains in women than men. 1. Dick R, Agel J, Marshall SW: National Collegiate Athletic Association Injury Surveillance System commentaries:Introduction and methods. J Athl Train 2007;42(2): Hootman JM, Dick R, Agel J:Epidemiology of collegiate injuries for 15sports: Summary and recommendations for injury prevention initiatives. J AthlTrain 2007;42(2): Borowski LA, Yard EE, Fields SK, Comstock RD: The epidemiology of US high school basketball injuries, Am J Sports Med 2008;36(12): Badekas T, Papadakis SA, Vergados N,et al: Foot and ankle injuries during the Athens 2004 Olympic Games. J Foot Ankle Res 2009;2:9. 5. Crim JR: Winter sports injuries: The 2002 Winter Olympics experience and a review of the literature. Magn Reson Imaging Clin N Am 2003;11(2): Hosea TM, Carey CC, Harrer MF: The gender issue: Epidemiology of ankle injuries in athletes who participate in basketball. Clin Orthop Relat Res 2000;372:")
3
Tibia Fibula Medial Malleolus Tibial Plafond Lateral Malleolus Talus
Talus is largely covered in cartilage. Subtalar joint: inversion/eversion function of the ankle. Tibial plafond or ceiliing; broader anteriorly Subtalar joint

5
Resists posterior displacement
Provides stabilization in plantarflexion ATFL is the weakest of the three and most likely to be injured because in the plantarflexed/inverted foot (the MOI) it is most susceptible Stabilizes ankle and subtalar joint; especially during inversion
 it is most susceptible. Stabilizes ankle and subtalar joint; especially during inversion.")
6
Evaluation of Foot and Ankle Injuries
Identify and localize the injured bony and soft-tissue structures Determine MOI Clues regarding location and severity of injury Clues to potential concomitant injuries that may be overlooked More extensive evaluation in severe sprains Arouse suspicion of fx or articular injury 1% of ankle sprains are syndesmotic - more common with eversion Persistent symptoms 4-6 weeks despite appropriate treatment

7
Imitators Osteochondral lesions of the talar dome
Lateral process talar fractures Peroneal tendon subluxation and dislocation Base of the 5th metatarsal (avulsion) Tarsal coalition
 Tarsal coalition.")
8
Osteochondral Lesions of the Talar Dome
Injury to the cartilage and underlying bone of the talus History of trauma in 98% of lateral dome lesions 70% of medial dome lesions Trauma is often an inversion-type injury Initial radiographs often unremarkable Seen best on mortise view

9
Berndt and Hardy Classification

10
Osteochondral Lesion Presentation
Persistent pain and swelling well after injury Occasionally will have a slow onset +/- mechanical symptoms Intraarticular process

12
Why do we need to catch an osteochondral lesion early?
The fracture damages vascular supply to the subchondral bone If treated early, capillaries can restore bloodflow If not, prolonged weight-bearing causes fibrous tissue to accumulate which will block capillary ingrowth Leading to AVN and later DJD

13
Diagnosis and Treatment
CT or MRI if radiographs negative and suspicion is high Conservative Rest and immobilization Surgical Drilling Debridement Excision of fragment Osteochondral graft Immobilization is often casting

