Download presentation
Presentation is loading. Please wait.

1
Mind the Gap: AF and the Evolving Strategies in Anticoagulation
In Cooperation with

2
Faculty Disclosures Fred M. Kusomoto, MD, FACC Mayo Clinic
Consulting Fees/Honoraria: Medtronic Ralph J. Verdino, MD, FACC University of Pennsylvania Consulting Fees/Honoraria: Biosense Webster; Biotronic, Inc.; Boston Scientific; Medtronic; St. Jude Medical; Zoll Officer, Director, Trustee or Other Fiduciary Role: LifeWatch, Inc.

3
Acknowledgement Boehringer Ingelheim Pharmaceuticals, Inc. is a Founding Sponsor for the Mind the Gap Forums.

4
“Atrial Fibrillation is the Low Back Pain of Cardiology.”
Mike Crawford

5
Program Objectives Upon completion of this session, attendees should be able to — Implement evidence-based anticoagulation regimens for atrial fibrillation patients based on individual risks and patients’ preferences Recognize common barriers associated with managing chronic anticoagulation in atrial fibrillation patients

6
Atrial Fibrillation (AF) in the U.S
2.2 million people have AF 3.3 million in 2020; 5.6 million by 2050 Above age 70: 10% incidence Lifetime risk: 25% Risk increases with increasing age Epidemiology of problem, stressing importance 6

7
Future of Atrial Fibrillation ATRIA Study
AF Forum: Management, Anticoagulation, and Stroke Prevention Projected Number of Adults With AF in the US 1995 to 2050 7.0 6.0 5.61 5.42 5.0 5.16 4.78 4.0 4.0 4.34 Adults With AF (millions) 3.80 Age- and sex-specific prevalence data from 1 study population were applied to US population census information to estimate the number of adults with AF through This study estimates that currently there are approximately 2.3 million adults in the United States with AF. The study also projects a 2.5-fold increase to more than 5.6 million adults with AF by the year Thus, AF is poised to present a public health crisis in the near future. 3.0 3.33 2.94 2.66 2.44 2.0 2.26 2.08 1.0 1990 1995 2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050 Year Go et al. JAMA. 2001;285; Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA. 2001;285:
 Age- and sex-specific prevalence data from 1 study population were applied to US population census information to estimate the number of adults with AF through This study estimates that currently there are approximately 2.3 million adults in the United States with AF. The study also projects a 2.5-fold increase to more than 5.6 million adults with AF by the year Thus, AF is poised to present a public health crisis in the near future Year. Go et al. JAMA. 2001;285; Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA. 2001;285:")
8
Prevalence Incidence Biennial rate/1000 person exams Age
Ann Int Med 1995 Biennial rate/1000 person exams Age Benjamin EJ JAMA 1994; Framingham Heart Study

9
Atrial Fibrillation in the U.S. (Cont.)
Risks/causative factors: HTN, DM, CHF, age, valvular heart disease, MI, pulmonary embolus, cardiomyopathy, pulmonary disease, hyperthyroidism Genetics: Most common in “Lone AF” Connexin-40 Potassium channels: KCNQ1, KCNE2, KCNJ2, KCNH2 ANF peptide frame shift mutation 9

11
Atrial Fibrillation (AF) and Stroke
Stroke is the most common and devastating complication of AF1,2 Incidence of all-cause stroke in patients with AF is 5%1 AF is an independent risk factor for stroke2 Approximately 15% of all strokes in the US are caused by AF3 1. Fuster V, et al. Circulation. 2006;114:e 2. Benjamin EJ, et al. Circulation. 1998;98: 3. Lloyd-Jones D, et al. Circulation. 2009;119:e

