Download presentation
Presentation is loading. Please wait.

1
Female Urinary Incontinence; Tips for Taming the Tinkles
Felecia Fick, CRTT, PA-C

2
Disclosures None

3
Objectives Describe the evaluation of patients with urinary incontinence Discuss how to diagnose different types of urinary incontinence List treatment considerations for different types of urinary incontinence Describe when to refer patients with urinary incontinence

4
Normal Micturition Cycle
Detrusor muscle relaxes as it fills with urine due to sympathetic stimulation. Parasympathetic stimulation causes the bladder to contract and urethral sphincter and pelvic muscle to relax. When urge is strong enough and it is social appropriate to urinate, the pelvic floor relaxes, bladder contracts and you urinate. Bladder is constantly in a state of inhibition to contract. WE consciously release that inhibition, then bladder contracts and you void.

5
What is normal? Diurnal frequency- 8 voids Nocturia- 0-1 void
Bladder capacity cc Normal voids cc Daily fluid intake ounces So what are the normal parameters? These are just general guidelines… 400cc bladder capacity is for the best bladder contraction void. Dietician came up with fluid intake of 64 oz daily years ago with no scientific evidence and it has been passed on ever since.

6
What is urinary incontinence?
Any involuntary loss of urine (International Continence Society/ICS and American Urological Association/AUA) The symptom is the patient’s complaint The sign is the objective demonstration of urine loss Loss of bladder control (Mayo Clinic) Lots of definitions of UI-some strict, some not. It’s the loss of urine without you wanting it to is the pt’s complaint. The sign is seeing urinary incontinence on exam. At Mayo we commonly say loss of bladder control.
 The symptom is the patient’s complaint. The sign is the objective demonstration of urine loss. Loss of bladder control (Mayo Clinic) Lots of definitions of UI-some strict, some not. It’s the loss of urine without you wanting it to is the pt’s complaint. The sign is seeing urinary incontinence on exam. At Mayo we commonly say loss of bladder control.")
7
Prevalence At least 50% of patients do not report urinary incontinence [5] 25-51% of the population Around 13 million in the United States [6,7] More commonly seen caucasians,[4] multiple childbirths [10], aging [8], living in a nursing home [9]
![Prevalence At least 50% of patients do not report urinary incontinence [5] 25-51% of the population.](http://slideplayer.com/slide/2802698/10/images/7/Prevalence+At+least+50%25+of+patients+do+not+report+urinary+incontinence+%5B5%5D+25-51%25+of+the+population..jpg "Around 13 million in the United States [6,7] More commonly seen caucasians,[4] multiple childbirths [10], aging [8], living in a nursing home [9]")
8
Types of urinary incontinence
Stress Urge Mixed Overflow Functional Neurogenic Transient Looking at incontinence, the difficulty is addressing the different types. So, it is important to recognize the different types. Stress incontinence most common. Not going to focus much on the functional, neurogenic, transient today-but will give you the definitions so you know.

9
Stress Incontinence Involuntary loss of urine occurring when the intravesical pressure exceeds the maximum urethral pressure in the absence of a detrusor contraction (ICS) Loss of urine with exertion -coughing, sneezing Risk factors- pregnancy, vaginal deliveries, heredity, obesity Norton’s test What is stress incontinence? Losing urine (without wanting to) due to bladder pressures that are higher than urethral/sphincter pressures when the bladder isn’t squeezing. That is the definition from the international continence society. What activities cause this? C, S, running, lifting, reaching, even rolling over in bed
 Loss of urine with exertion -coughing, sneezing. Risk factors- pregnancy, vaginal deliveries, heredity, obesity. Norton’s test. What is stress incontinence Losing urine (without wanting to) due to bladder pressures that are higher than urethral/sphincter pressures when the bladder isn’t squeezing. That is the definition from the international continence society. What activities cause this C, S, running, lifting, reaching, even rolling over in bed.")
10
Urge incontinence (Overactive Bladder)
Involuntary loss of urine associated with a strong desire to void/urgency (ICS) Risk factors- aging, obesity, genetics, though usually idiopathic ***Urinary tract infection When you get an urge to urinate and can’t make it to the bathroom, that leakage of urine is called urge incontinence. Most common cause of urge incontinence UTI-so rule this out with by taking urine specimen.
 Risk factors- aging, obesity, genetics, though usually idiopathic. ***Urinary tract infection. When you get an urge to urinate and can’t make it to the bathroom, that leakage of urine is called urge incontinence. Most common cause of urge incontinence UTI-so rule this out with by taking urine specimen.")
11
Mixed incontinence Combination of stress AND urinary urge incontinence
Mixed incontinence- Those women who are blessed to have both

12
Overflow incontinence
Bladder is not emptying and overflows Frequent small urinations Constant dribbling Causes- Weak detrusor contraction (neurological) Outlet obstruction (pelvic prolapse, surgical procedures) Overflow incontinence is when your bladder is always full/stretched and doesn’t empty. Why does this happen? Your bladder is weak due to a neurogenic cause. Prolapse or surgical procedures can cause outlet obstruction
 Outlet obstruction (pelvic prolapse, surgical procedures) Overflow incontinence is when your bladder is always full/stretched and doesn’t empty. Why does this happen Your bladder is weak due to a neurogenic cause. Prolapse or surgical procedures can cause outlet obstruction.")
13
Functional incontinence
Incontinence due to a physical or cognitive impairment in the setting of a normal functioning urinary tract Causes- Mobility- (arthritis, orthopedic surgery) Cognition- (Alzheimer's disease) Pts using walker after ortho surgery
 Cognition- (Alzheimer s disease) Pts using walker after ortho surgery.")
14
Neurogenic Bladders (incontinence)
Incontinence due to a neurogenic cause Examples- (multiple sclerosis, spinal cord injuries, parkinsons, stroke) May present as urge, stress, overflow, or retention Requires a subspecialty appointment with a neurourologist so refer them If a pt has a neurological diagnosis and bladder symptomatology-she has a neurogenic bladder.
 May present as urge, stress, overflow, or retention. Requires a subspecialty appointment with a neurourologist so refer them. If a pt has a neurological diagnosis and bladder symptomatology-she has a neurogenic bladder.")
15
Transient incontinence
Temporary incontinence Occurs in 33% of community dwelling elderly and 50% of acutely hospitalized patients Secondary to “DIAPPERS” D elirium I nfection A trophic vaginitis P harmacological P sychological E ndocrine R estricted mobility S tool impaction [1,2,3] A third of our elderly neighbors have this. ½ of all acutely hospitalized pts do as well. Atrophic Vaginitis-due to a weakened sphincter from weakened vaginal tissue Endocrine-diabetes, diabetes insipidus The good thing about transient incontinence is that it IS temporary. If you correct the underlying problem, you correct the incontinence.