14
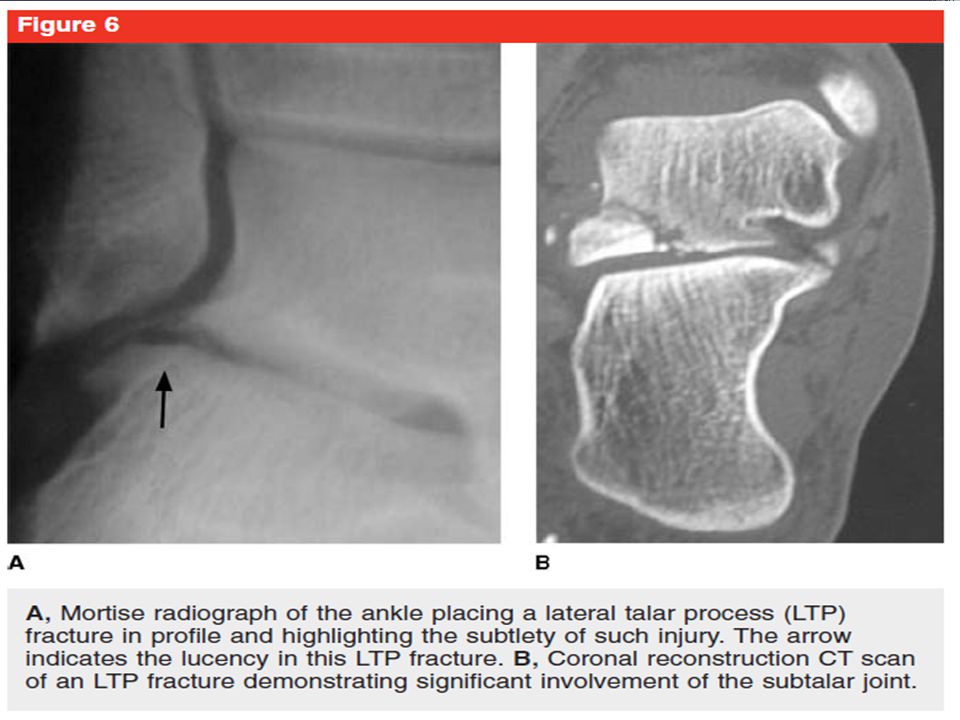
Lateral Talar Process Fractures
“Snowboarder’s fracture” Often subtle presentation plain films Best seen, if at all, on mortise. Clinically resemble an inversion ankle sprain Tenderness 1 cm from the tip of the lateral malleolus at the lateral talus

15
Lateral Talar Process Fracture Facts
24% of talar fractures are at the lateral process <1% of all ankle injuries are LTP fx 15% are misdiagnosed as ankle sprains Exam findings: “tenderness 1 cm inferior to tip of lateral malleolus” mimic ATFL McCrory P, Bladin C: Fractures of the lateral process of the talus: A clinical review. “Snowboarder’s ankle”. Clin J Sport Med 1996;6: Boon AJ, Smith J, Zobitz ME, Amrami KM: Snowboarder’s talus fracture: Mechanism of injury. Am J Sports Med 2001;29:

17
MOI: dorsiflexion + inversion + ER force
More of an impact or crush injury Comminution More often than not have IA involvement

19
Evaluation and Treatment
CT in all cases to determine intraarticular involvement and level of comminution Conservative Only for non-displaced SLNWB cast for 4 weeks Advance WB in boot for 2 additional weeks Operative Excision (fragments <1cm) ORIF (fragments >1cm)
 ORIF (fragments >1cm)")
20
Peroneal Tendon Instability
Subluxation or dislocation Can be associated with chronic lateral ankle instability Functional Mechanical Previous injury Concern for degenerative tears of the peroneus brevis tendon Persistent pain after Grade III sprains is commonly due to incomplete rehab with too early RTP Peroneal strengthening

21
Brevis and longus originate from the lateral fibula: Brevis to 5th metatarsal base and Longus to 1st metatarsal base. Make up lateral compartment. Innervation is superficial peroneal n. Common n

22
Superficial Peroneal Nerve
Supplies lateral compartment muscles High incidence of neuropraxia Grade II and III sprains Almost all resolve spontaneously with time Nitz AJ, Dobner JJ, Kersey D: Nerve injury and grades II and III ankle sprains. Am J Sports Med 1985;13(3):
:")
23
History and Physical Exam
Previous inversion injury Specific activities i.e. dancers Swelling and possibly ecchymosis (acute) posterior to lateral malleolus Stress test Resist dorsiflexion from the plantarflexed position while the foot is in inversion Varus hindfoot
 posterior to lateral malleolus. Stress test. Resist dorsiflexion from the plantarflexed position while the foot is in inversion. Varus hindfoot.")
25
Treatment Conservative Surgical Acute injuries Chronic Reattachment
Reduce tendon and SLWB cast for 6 weeks 50% success rate Chronic PT Surgical Reattachment Deepen groove Reroute tendon Reconstruct retinaculum Bone block

26
Tarsal Coalition Congenital fusion of tarsal bones Rigid flatfoot
Calcaneus to navicular most common 8-12 years old Talus to calcaneus 12-15 years old Rigid flatfoot “Peroneal spastic flatfoot”

27
Ant-eater sign…. Elongated anterior calcaneal process

28
History and Physical Exam
Lateral ankle pain Worse with activity May radiate to calf Inspect feet Flat Hindfoot valgus No arch with toe raise Limited subtalar motion Tight heel cords