12
Stroke Rates in Placebo-Treated Patients With AF*
In a meta-analysis of 16 trials that included a total of 9874 patients with nonvalvular AF, Hart et al sought to characterize the efficacy of anticoagulant and antiplatelet agents. The trials in this slide constitute the 6 warfarin trials in the meta-analysis that assessed warfarin versus aspirin or placebo. The studies included a total of 2900 patients across the 6 trials. The mean age was 69 years and approximately 20% of patients were older than 75. Illustrated here are the high rates of stroke in patients not treated with anticoagulant therapy. Across all studies, stroke rates were higher in AF patients who were not on warfarin. AFASAK reported 5.7% of placebo patients having a stroke compared with 2.7% in the warfarin group. The same reductions were true for SPAF (9.0% vs 3.8%), BAATAF (6.3% vs 1.4%), CAFA (4.7% vs 3.2%), SPINAF (7.9% vs 2.5%) and the secondary-prevention trial EAFT (23.4% vs 8.9%). Overall, warfarin reduced the risk of stroke by 2.7% per year for primary prevention and 8.4% per year for secondary prevention. Overall relative risk reduction was 62%. AFASAK SPAF BAATAF CAFA SPINAF EAFT† *This represents patients who are not anticoagulated; †Secondary prevention. Hart et al. Ann Intern Med. 1999;131: Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta-analysis. Ann Intern Med. 1999;131:
, BAATAF (6.3% vs 1.4%), CAFA (4.7% vs 3.2%), SPINAF (7.9% vs 2.5%) and the secondary-prevention trial EAFT (23.4% vs 8.9%). Overall, warfarin reduced the risk of stroke by 2.7% per year for primary prevention and 8.4% per year for secondary prevention. Overall relative risk reduction was 62%. AFASAK. SPAF. BAATAF. CAFA. SPINAF. EAFT† *This represents patients who are not anticoagulated; †Secondary prevention. Hart et al. Ann Intern Med. 1999;131: Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta-analysis. Ann Intern Med. 1999;131:")
13
Atrial Fibrillation and Stroke (Cont.)
Risk of stroke increases with age1 Ischemic stroke associated with AF is often more severe than stroke of other etiologies4 Stroke risk persists even in asymptomatic AF5 Asymptomatic AF implicated as a cause of cryptogenic stroke6 4. Dulli DA, et al. Neuroepidemiology. 2003;22: 5. Page RL, et al. Circulation. 2003;107:1141-5 6. Bhatt A, et al. Stroke Res Treat. 2011; 2011: 1-5

14
CHADS2 Congestive heart failure Hypertension Age >75 years
Diabetes mellitus Prior Stroke or TIA (*2 points) Is the putative risk high and how good is the data for factors not included? A general schema for assessing stroke risk but should be modified as needed by clinical judgement CHADS score did not include all risk factors Of those other risk factors ( female gender, thyrotoxicosis, LA size, etc. ) How compelling is the data for each of them. CHADS2 score may not tell the whole story in each patient and clinical judgment comes into play and may need to be emphasized. Gage, BF, et al. JAMA. 2001;285:
 Is the putative risk high and how good is the data for factors not included A general schema for assessing stroke risk but should be modified as needed by clinical judgement. CHADS score did not include all risk factors. Of those other risk factors ( female gender, thyrotoxicosis, LA size, etc. ) How compelling is the data for each of them. CHADS2 score may not tell the whole story in each patient and clinical judgment comes into play and may need to be emphasized. Gage, BF, et al. JAMA. 2001;285:")
15
Stroke Risk in AF ACP/AAFP Guidelines
CHADS2 Score Adjusted Stroke Rate* (95% CI) CHADS2 Risk Level 1.9 ( ) Low Aspirin 1 2.8 ( ) Low Aspirin/Warfarin 2 4.0 ( ) Moderate 3 5.9 ( ) Moderate 4 8.5 ( ) High Warfarin Warfarin was used here. This goes back to data that pre-dates the DTIs. Keep in mind the DTIs and Xa inhibitors. 5 12.5 ( ) High 6 18.2 ( ) High *Expected rate of stroke per 100 patient-years Snow V, et al. Ann Intern Med. 2003;139: 15 15
 CHADS2 Risk Level. 1.9 ( ) Low. Aspirin ( ) Low. Aspirin/Warfarin ( ) Moderate ( ) Moderate ( ) High. Warfarin. Warfarin was used here. This goes back to data that pre-dates the DTIs. Keep in mind the DTIs and Xa inhibitors ( ) High ( ) High. *Expected rate of stroke per 100 patient-years. Snow V, et al. Ann Intern Med. 2003;139:")
16
CHADS2 Congestive heart failure Hypertension Age >75 years
Diabetes mellitus Prior Stroke or TIA (*2 points) Is the putative risk high and how good is the data for factors not included? A general schema for assessing stroke risk but should be modified as needed by clinical judgement CHADS score did not include all risk factors Of those other risk factors ( female gender, thyrotoxicosis, LA size, etc. ) How compelling is the data for each of them. CHADS2 score may not tell the whole story in each patient and clinical judgment comes into play and may need to be emphasized. Gage, BF, et al. JAMA. 2001;285:
 Is the putative risk high and how good is the data for factors not included A general schema for assessing stroke risk but should be modified as needed by clinical judgement. CHADS score did not include all risk factors. Of those other risk factors ( female gender, thyrotoxicosis, LA size, etc. ) How compelling is the data for each of them. CHADS2 score may not tell the whole story in each patient and clinical judgment comes into play and may need to be emphasized. Gage, BF, et al. JAMA. 2001;285:")
17
CHADS2 Congestive heart failure Hypertension Age >75 years
Diabetes mellitus Prior Stroke or TIA (*2 points) CHADS2 did not consider other important risk factors: Female gender (not confirmed in all studies) Thyrotoxicosis LA size HOCM Valvular heart disease Is the putative risk high and how good is the data for factors not included? A general schema for assessing stroke risk but should be modified as needed by clinical judgement CHADS score did not include all risk factors Of those other risk factors ( female gender, thyrotoxicosis, LA size, etc. ) How compelling is the data for each of them. CHADS2 score may not tell the whole story in each patient and clinical judgment comes into play and may need to be emphasized. Gage, BF, et al. JAMA. 2001;285:
 CHADS2 did not consider other important risk factors: Female gender (not confirmed in all studies) Thyrotoxicosis. LA size. HOCM. Valvular heart disease. Is the putative risk high and how good is the data for factors not included A general schema for assessing stroke risk but should be modified as needed by clinical judgement. CHADS score did not include all risk factors. Of those other risk factors ( female gender, thyrotoxicosis, LA size, etc. ) How compelling is the data for each of them. CHADS2 score may not tell the whole story in each patient and clinical judgment comes into play and may need to be emphasized. Gage, BF, et al. JAMA. 2001;285:")
18
CHADS2 Lip et al Chest 2010