16
Don’t ask, don’t tell-patient perspective
Patient embarrassment Belief that symptoms are normal Belief that symptoms will subside Patient is unaware of treatment options or that treatment will be successful Afraid of invasive, costly procedures - specifically the CATHETER…. Many times the patient is embarrassed. She thinks this is normal. She believes that her incontinence will go away. She doesn’t know something can be done to help her. She is afraid of the deadly catheter or other scary procedures…

17
Reasons incontinence is not addressed from a provider perspective
Many other important symptoms take precedence Perception that patient is not bothered Unaware of the significant impact on the patient’s quality of life Unaware of treatment options or positive benefit of treatment What can be worse than peeing your pants? Don’t be afraid to refer

18
Reasons to address incontinence
Quality of life improvement Morbidity and Mortality Cost

19
Quality of Life Quality of Life Physical Limitations or cessation of physical activity Psychological Guilt/depression Loss of self-respect/dignity Fear Social Reduction in social activity Alteration of travel plans Institutionalization Domestic Special precautions with clothing Specialized underwear, bedding Occupational Absence from work Decreased productivity Sexual Avoidance of sexual contact and intimacy There are many factors affecting quality of life. Physical-limiting activities or even stopping them Psychological- depression, loss of dignity Social-avoidance of socialization and travel Domestic- changes in clothing (wearing only dark clothes, special underwear, bedding)-hide from partner changing bedsheets Occupational- absence from work or decreased productivity Sexual avoidance
-hide from partner changing bedsheets. Occupational- absence from work or decreased productivity. Sexual avoidance.")
20
Morbidity and Mortality
Infections UTIs, urosepsis, candida, cellulitis, pressure ulcers Falls and fractures Sleep deprivation Psychological Impact Poor self-esteem, depression, social withdrawal, sexual dysfunction Caregiver burden [11,13,20]

21
Cost Billions! $20 billion in 2000 for total urinary incontinence costs to society [14] 56 percent consequence costs (i.e., nursing home admissions) and loss of productivity [15,16] $65.9B in 2007 for OAB Projected $76.2B- 2015 $82.6B-2020[17] The estimated total national cost of OAB with UUI in 2007 was $65.9 billion, with projected costs of $76.2 billion in 2015 and $82.6 billion in 2020. J Manag Care Pharm Feb;20(2): Economic burden of urgency urinary incontinence in the United States: a systematic review. Coyne KS1,et al (pub med)
![Cost Billions! $20 billion in 2000 for total urinary incontinence costs to society [14]](http://slideplayer.com/slide/2802698/10/images/21/Cost+Billions%21+%2420+billion+in+2000+for+total+urinary+incontinence+costs+to+society+%5B14%5D.jpg "56 percent consequence costs (i.e., nursing home admissions) and loss of productivity [15,16] $65.9B in 2007 for OAB. Projected $76.2B $82.6B-2020[17] The estimated total national cost of OAB with UUI in 2007 was $65.9 billion, with projected costs of $76.2 billion in 2015 and $82.6 billion in J Manag Care Pharm Feb;20(2): Economic burden of urgency urinary incontinence in the United States: a systematic review. Coyne KS1,et al (pub med)")
22
Patient evaluation History Questionnaires Voiding Diary Physical exam
Additional testing - urines - post void residual - urodynamics test - cystoscopy So let’s talk about evaluation of our patients. After all it IS one of the objectives of the talk.. Can you have the pt call the incontinence helpline shown on this slide? Too bad there’s not one, right? I use the above bullet points with each of my patients. Additional testing is evaluated on a case to case basis.

23
History You may be afraid to ask about the bladder as you could open up a can of worms. Your time is precious and limited with all the medical concerns you need to address. Never be afraid to refer these patients to Urogynecology. I would be happy to personally see them. "Whatever you do, just don't get her started on her bladder control problem."

24
Patient history Review Questionnaire (UDI=urogenital distress inventory, IIQ=incontinence impact questionnarie…) OBGYN - number of pregnancies - delivery method (vaginal, cesarean) - instruments used (forceps, suction) - degree of tearing, episiotomy Pelvic Surgery There are different types of questionnaires. Choose one and be consistent with utilization. We have our own Mayo Urogynecology questionnaire. Some practices use the UDI=Urogenital Distress Inventory. Others use the IIQ or Incontinence Impact Questionnaire. Others create their own questionnaire which we have at Mayo that the patient fills out prior to the appointment or while waiting to be roomed. This helps prepare the patient for what types of questions will be asked and helps them know what they will answer. It has worked well for my patients.
 - instruments used (forceps, suction) - degree of tearing, episiotomy. Pelvic Surgery. There are different types of questionnaires. Choose one and be consistent with utilization. We have our own Mayo Urogynecology questionnaire. Some practices use the UDI=Urogenital Distress Inventory. Others use the IIQ or Incontinence Impact Questionnaire. Others create their own questionnaire which we have at Mayo that the patient fills out prior to the appointment or while waiting to be roomed. This helps prepare the patient for what types of questions will be asked and helps them know what they will answer. It has worked well for my patients.")
25
Patient history Bladder symptoms (LUTS=lower urinary tract symptoms)
Storage symptoms Urgency Frequency Nocturia Incontinence Pain Voiding symptoms Hesitancy Weak slow stream Incomplete emptying Post void dribbling Pain

26
Bladder diary The voiding diary is a nice tool for incontinence evaluation. You can find a lot of answers just by looking at a voiding diary. Fluid intake Urine output Frequency Voided volumes which I have found to be most helpful. Incontinent episodes and descriptions of them –associated with urgency or no urgency AND….. NUMBER OF PADS

27
Patient history “Incontinence”
When do you leak urine? What triggers your leakage episodes? How often does it happen? Do you wear pads? What kind of pad? How many per day? Are they soaked or damp? When I am talking to a patient about urinary incontinence I ask these questions. Do you wear pads lets us know how bad of a problem the incontinence is. I counsel my patients on using incontinence pads rather than maxi pads to reduce skin irritation and help with holding capacity.