30
Evaluation and Treatment
CT or MRI Looking for other coalitions Determine size Conservative If asymptomatic – observation Symptomatic – orthotics or casting Surgical Resect coalition and interpose with fat graft or EDB tendon Arthrodesis – not often used Conservative treatment is successful in many cases

31
Thank you for your attention!
Questions?

32
Bibliography Dick R, Agel J, Marshall SW: National Collegiate Athletic Association Injury Surveillance System commentaries:Introduction and methods. J Athl Train 2007;42(2): Hootman JM, Dick R, Agel J:Epidemiology of collegiate injuries for 15sports: Summary and recommendations for injury prevention initiatives. J AthlTrain 2007;42(2): Borowski LA, Yard EE, Fields SK, Comstock RD: The epidemiology of US high school basketball injuries, 2005-Am J Sports Med 2008;36(12): Badekas T, Papadakis SA, Vergados N,et al: Foot and ankle injuries during the Athens 2004 Olympic Games. J Foot Ankle Res 2009;2:9. Crim JR: Winter sports injuries: The 2002 Winter Olympics experience and a review of the literature. Magn Reson Imaging Clin N Am 2003;11(2): Hosea TM, Carey CC, Harrer MF: The gender issue: Epidemiology of ankle injuries in athletes who participate in basketball. Clin Orthop Relat Res 2000;372:45-49 Anderson RB, Hunt KJ, McCormick JJ. J Am Acad Orthop Surg 2010;18: McCrory P, Bladin C: Fractures of the lateral process of the talus: A clinical review. “Snowboarder’s ankle”. Clin J Sport Med 1996;6: Boon AJ, Smith J, Zobitz ME, Amrami KM: Snowboarder’s talus fracture: Mechanism of injury. Am J Sports Med 2001;29: Weatherby, Brian. “Start Smart: What Every Practitioner Should Know About Treating Foot and Ankle Pain.” Powerpoint presentation. DeLee and Drez's Orthopaedic Sports Medicine, 3rd ed. Copyright © 2009 Saunders, An Imprint of Elsevier Renstrom PA: Persistently painful sprained ankle. J Am Acad Orthop Surg 1994;2(5): Nitz AJ, Dobner JJ, Kersey D: Nerve injury and grades II and III ankle sprains. Am J Sports Med 1985;13(3):
: Hootman JM, Dick R, Agel J:Epidemiology of collegiate injuries for 15sports: Summary and recommendations for injury prevention initiatives. J AthlTrain 2007;42(2): Borowski LA, Yard EE, Fields SK, Comstock RD: The epidemiology of US high school basketball injuries, 2005-Am J Sports Med 2008;36(12): Badekas T, Papadakis SA, Vergados N,et al: Foot and ankle injuries during the Athens 2004 Olympic Games. J Foot Ankle Res 2009;2:9. Crim JR: Winter sports injuries: The 2002 Winter Olympics experience and a review of the literature. Magn Reson Imaging Clin N Am 2003;11(2): Hosea TM, Carey CC, Harrer MF: The gender issue: Epidemiology of ankle injuries in athletes who participate in basketball. Clin Orthop Relat Res 2000;372: Anderson RB, Hunt KJ, McCormick JJ. J Am Acad Orthop Surg 2010;18: McCrory P, Bladin C: Fractures of the lateral process of the talus: A clinical review. Snowboarder’s ankle . Clin J Sport Med 1996;6: Boon AJ, Smith J, Zobitz ME, Amrami KM: Snowboarder’s talus fracture: Mechanism of injury. Am J Sports Med 2001;29: Weatherby, Brian. Start Smart: What Every Practitioner Should Know About Treating Foot and Ankle Pain. Powerpoint presentation. DeLee and Drez s Orthopaedic Sports Medicine, 3rd ed. Copyright © 2009 Saunders, An Imprint of Elsevier. Renstrom PA: Persistently painful sprained ankle. J Am Acad Orthop Surg 1994;2(5): Nitz AJ, Dobner JJ, Kersey D: Nerve injury and grades II and III ankle sprains. Am J Sports Med 1985;13(3):")
Similar presentations








>")


 Radiographic Evaluation of the Ankle>")