19
CHA2DS2-VASc Clinical Feature Points CHF 1 HTN Age ≥ 75 2
Diabetes mellitus Stroke, TIA, or embolism Female gender Age Vascular disease (prior MI, PVD, aortic plaque A refinement of CHADS2

20
CHADS2 vs. CHA2DS2-VASc Lip et al Chest 2010

21
ESC Guidelines for Antithrombotic Therapy
CHA2DS2VASc score Adjusted stroke rate (%/year) Recommended antithrombotic therapy ASA mg or no therapy. No therapy preferred 1 1.3 Either oral anticoagulation or ASA mg daily, anticoagulation preferred 2 2.2 Oral anticoagulation 3 3.2 4 4.0 5 6.7 6 9.8 7 9.6 8 9 15.2 Could give example of a 70 y.o. woman without other risk factors who by CHADS2 would get ASA but by CHA2DS2VAS2 would get warfarin. Europace 2010; 12:
 Recommended antithrombotic therapy. ASA mg or no therapy. No therapy preferred Either oral anticoagulation or ASA mg daily, anticoagulation preferred Oral anticoagulation Could give example of a 70 y.o. woman without other risk factors who by CHADS2 would get ASA but by CHA2DS2VAS2 would get warfarin. Europace 2010; 12:")
22
Stroke Prevention: Coumadin
Warfarin AFASAK BAATAF SPAF CAFA SPINAF Warfarin/ASA EAFT SPAF II AFASAK Foundation of current treatment recs.

25
Warfarin: Risk-Benefit Profile
20 Ischemic Stroke 15 Intracranial Bleeding Odds Ratio 10 5 Range applies to patients without mechanical prosthetic valves. Therapeutic range depends on patient upstraight. When INR falls below 2.0, you will see a very rapid rise in ischemic stroke. In terms of warfarin 2.0 is the magic number and there’s a big difference between 1.9 and 2.0 1 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 INR Fuster V, et al. Circulation. 2006;114:e