28
Patient history Vaginal symptoms
Itching, dryness, burning, discharge, bleeding, infection, history of skin conditions such as atrophic vaginitis or lichen sclerosus Can be seen with pelvic prolapse and/or Incontinence

29
Patient history Sexual history Sexually active or not Dyspareunia
Penetration, movement, orgasm, anorgasmic Vaginal dryness-lubricants used Post coital bleeding ?sexually transmitted infection Abuse Is the patient sexually active? Does she have dyspareunia? If so with what?

30
Patient history Bowel symptoms Constipation Fecal incontinence
Splinting Incomplete emptying The bowels play a large role in bladder symptomatology, which is why I ask about them. I work closely with the Motility clinic as the bowel and bladder go hand in hand. When bowels are not well controlled, neither are bladder symptoms.

31
Patient history Neurological Pulmonary Medical Diagnosis
Physical Mobility Mental Status including psychiatric history Obesity Medical diagnosis-diabetes or diabetes inspidius Since I brought up obesity-let’s talk about that more as it can negatively affect urinary incontinence.

32
Patient history Medication review-diuretics, lithium, etc.. Social
Smoking, alcohol, recreational drugs Family history Gynecological, urological, colorectal malignancy

33
Physical Exam General Abdominal /Back(scars, masses, CVA tenderness on the back) Urologic/gynecologic Visual inspection Skin conditions, rashes, atrophy, vaginal discharge Perineal sensation, reflexes (soft touch/sharp) Cough stress test Kegels or pelvic floor myalgia Prolapse Masses-(bartholins, urethral, skenes, diverticulum, bimanual, rectal exam included in this evaluation)
 Cough stress test. Kegels or pelvic floor myalgia. Prolapse. Masses-(bartholins, urethral, skenes, diverticulum, bimanual, rectal exam included in this evaluation)")
34
Kegels Squeezing and releasing the pelvic floor muscles which includes the vagina, urethra, rectum. Same muscle used to stop the urinary stream. Graded as absent, weak, moderate, strong. Can be taught through pelvic floor physical therapy. Used as a treatment option for urinary incontinence.

35
Squirting Sue 40 yo c/o urinary incontinence only with running (no other urogynecological symptoms) G4, P4 (vaginal, forceps with first 2, 3rd degree tearing with 3rd, largest birth weight 10 lbs) BMI 22 PMH/PSH-Healthy. No surgeries. Medications/allergies-None. Bladder diary, urines, post void residual-normal Physical exam is normal with strong kegels.
 BMI 22. PMH/PSH-Healthy. No surgeries. Medications/allergies-None. Bladder diary, urines, post void residual-normal. Physical exam is normal with strong kegels.")
36
Squirting Sue What is her diagnosis? Transient incontinence
Overflow incontinence Urge incontinence Stress incontinence Mixed incontinence

37
Squirting Sue Answer Stress incontinence Transient incontinence
Overflow incontinence Urge incontinence Stress incontinence Mixed incontinence

38
Squirting Sue First LineTreatment
1) Urethral insert (Femsoft) 2) Pessary 3) Kegels on her own 4) Pelvic floor physical therapy/biofeedback 5) Surgery 6) Tell her to wear a pad
 Urethral insert (Femsoft) 2) Pessary. 3) Kegels on her own. 4) Pelvic floor physical therapy/biofeedback. 5) Surgery. 6) Tell her to wear a pad.")
39
All are potential options, depending on how aggressive the patient wants to be with treatment

40
Squirting Sue First LineTreatment
1) Urethral insert (Femsoft) 2) Pessary 3) Kegels on her own 4) Pelvic floor physical therapy/biofeedback 5) Surgery 6) Tell her to wear a pad
 Urethral insert (Femsoft) 2) Pessary. 3) Kegels on her own. 4) Pelvic floor physical therapy/biofeedback. 5) Surgery. 6) Tell her to wear a pad.")
41
1) Urethral insert (Femsoft)
Answer 1) Urethral insert (Femsoft) DO NOT USE in pts with urinary tract infections or taking anticoagulants!
 Urethral insert (Femsoft) DO NOT USE in pts with urinary tract infections or taking anticoagulants!")
42
Urgency Ursula 70 yo c/o urinary incontinence with a strong urge, urgency, frequency. No incontinence with cough or stress manuevers. G0. PMH/PSH-Healthy. No surgeries. BMI 30. Medications/allergies-None. Labs-Urines and post void residual are normal. She has never been pregnant. Her past medical and surgical history are unremarkable, though she is overweight. No medications or allergies. Labs and post void residual are normal.

43
Urgency Ursula’s Physical Exam
This is what her vaginal mucosa looks like this

44
Urgency Ursula’s Physical Exam
This is what Ursula’s external genitalia looks like this.

45
Urgency Ursula’s Physical Exam
No prolapse or incontinence. Weak kegels. Otherwise, unremarkable. Her physical exam otherwise shows no prolapse or incontinence. She DOES have a weak pelvic floor. So ……. what can we look at next? (Pause) How about her voiding diary?
 How about her voiding diary")
46
Bladder diary This is Urgency Ursula’s bladder diary. Let‘s start by looking at the left which is the intake column. We see that she takes in a total of 48 ounces. Is that a normal daily fluid intake??? No, she should have around 60 oz daily for her age (60 and over I usually use). This is just a general guideline. This varies depending on the health and activity status of my patients of course. I also look at what types of fluids my patients take in. Is it generally water? Not in Ursula’s case. She only has 6 oz of water out of the 48 oz total.
. This is just a general guideline. This varies depending on the health and activity status of my patients of course. I also look at what types of fluids my patients take in. Is it generally water Not in Ursula’s case. She only has 6 oz of water out of the 48 oz total.")
47
Bladder diary Next I look at the output column. I look at her total output of 51 oz which coordinates nicely with he input of 48 oz, so there is no concern there. More importantly, though, I look at her individual voided volumes and her frequency. Are these normal voided volumes? Pause. No, they are not. 10oz voids would be normal. So we know so far that Ursula doesn’t drink enough daily fluid. She doesn’t drink enough water and instead takes in dietary irritants which we will discuss in an upcoming slide, and her voided volumes are small capacity voids. You probably are already formulating a diagnosis based on this information. Smile

48
Bladder diary It is helpful to know how much time the patient has between voids. I say if the patient is voiding every 2 hours during the day, this is normal provided she is taking in a normal fluid intake.