26
Warfarin and Drug Interactions
Warfarin is metabolized by the hepatic P450 enzyme CYP2C9 Warfarin concentration (and therefore INR) is increased by drugs that inhibit CYP2C9. INR must be closely followed and warfarin dosage decreased CYP2C9 inhibitors include: Amiodarone Statins simvastatin and rosuvastatin (not atorvastatin, pravastatin) Fibrates (fenofibrate, gemfibrozil) Antibiotics (sulfamethoxazole/trimethoprim, metronidazole) Azole antifungals (fluconazole, miconazole, voriconazole) Might also mention dietary factors.
 is increased by drugs that inhibit CYP2C9. INR must be closely followed and warfarin dosage decreased. CYP2C9 inhibitors include: Amiodarone. Statins simvastatin and rosuvastatin (not atorvastatin, pravastatin) Fibrates (fenofibrate, gemfibrozil) Antibiotics (sulfamethoxazole/trimethoprim, metronidazole) Azole antifungals (fluconazole, miconazole, voriconazole) Might also mention dietary factors.")
27
Warfarin and Drug Interactions (Cont.)
Drugs that induce CYP2C9: warfarin’s effectiveness is decreased, reducing INR - Rifampin Other drugs interactions not via CYP2C metabolism - Thyroid hormone For more information visit (Arizona CERT) or (Indiana University, Prof D.A. Flockhart)
 or (Indiana University, Prof D.A. Flockhart)")
28
Quality of Warfarin Control in AF Patients on Chronic Anticoagulation
63% 55% 51% Time Spent in Therapeutic INR Range (%) Our meta-analysis assessed 8 studies including a total of 14 groups involving 22,237 warfarin-treated AF patients with 41,199 years of follow-up. Atrial fibrillation patients in the 14 groups spent 55% (95% CI = 51%-58%) of their time within the therapeutic INR range. Of the 8 studies, 13 groups could be evaluated by setting: warfarin dosing was managed by anticoagulation clinics for 4 (31%) groups and by community (physician) practice, defined as usual care, for 9 (69%). Patients in anticoagulation clinics spent on average 63% (95% CI = 58%-68%) of their time in the therapeutic range versus 51% (95% CI = 47%-55%) for patients in community practice. Compared with an anticoagulation clinic, patients treated in the usual care (community) setting spent 11% (95% CI = 2%-20%, n = 6 studies) less time in therapeutic INR range. Only 48% of eligible patients in this analysis received warfarin Baker WL, et al. J Manag Care Pharm. 2009;15: 28
 Our meta-analysis assessed 8 studies including a total of 14 groups involving 22,237 warfarin-treated AF patients with 41,199 years of follow-up. Atrial fibrillation patients in the 14 groups spent 55% (95% CI = 51%-58%) of their time within the therapeutic INR range. Of the 8 studies, 13 groups could be evaluated by setting: warfarin dosing was managed by anticoagulation clinics for 4 (31%) groups and by community (physician) practice, defined as usual care, for 9 (69%). Patients in anticoagulation clinics spent on average 63% (95% CI = 58%-68%) of their time in the therapeutic range versus 51% (95% CI = 47%-55%) for patients in community practice. Compared with an anticoagulation clinic, patients treated in the usual care (community) setting spent 11% (95% CI = 2%-20%, n = 6 studies) less time in therapeutic INR range. Only 48% of eligible patients in this analysis received warfarin. Baker WL, et al. J Manag Care Pharm. 2009;15:")
29
Time Spent in Therapeutic INR Range and Clinical Outcomes
Groups stratified by time spent in therapeutic INR range ( ) All patients had a CHADS2 score ≥ 2 What alternatives can we have to warfarin? This is the last slide discussing eficacy of warfarin. Following slides will discuss alternatives. Morgan CL, et al. Thromb Res. 2009;124:37-41. 29
 All patients had a CHADS2 score ≥ 2. What alternatives can we have to warfarin This is the last slide discussing eficacy of warfarin. Following slides will discuss alternatives. Morgan CL, et al. Thromb Res. 2009;124:")
30
Warfarin in Eligible Patients ATRIA Study
% Use in Eligible Patients Warfarin has been shown to reduce the incidence of ischemic CVA in patients with nonvalvular AF. The ATRIA study’s objective was to evaluate rates and predictors of warfarin use in the outpatient population. It was a cross-sectional study of patients enrolled in a large California HMO. Among the 11,082 patients with AF and no contraindications to anticoagulation, only 55% were prescribed warfarin, and warfarin was nonlinearly associated with age. The lowest rates of warfarin use were noted in the youngest age group (age <55 years), 44.3%, and the oldest age group (age >85 years), 35.4%. The highest incidence of warfarin use was in the age 55 to 84 category (57.3%-60.7%). It should be noted that this percent of underuse represents the portion of the population considered eligible for anticoagulation. <55 55-64 65-74 75-84 85 Overall Age (years) Go et al. Ann Intern Med. 1999;131: Go AS, Hylek EM, Borowsky LH, et al. Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. Ann Intern Med. 1999;131:
, 44.3%, and the oldest age group (age >85 years), 35.4%. The highest incidence of warfarin use was in the age 55 to 84 category (57.3%-60.7%). It should be noted that this percent of underuse represents the portion of the population considered eligible for anticoagulation. < 85. Overall. Age (years) Go et al. Ann Intern Med. 1999;131: Go AS, Hylek EM, Borowsky LH, et al. Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. Ann Intern Med. 1999;131:")
31
Warfarin in Eligible Patients ATRIA Study
% Use in Eligible Patients Warfarin has been shown to reduce the incidence of ischemic CVA in patients with nonvalvular AF. The ATRIA study’s objective was to evaluate rates and predictors of warfarin use in the outpatient population. It was a cross-sectional study of patients enrolled in a large California HMO. Among the 11,082 patients with AF and no contraindications to anticoagulation, only 55% were prescribed warfarin, and warfarin was nonlinearly associated with age. The lowest rates of warfarin use were noted in the youngest age group (age <55 years), 44.3%, and the oldest age group (age >85 years), 35.4%. The highest incidence of warfarin use was in the age 55 to 84 category (57.3%-60.7%). It should be noted that this percent of underuse represents the portion of the population considered eligible for anticoagulation. <55 55-64 65-74 75-84 85 Overall Age (years) Go et al. Ann Intern Med. 1999;131: Go AS, Hylek EM, Borowsky LH, et al. Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. Ann Intern Med. 1999;131:
, 44.3%, and the oldest age group (age >85 years), 35.4%. The highest incidence of warfarin use was in the age 55 to 84 category (57.3%-60.7%). It should be noted that this percent of underuse represents the portion of the population considered eligible for anticoagulation. < 85. Overall. Age (years) Go et al. Ann Intern Med. 1999;131: Go AS, Hylek EM, Borowsky LH, et al. Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. Ann Intern Med. 1999;131:")
32
Cumulative Hazard Rates
ACTIVE-W: Warfarin vs. Dual Antiplatelet Therapy for Prevention of Cardiovascular Events Cumulative risk of primary composite endpointa Cumulative Hazard Rates RR = 1.44 ( ), P = Time (years) This section is alternatives to warfarin. Warfarin superior to dual anti-platelet therapy in patients who are warfarin candidates. aStroke, MI, non-CNS systemic embolism, or vascular death. ACTIVE Investigators. Lancet. 2006;367: 32
, P = Time (years) This section is alternatives to warfarin. Warfarin superior to dual anti-platelet therapy in patients who are warfarin candidates. aStroke, MI, non-CNS systemic embolism, or vascular death. ACTIVE Investigators. Lancet. 2006;367:")
33
Primary Composite Endpointa
ACTIVE-A: Dual Antiplatelet Therapy Reduces the Incidence of Vascular Events in AF When Warfarin Therapy Is “Unsuitable” Primary Composite Endpointa Stroke P = 0.01 P < 0.001 Cumulative Incidence “Unsuitable” in quotes – per Dr. Waldo, it was probably an overly generous use of the term in this study (50% physician determined and 25% patient preference). Point out difference between ACTIVE-A and ACTIVE-W. Time (years) Time (years) aStroke, MI, non-CNS systemic embolism, or vascular death. ACTIVE Investigators. N Engl J Med. 2009;360: 33
. Point out difference between ACTIVE-A and ACTIVE-W. Time (years) Time (years) aStroke, MI, non-CNS systemic embolism, or vascular death. ACTIVE Investigators. N Engl J Med. 2009;360:")
34
ACTIVE-A: Dual Antiplatelet Therapy Increases the Risk of Bleeding