49
Bladder diary I then focus my attention to the right hand column which describes the patient’s urinary incontinence. I look at the frequency of the incontinence, how much she is leaking, what activities provoke it if any, if there’s urgency before she leaks and.. How many pads she wears during the day AND night.

50
Urgency Ursula What is her diagnosis? 1) Stress incontinence
2) Urge incontinence 3) Mixed incontinence and atrophic vaginitis 4) Overflow incontinence 5) Urge incontinence and atrophic vaginitis
 Urge incontinence. 3) Mixed incontinence and atrophic vaginitis. 4) Overflow incontinence. 5) Urge incontinence and atrophic vaginitis.")
51
5) Urge incontinence and atrophic vaginitis
Urgency Ursula Answer 1) Stress incontinence 2) Urge incontinence 3) Mixed incontinence and atrophic vaginitis 4) Overflow incontinence 5) Urge incontinence and atrophic vaginitis
 Stress incontinence. 2) Urge incontinence. 3) Mixed incontinence and atrophic vaginitis. 4) Overflow incontinence. 5) Urge incontinence and atrophic vaginitis.")
52
Urgency Ursula Treatment
1) Pelvic floor physical therapy 2) Vaginal estrogen 3) Dietary irritant avoidance 4) Weight loss 5) All of the above How will we treat Ursula?
 Pelvic floor physical therapy. 2) Vaginal estrogen. 3) Dietary irritant avoidance. 4) Weight loss. 5) All of the above. How will we treat Ursula")
53
Urgency Ursula’s Treatment Answer
1) Pelvic floor physical therapy 2) Vaginal estrogen 3) Dietary irritant avoidance 4) Weight loss 5) All of the above The answer is number 5-all of the above
 Pelvic floor physical therapy. 2) Vaginal estrogen. 3) Dietary irritant avoidance. 4) Weight loss. 5) All of the above. The answer is number 5-all of the above.")
54
Treatment Overactive Bladder
Behavioral Modification Fluid management Avoid Bladder Irritants Pelvic Floor Muscle Strengthening (Consider PT) Urge Suppression/ Awareness Of Triggers Bladder Retraining/ Timed Voiding Improve Mobility and Coexisting Health Issues Bowel Habits/ Regularity Since Ursula had an overactive bladder-let’s look at this chart that shows various treatments of OAB. You can see there are many. Behavioral modification plays a big role in improving overactive bladders. In my department, we have special folders with a lot of helpful information that not only we review as providers, but have our urogynecology nurses re-enforce the teaching.
 Urge. Suppression/ Awareness. Of Triggers. Bladder. Retraining/ Timed. Voiding. Improve. Mobility and. Coexisting. Health Issues. Bowel. Habits/ Regularity. Since Ursula had an overactive bladder-let’s look at this chart that shows various treatments of OAB. You can see there are many. Behavioral modification plays a big role in improving overactive bladders. In my department, we have special folders with a lot of helpful information that not only we review as providers, but have our urogynecology nurses re-enforce the teaching.")
55
What are dietary irritants?
The 6 C’s Caffeine Citrus Carbonation Vitamin C Alcohol (Cocktails) Cigarettes
 Cigarettes.")
56
Urgency Ursula returns 3 months later
Overactive bladder symptoms are no better. She has faithfully followed all recommendations. Vaginal tissue – improved Normal BMI. 4 sessions PT completed. Moderate kegel. Bladder diary-same except for no longer taking in dietary irritants. Unfortunately, Ursula’s symptoms are the same despite following our recommendations. She has estrogenized her vaginal tissue, lost weight, completing pelvic floor physical therapy, and avoided the 6 C’s.

57
Urgency Ursula’s return treatment?
1) Anticholinergics 2) Surgery 3) Continue with conservative therapy as the treatment risks outweigh the benefits 4) Pessary Explain why to not use pessary with atrophic tissue and wont’ work for urgency Surgery is not recommended for urgency until you fail medications
 Anticholinergics. 2) Surgery. 3) Continue with conservative therapy as the treatment risks outweigh the benefits. 4) Pessary. Explain why to not use pessary with atrophic tissue and wont’ work for urgency. Surgery is not recommended for urgency until you fail medications.")
58
Urgency Ursula’s return treatment answer
1) Anticholinergics 2) Surgery 3) Continue with conservative therapy as the above treatments risks outweigh the benefits 4) Pessary I would start her on medication. Even with her age, it is fine to use. And continue with # 3
 Anticholinergics. 2) Surgery. 3) Continue with conservative therapy as the above treatments risks outweigh the benefits. 4) Pessary. I would start her on medication. Even with her age, it is fine to use. And continue with # 3.")
59
Distribution of Muscarinic Receptors in Target Organs of the Parasympathetic Nervous System
Iris/Ciliary Body = Blurred Vision CNS Lacrimal Gland = Dry Eyes Salivary Glands = Dry Mouth Dizziness Somnolence Impaired Memory & Cognition Heart = Tachycardia Gall Bladder Stomach = Dyspepsia This slides shows the distribution of muscarinic receptors and is important because by remembering this distribution you can easily recall most of the common SE associated with this class of agents. Muscarinic receptors in the brain are associated in memory deficits and somnolence Lacrimal glands: Blurred vision Salivary glands: Dry mouth (the most common SE with this class of drugs) Heart: Receptors in the SA can cause increase in baseline HR and prolongation of the QT interval GI tract: constipation: the second most common SE Presence in the bladder accounts for the therapeutic benefit of this class of drugs. Colon = Constipation Bladder (detrusor muscle) Abrams P, Wein AJ. (1998). The Overactive Bladder: A Widespread and Treatable Condition. Erik Sparre Medical AB.
 Heart: Receptors in the SA can cause increase in baseline HR and prolongation of the QT interval. GI tract: constipation: the second most common SE. Presence in the bladder accounts for the therapeutic benefit of this class of drugs. Colon = Constipation. Bladder (detrusor muscle) Abrams P, Wein AJ. (1998). The Overactive Bladder: A Widespread and Treatable Condition. Erik Sparre Medical AB.")
60
Available anticholinergics
Oxybutynin tablet (Ditropan IR, ER) transdermal patch (Oxytrol)-which is OTC transdermal gel (Gelnique) Tolterodine tartrate (Detrol, IR, ER) Trospium chloride (Sanctura, IR, XR) Fesoterodine fumarate (Toviaz) Darifenacin (Enablex) Solifenacin succinate (Vesicare) Mirabegron (Myrbetriq) 7 different anticholinergics available on the market Myrebetriq is the newest one-only FDA approved Beta 3 adrenergic agonist. Comes in 25 and 50mg tablets. Most common SE was HTN at 11% in trials.
 transdermal patch (Oxytrol)-which is OTC. transdermal gel (Gelnique) Tolterodine tartrate (Detrol, IR, ER) Trospium chloride (Sanctura, IR, XR) Fesoterodine fumarate (Toviaz) Darifenacin (Enablex) Solifenacin succinate (Vesicare) Mirabegron (Myrbetriq) 7 different anticholinergics available on the market. Myrebetriq is the newest one-only FDA approved Beta 3 adrenergic agonist. Comes in 25 and 50mg tablets. Most common SE was HTN at 11% in trials.")
61
Which one to chose? In general, you could start with any one.
OBJECT trial, Mayo Clinic Proceedings, 2001 Oxybutynin ER/ Ditropan XL 10mg daily Good efficacy, reasonable cost If not effective or side effects Try another

62
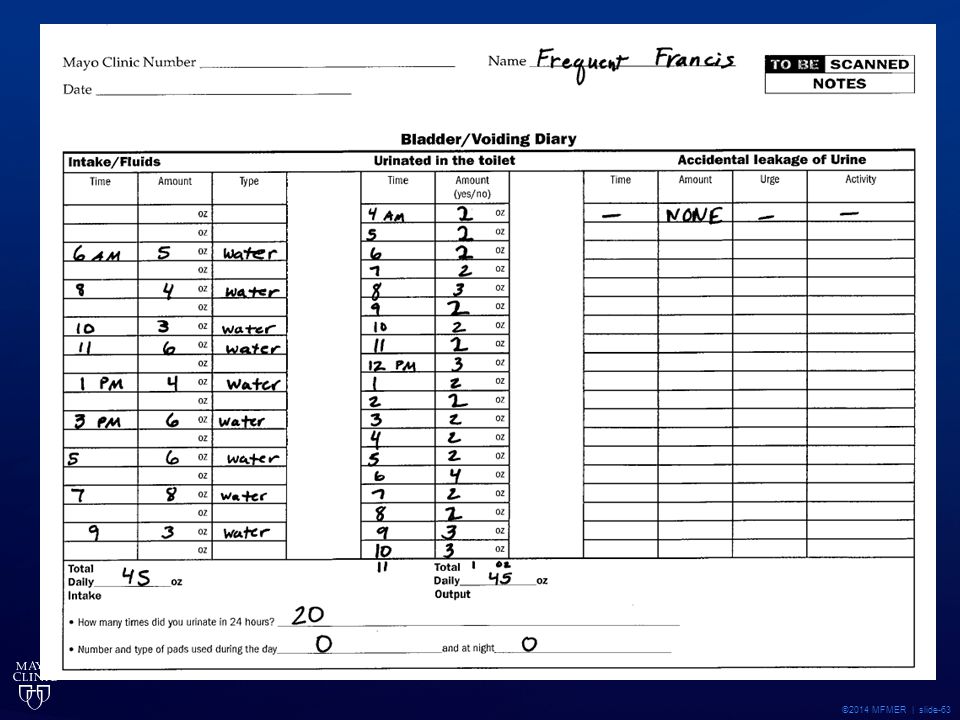
Frequent Francis 50 yo G0 c/o urinary frequency. Failed Tolterodine tartrate (Detrol LA), Fesoterodine fumarate (Toviaz), and Solifenacin succinate (Vesicare). Not interested in trying another medication. No dietary irritants. BMI 23. PMH/PSH- healthy. No meds/allergies. Labs-urines normal. Exam-normal with strong kegels. Add a slide for a bladder diary
, Fesoterodine fumarate (Toviaz), and Solifenacin succinate (Vesicare). Not interested in trying another medication. No dietary irritants. BMI 23. PMH/PSH- healthy. No meds/allergies. Labs-urines normal. Exam-normal with strong kegels. Add a slide for a bladder diary.")
64
Frequent Francis’s diagnosis
Urinary urgency Urinary frequency Obstructive voiding symptoms Urge incontinence

65
Frequent Francis’s diagnosis
Urinary urgency Urinary frequency Obstructive voiding symptoms Urge incontinence

66
Frequent Francis’s Treatment
1) Oxybutynin ER 10mg daily 2) Botox 3) Sacral Nerve Stimulator 4) Augmentation Cystoplasty 5) Refer This really affects franscis . She is at her wits end, so surgery may truly improve her quality of life. She is willing to even do major surgery she tells you.
 Oxybutynin ER 10mg daily. 2) Botox. 3) Sacral Nerve Stimulator. 4) Augmentation Cystoplasty. 5) Refer. This really affects franscis . She is at her wits end, so surgery may truly improve her quality of life. She is willing to even do major surgery she tells you.")
67
Frequent Francis’s Treatment
1) Oxybutynin ER 10mg daily 2) Botox 3) Sacral Nerve Stimulator 4) Augmentation Cystoplasty 5) Refer
 Oxybutynin ER 10mg daily. 2) Botox. 3) Sacral Nerve Stimulator. 4) Augmentation Cystoplasty. 5) Refer.")
68
Botulinum Toxin Many uses in the medical field today
Outpatient surgery injected cystoscopically Effective within 2 weeks Effective for 6-12 months Around 80% success Small chance of urinary retention $$$$ so we always ask pt to get insurance pre- approval