35
2011 Focused Update Recommendation
Class IIb (New Recommendation) The addition of clopidogrel to aspirin (ASA) to reduce the risk of major vascular events, including stroke, might be considered in patients with AF in whom oral anticoagulation with warfarin is considered unsuitable due to patient preference or the physician’s assessment of the patient’s ability to safely sustain anticoagulation. (Level of Evidence: B) Single reference: ACTIVE A 2011 ACCF/AHA/HRS Focused Update on the Management of Patients with Atrial Fibrillation (Updating the 2006 Guideline). Circulation 2011;123:
 The addition of clopidogrel to aspirin (ASA) to reduce the risk of major vascular events, including stroke, might be considered in patients with AF in whom oral anticoagulation with warfarin is considered unsuitable due to patient preference or the physician’s assessment of the patient’s ability to safely sustain anticoagulation. (Level of Evidence: B) Single reference: ACTIVE A ACCF/AHA/HRS Focused Update on the Management of Patients with Atrial Fibrillation (Updating the 2006 Guideline). Circulation 2011;123:")
37
New Pharmacologic Approaches for Stroke Reduction in AF
Oral direct thrombin inhibitors Fixed-dose, no monitoring Dabigatran Oral factor Xa inhibitors Apixaban Edoxaban Rivaroxaban Dabigatran, a long-acting oral direct thrombin inhibitor that requires no monitoring, The oral factor Xa inhibitors, apixaban and rivaroxaban, can also be administered as a fixed-dose with no monitoring required. 37