69
Treatment Urinary Urge Incontinence
Surgical Options: Sacral Neuromodulation (Interstim) Uses a small device (battery) which sends electrical impulses through a lead positioned close to S3 sacral nerve Modulates the nervous signals to the bladder TENS unit, percutaneous posterior tibial nerve stimulation, interstim
 Uses a small device (battery) which sends electrical impulses through a lead positioned close to S3 sacral nerve. Modulates the nervous signals to the bladder. TENS unit, percutaneous posterior tibial nerve stimulation, interstim.")
70
Wet Wanda 57 yo c/o urinary incontinence with urgency (larger volume leakage) and stress activities (small drops). She has constipation. No other complaints. G2, P2 (forceps with first, largest birth weight 9lbs). BMI 28 PMH/PSH- Hysterectomy, DM2, HTN Medications- Estradiol TD (Vivelle Dot), Metformin, HCTZ Allergies-NKDA SH: Drinks 1 pot of coffee daily and has 3 sodas. Smokes 1 pack of cigarettes daily x 25 years. Urines and post void residual are normal. Wanda is 57. She leaks urine with an urgency beforehand as well as when she coughs, sneezes, or does activity. She’s had 2 vaginal deliveries. Forceps assisted her first one who weighed 9lbs. She is overweight. She loves coffee and drinks 1 pot per day. She has 3 daily sodas and is a smoker. There is no urinary tract infection and she empties her bladder well.
 and stress activities (small drops). She has constipation. No other complaints. G2, P2 (forceps with first, largest birth weight 9lbs). BMI 28. PMH/PSH- Hysterectomy, DM2, HTN. Medications- Estradiol TD (Vivelle Dot), Metformin, HCTZ. Allergies-NKDA. SH: Drinks 1 pot of coffee daily and has 3 sodas. Smokes 1 pack of cigarettes daily x 25 years. Urines and post void residual are normal. Wanda is 57. She leaks urine with an urgency beforehand as well as when she coughs, sneezes, or does activity. She’s had 2 vaginal deliveries. Forceps assisted her first one who weighed 9lbs. She is overweight. She loves coffee and drinks 1 pot per day. She has 3 daily sodas and is a smoker. There is no urinary tract infection and she empties her bladder well.")
71
Wet Wanda Physical exam- Normal external genitalia. Normal vaginal mucosa. Weak kegels. No prolapse. With cough, leaks small amount. While getting off the exam table, she had a strong urge and gushed a larger amount of urine.

72
Wet Wanda’s diagnosis 1) Stress incontinence 2) Urge incontinence
3) Mixed incontinence 4) Overflow incontinence What is her diagnosis? Remember she leaked all over the exam table.
 Mixed incontinence. 4) Overflow incontinence. What is her diagnosis Remember she leaked all over the exam table.")
73
Wet Wanda diagnosis answer
1) Stress incontinence 2) Urge incontinence 3) Mixed incontinence 4) Overflow incontinence
 Stress incontinence. 2) Urge incontinence. 3) Mixed incontinence. 4) Overflow incontinence.")
74
How do you treat mixed incontinence?
Do you treat the stress or urge first? Ask the patient what bothers her most Treat the most bothersome symptom first For Wet Wanda, she is most bothered by her urinary urge incontinence So then how would we treat her if she has both?

75
Wet Wanda’s first treatment
1) Take her off the HCTZ and do a sling surgery 2) Pessary 3) Anticholinergics 4) Conservative management- avoid constipation, lose weight, avoid dietary/social irritants-smoking, soda, coffee.. 5) Who knows? So would you..
 Take her off the HCTZ and do a sling surgery. 2) Pessary. 3) Anticholinergics. 4) Conservative management- avoid constipation, lose weight, avoid dietary/social irritants-smoking, soda, coffee.. 5) Who knows So would you..")
76
Wet Wanda’s answer 1) Take her off the HCTZ and do a sling surgery 2) Pessary 3) Anticholinergics 4) Conservative management- avoid constipation, lose weight, avoid dietary/social irritants-smoking, soda, coffee.. 5) Who knows? . Let’s look at each of these options carefully and discuss them. She leaked urine on exam physical exam, but I wouldn’t jump right to a sling. I also don’t discontinue medications that I haven’t prescribed. She had no prolapse, so I wouldn’t use a pessary. She DOES have stress incontinence, but also urge and I have not seen pessaries help with urge incontinence. Anticholinergics are an option for this patient, but..its always best to start conservatively. 4 is the best answer. Referral to a nutritionist. Miralax for her constipation. Behavioral therapy through my urogyn nurses for dietary irritant avoidance and smoking cessation clinic here at Mayo.
 Conservative management- avoid constipation, lose weight, avoid dietary/social irritants-smoking, soda, coffee.. 5) Who knows . Let’s look at each of these options carefully and discuss them. She leaked urine on exam physical exam, but I wouldn’t jump right to a sling. I also don’t discontinue medications that I haven’t prescribed. She had no prolapse, so I wouldn’t use a pessary. She DOES have stress incontinence, but also urge and I have not seen pessaries help with urge incontinence. Anticholinergics are an option for this patient, but..its always best to start conservatively. 4 is the best answer. Referral to a nutritionist. Miralax for her constipation. Behavioral therapy through my urogyn nurses for dietary irritant avoidance and smoking cessation clinic here at Mayo.")
77
Obesity Obesity-it’s a growing problem-LITERALLY

78
Does weight loss help incontinence?
Program to Reduce Incontinence by Diet and Exercise (PRIDE) January New England Journal of Medicine 338 women 30 and older with a BMI of 25-50 greater than 3 months incontinence leaking at least 10 times/week 6 month weight loss program and followed for 18 months [18,19] Has anyone heard of the PRIDE study? The PRIDE study stands for Program to Reduce Incontinence by Diet and Exercise. The New England Journal of Medicine was first to publish this in Jan. 2009, September Journal of Urology, August Obstetrics & Gynecology This was a really neat and helpful study for urinary incontinent patients.
 January New England Journal of Medicine women. 30 and older with a BMI of greater than 3 months incontinence leaking at least 10 times/week. 6 month weight loss program and followed for 18 months [18,19] Has anyone heard of the PRIDE study The PRIDE study stands for Program to Reduce Incontinence by Diet and Exercise. The New England Journal of Medicine was first to publish this in Jan. 2009, September Journal of Urology, August Obstetrics & Gynecology. This was a really neat and helpful study for urinary incontinent patients.")
79
PRIDE, continued.. Group 1-”intensive” weight loss group had diet, exercise, behavioral modification with coaches, classes, etc.. And a follow up 12 month weight maintenance program Group 2-received information on diet and exercise with NO direct training to help them change habits [18,19]

80
PRIDE, continued… Group 1- Lost an average of 8% (about 17lbs) of their body weight Investigators reported a 47% mean reduction of weekly incontinent episodes Group 2- Lost an average of 1.6% (about 3lbs) of their body weight Investigators reported a 28% mean reduction in weekly incontinent episodes [19]
 of their body weight. Investigators reported a 28% mean reduction in weekly incontinent episodes [19]")
81
Wet Wanda returns 3 months later…
She is 50% improved from her urge incontinence, has stopped smoking, lost weight to now a normal BMI, no more constipation. She is interested in more aggressive treatment options. She’s improved by 50% and is happy about that, but would like to be dry.

82
Wet Wanda returns 3 months later…
Treatment options.. 1) Haven’t we fixed her yet? She’s still leaking? 2) Anticholinergics 3) Pessary 4) Surgery
 Haven’t we fixed her yet She’s still leaking 2) Anticholinergics. 3) Pessary. 4) Surgery.")
83
Wet Wanda returns 3 months later…
Treatment options.. 1) Haven’t we fixed her yet? She’s still leaking? 2) Anticholinergics 3) Pessary 4) Surgery
 Haven’t we fixed her yet She’s still leaking 2) Anticholinergics. 3) Pessary. 4) Surgery.")
84
Wet Wanda returns 2 months later..
Good news! You fixed Wanda’s urge incontinence! It is gone! She has now joined a Crossfit class and has had to stop it due to her bothersome incontinence with these Crossfit exercises. She has been so pleased with your care of fixing her urge incontinence, that she is confident in your ability to fix her stress urinary incontinence.

85
Wet Wanda’s treatment for stress incontinence
1) Urethral insert (Femsoft) 2) Pessary 3) Surgery
 Urethral insert (Femsoft) 2) Pessary. 3) Surgery.")
86
Answer Any option is reasonable.
I would present all options to the patient and let her decide as there is no wrong answer.

87
Treatment Stress Urinary Incontinence
Ring with a Knob Pessary Marland Pessary

88
Pessary care Patient self maintenance preferred
Removed twice weekly to clean with soap/water Some use only with activity Inserted with a water based lubricant Removed before intercourse Last usually around 10 years Around $80 each