38
Antithrombotic Therapy in Atrial Fibrillation
Antithrombotic Therapy in Atrial Fibrillation. Circulation 2011;75:

39
Direct Thrombin Inhibitors
Ximelagatran Tested in Stroke Prevention Using an Oral Thrombin Inhibitor in Atrial Fibrillation (SPORTIF) III (open label) and V (double blind) Ximelagatran as effective as warfarin with lower risk of bleeding Did not make it to market due to liver toxicity
 III (open label) and V (double blind) Ximelagatran as effective as warfarin with lower risk of bleeding. Did not make it to market due to liver toxicity.")
40
RE-LY: Randomized Evaluation of Long-term Anticoagulation Therapy
18,113 patients with atrial fibrillation randomized to dabigatran (110 mg or 150 mg twice daily) versus warfarin (INR target ) Mean CHADS2 score = 2.1 By intention-to-treat analysis dabigatran 110 mg was non-inferior (p < 0.001) while dabigatran 150 mg was superior( p<0.001) to warfarin INR was in the therapeutic range 64% of the time NEJM
 versus warfarin (INR target ) Mean CHADS2 score = 2.1. By intention-to-treat analysis dabigatran 110 mg was non-inferior (p < 0.001) while dabigatran 150 mg was superior( p<0.001) to warfarin. INR was in the therapeutic range 64% of the time. NEJM")
41
RE-LY “High risk” AF patients:
At least one of: Prior CVA or TIA LVEF < 40%; NYHA Class I or greater CHF Age >75 yrs Age and on of: DM HTN CAD Exclusions: “severe valve disease;” CVA <14 days or “severe CVA” <6 months; increased bleeding risk; active liver disease; CrCl <30; pregnancy