89
Leaking Liz 37 yo G2, P2 (NSVD) female who leaks with plyometrics which incorporates a lot of jumping. Femsoft worked for her intermittent incontinence (early 20s). Continent pessary worked well from 36-37yo. Now interested in a more permanent fix. Healthy. Normal BMI. No meds/allergies. Unremarkable PMH/PSH. Normal exam with strong kegels.
. Continent pessary worked well from 36-37yo. Now interested in a more permanent fix. Healthy. Normal BMI. No meds/allergies. Unremarkable PMH/PSH. Normal exam with strong kegels.")
90
Leaking Liz treatments
1) Bulking agent 2) Slings
 Bulking agent. 2) Slings.")
91
Leaking Liz treatments
1) Bulking agent 2) Slings ***Pt to talk with surgeon to decide correct procedure for her. One size does not fit all. Recovery time versus anesthesia time
 Bulking agent. 2) Slings. ***Pt to talk with surgeon to decide correct procedure for her. One size does not fit all. Recovery time versus anesthesia time.")
92
Surgical treatment for stress incontinence
Outpatient surgery Bulking agents Periurethral injection of material (collagen, macroplastique, etc..) to increase tissue bulk. Slings Piece of material (like a hammock) inserted transvaginally supporting the urethra. Goal is to reduce stress incontinence without causing obstructive voiding symptoms or urinary retention.
 to increase tissue bulk. Slings. Piece of material (like a hammock) inserted transvaginally supporting the urethra. Goal is to reduce stress incontinence without causing obstructive voiding symptoms or urinary retention.")
93
References 1. Resnick NM, Yalla SV: Geriatric incontinence and voiding dysfunction. In: Campbell-Walsh Urology (9th Edition). Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA (Eds). Saunders Elsevier, PA, USA, 2305– 2321 (2005). 2. Herzog AR, Fultz NH: Prevalence and incidence of urinary incontinence in community-dwelling populations. J. Am. Geriatr. Soc. 38(3), 273–281 (1990). 3. Resnick NM: Urinary incontinence in the elderly. Med. Grand Rounds 3, 281–290 (1984). •• Original article suggesting 'delirium, infection, atrophy, pharmaceuticals, excess urine output, restricted mobility, stool impaction' (DIAPERS) mnemonic for transient causes of urinary incontinence in the elderly. 4. Matthews CA, Whitehead WE, Townsend MK, Grodstein F: Risk factors for urinary, fecal, or dual incontinence in the Nurses' Health Study. Obstet Gynecol. 2013;122(3):539. 5. Branch LG, Walker LA, Wetle TT, DuBeau CE, Resnick NM: Urinary incontinence knowledge among community-dwelling people 65 years of age and older. J Am Geriatr Soc. 1994;42(12):1257. 6. Buckley BS, Lapitan MC: Epidemiology Committee of the Fourth International Consultation on Incontinence, Paris, 2008: Prevalence of urinary incontinence in men, women, and children--current evidence: findings of the Fourth International Consultation on Incontinence. Urology. 2010;76(2):265. 7. Markland AD, Richter HE, Fwu CW, Eggers P, Kusek JW: Prevalence and trends of urinary incontinence in adults in the United States, 2001 to J Urol. 2011;186(2):589.
. Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA (Eds). Saunders Elsevier, PA, USA, 2305– 2321 (2005). 2. Herzog AR, Fultz NH: Prevalence and incidence of urinary incontinence in community-dwelling populations. J. Am. Geriatr. Soc. 38(3), 273–281 (1990). 3. Resnick NM: Urinary incontinence in the elderly. Med. Grand Rounds 3, 281–290 (1984). •• Original article suggesting delirium, infection, atrophy, pharmaceuticals, excess urine output, restricted mobility, stool impaction (DIAPERS) mnemonic for transient causes of urinary incontinence in the elderly. 4. Matthews CA, Whitehead WE, Townsend MK, Grodstein F: Risk factors for urinary, fecal, or dual incontinence in the Nurses Health Study. Obstet Gynecol. 2013;122(3): Branch LG, Walker LA, Wetle TT, DuBeau CE, Resnick NM: Urinary incontinence knowledge among community-dwelling people 65 years of age and older. J Am Geriatr Soc. 1994;42(12): Buckley BS, Lapitan MC: Epidemiology Committee of the Fourth International Consultation on Incontinence, Paris, 2008: Prevalence of urinary incontinence in men, women, and children--current evidence: findings of the Fourth International Consultation on Incontinence. Urology. 2010;76(2): Markland AD, Richter HE, Fwu CW, Eggers P, Kusek JW: Prevalence and trends of urinary incontinence in adults in the United States, 2001 to J Urol. 2011;186(2):589.")
94
References continued 8. Nygaard I, et. al. Pelvic Floor Disorders Network: Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008;300(11):1311. 9. Offermans MP et al. Prevalence of urinary incontinence and associated risk factors in nursing home residents: a systematic review. Neurourol Urodyn 2009; 28:288. 10. Burgio KL, Zyczynski H, Locher JL, et al. Urinary incontinence in the 12-month postpartum period. Obstet Gynecol 2003; 102:1291. 11. Brown JS, Vittinghoff E, Wyman JF, et al. Urinary incontinence: does it increase risk for falls and fractures? Study of Osteoporotic Fractures Research Group. J Am Geriatr Soc 2000; 48:721. 12. DuBeau CE, Kuchel GA, Johnson T, et al.. Incontinence in the frail elderly. In: Incontinence, 4th ed., Abrams P, Cardozo L, Khoury S, Wein A. (Eds), Health Publications Ltd, Paris p.961. 13. Herzog AR, Diokno AC, Brown MB, et al. Urinary incontinence as a risk factor for mortality. J Am Geriatr Soc 1994; 42:264 14. Hu TW, Wagner TH, Bentkover JD, et al. Costs of urinary incontinence and overactive bladder in the United States: a comparative study. Urology 2004; 63:461. 15. Stothers L, Thom D, Calhoun E. Urologic diseases in America project: urinary incontinence in males-- demographics and economic burden. J Urol 2005; 173:1302. 16. Thom DH, Nygaard IE, Calhoun EA. Urologic diseases in America project: urinary incontinence in women- national trends in hospitalizations, office visits, treatment and economic impact. J Urol 2005; 173:1295.
: Offermans MP et al. Prevalence of urinary incontinence and associated risk factors in nursing home residents: a systematic review. Neurourol Urodyn 2009; 28: Burgio KL, Zyczynski H, Locher JL, et al. Urinary incontinence in the 12-month postpartum period. Obstet Gynecol 2003; 102: Brown JS, Vittinghoff E, Wyman JF, et al. Urinary incontinence: does it increase risk for falls and fractures Study of Osteoporotic Fractures Research Group. J Am Geriatr Soc 2000; 48: DuBeau CE, Kuchel GA, Johnson T, et al.. Incontinence in the frail elderly. In: Incontinence, 4th ed., Abrams P, Cardozo L, Khoury S, Wein A. (Eds), Health Publications Ltd, Paris p Herzog AR, Diokno AC, Brown MB, et al. Urinary incontinence as a risk factor for mortality. J Am Geriatr Soc 1994; 42: Hu TW, Wagner TH, Bentkover JD, et al. Costs of urinary incontinence and overactive bladder in the United States: a comparative study. Urology 2004; 63: Stothers L, Thom D, Calhoun E. Urologic diseases in America project: urinary incontinence in males-- demographics and economic burden. J Urol 2005; 173: Thom DH, Nygaard IE, Calhoun EA. Urologic diseases in America project: urinary incontinence in women- national trends in hospitalizations, office visits, treatment and economic impact. J Urol 2005; 173:1295.")
95
References continued.. 17. Coyne KS1, Economic burden of urgency urinary incontinence in the United States: a systematic review. J Manag Care Pharm Feb;20(2): 18. Subak LL, et. al. Weight loss to treat urinary incontinence in overweight and obese women. N Engl J Med Jan 29;360(5): 19. Wing RR, et. Al. Effect of weight loss on urinary incontinence in overweight and obese women:results at 12 and 18 months. Journal of Urology 2010 Sept;18(3): 20. Wing RR., et. Al. Improving urinary incontinence in overweight and obese women through modest weight loss. Obstetrics & Gynecology 2010 Aug;116(2 Pt 1):284-92 21. Coyne KS, Sexton CC, Irwin DE, et al. The impact of overactive bladder, incontinence and other lower urinary tract symptoms on quality of life, work productivity, sexuality and emotional well-being in men and women: results from the EPIC study. BJU Int 2008; 101:1388. 22.
: Subak LL, et. al. Weight loss to treat urinary incontinence in overweight and obese women. N Engl J Med Jan 29;360(5): Wing RR, et. Al. Effect of weight loss on urinary incontinence in overweight and obese women:results at 12 and 18 months. Journal of Urology 2010 Sept;18(3): Wing RR., et. Al. Improving urinary incontinence in overweight and obese women through modest weight loss. Obstetrics & Gynecology 2010 Aug;116(2 Pt 1): Coyne KS, Sexton CC, Irwin DE, et al. The impact of overactive bladder, incontinence and other lower urinary tract symptoms on quality of life, work productivity, sexuality and emotional well-being in men and women: results from the EPIC study. BJU Int 2008; 101:")
Similar presentations













 Grants Chapter 6.>")




 Motion Controller Design for A Class of Second-order Systems Center for Self-Organizing Intelligent.>")
>")