42
RE-LY: Dabigatran Reduces the Risk of Stroke in AF Patients
Cumulative Hazard Rate Time (months) Connolly SJ, et al. N Engl J Med. 2009;361:
 Connolly SJ, et al. N Engl J Med. 2009;361:")
43
RE-LY: Safety Outcomes with Dabigatran
Dabigatran 110 mg vs. Warfarin Dabigatran 150 mg Event RR (95% CI) P value Major bleeding 0.80 ( ) 0.003 0.93 ( ) 0.31 Life threatening 0.68 ( ) < 0.001 0.81 ( ) 0.04 Gastrointestinal bleeding 1.10 ( ) 0.43 1.50 ( ) Major or minor bleeding 0.78 ( ) 0.91 ( ) 0.002 Intracranial bleeding 0.31 ( ) 0.40 ( ) Modified from Connolly SJ, et al. N Engl J Med. 2009;361: 43
 P value. Major bleeding ( ) ( ) Life threatening ( ) < ( ) Gastrointestinal bleeding ( ) ( ) Major or minor bleeding ( ) 0.91 ( ) Intracranial bleeding ( ) 0.40 ( ) Modified from Connolly SJ, et al. N Engl J Med. 2009;361:")
44
FDA Approval for Dabigatran:
Dabigatran 150 was superior to warfarin and dabigatran 110 mg for stroke prevention; Dabigatran 150 mg was similar to warfarin for bleeding risk but inferior to dabigatran 110 mg. Among the elderly (40% of Re-Ly patients over age 75), thromboembolism risk was lower with dabi-150 than with dabi-110, but bleeding risk was higher. Because bleeding is “less undesirable” than stroke, dabi-110 not felt to be advantageous. Discuss QOL issues re. warfarin vs. dabigatran Beasley BN, Unger EF, Temple R. Anticoagulant Options – Why the FDA Approved a Higher but Not a Lower Dose of Dabigatran. NEJM 2011 (online first).
, thromboembolism risk was lower with dabi-150 than with dabi-110, but bleeding risk was higher. Because bleeding is less undesirable than stroke, dabi-110 not felt to be advantageous. Discuss QOL issues re. warfarin vs. dabigatran. Beasley BN, Unger EF, Temple R. Anticoagulant Options – Why the FDA Approved a Higher but Not a Lower Dose of Dabigatran. NEJM 2011 (online first).")
45
FDA Approval for Dabigatran: 75 mg q12h
Among pts with impaired renal function (CrCl 30-50), stroke risk for dabi-150 was 1/2 that of dabi-110 but bleeding risk was not higher. ==> dabi-110 was not felt to offer any advantage, and it was felt that most patients should receive the higher dosage. The decision to approve the 75 mg q12h dose was based on pharmacokinetic and pharmacodynamic modeling; there is no safety or efficacy data. Beasley BN, Unger EF, Temple R. Anticoagulant Options – Why the FDA Approved a Higher but Not a Lower Dose of Dabigatran. NEJM 2011 (online first).
, stroke risk for dabi-150 was 1/2 that of dabi-110 but bleeding risk was not higher. ==> dabi-110 was not felt to offer any advantage, and it was felt that most patients should receive the higher dosage. The decision to approve the 75 mg q12h dose was based on pharmacokinetic and pharmacodynamic modeling; there is no safety or efficacy data. Beasley BN, Unger EF, Temple R. Anticoagulant Options – Why the FDA Approved a Higher but Not a Lower Dose of Dabigatran. NEJM 2011 (online first).")
46
Antithrombotic Therapy in Atrial Fibrillation
Antithrombotic Therapy in Atrial Fibrillation. Circulation 2011;75:

47
Can point out different population in RELY and ROCKET-AF with respect to CHADS2 score.
Antithrombotic Therapy in Atrial Fibrillation. Circulation 2011;75:

48
Apixaban: AVERROES Trial
5599 patients with AF deemed “unsuitable” for warfarin randomized to apixaban (5mg twice daily) or aspirin (81-324mg daily) Primary endpoint: stroke or systemic embolism Trial terminated early due to superiority of apixaban Connolly et al. NEJM :
 or aspirin (81-324mg daily) Primary endpoint: stroke or systemic embolism Trial terminated early due to superiority of apixaban Connolly et al. NEJM :")
49
ROCKET-AF: Rivaroxaban for the Prevention of Stroke and Non-CNS Embolism
14,264 patients with atrial fibrillation randomized to rivaroxaban (20mg once daily) versus warfarin (INR target 2.5) Mean CHADS2 score = 3.5 By intention-to-treat analysis rivaroxaban was non-inferior (p < ) but not superior ( p =0.12) to warfarin INR was in the therapeutic range only 55 percent of the time Currently before the FDA for AF indication Safety: overall similar bleeding rates with less life-threatening (fatal or intracranial) hemorrhage Once daily dosing with half-life 5-13 hours and no monitoring Clearance: 1/3 renal, 2/3 by P450 enzymes Could point out the non-inferiority vs. superiority issue. Rivaroxaban was non-inferior by intention-to-treat and per protocol analysis. By per protocol without protocol violations it was superior. Intention-to-treat considered gold standard and therefore non-inferior. Factor Xa inhibition ROCKET-AF and AVVEROES are not FDA approved agents and are NOT on the market in the US. Do NOT discuss using these agents during the cases as they would not be applicable and would be off label!! NEJM
 versus warfarin (INR target 2.5) Mean CHADS2 score = 3.5. By intention-to-treat analysis rivaroxaban was non-inferior (p < ) but not superior ( p =0.12) to warfarin. INR was in the therapeutic range only 55 percent of the time. Currently before the FDA for AF indication. Safety: overall similar bleeding rates with less life-threatening (fatal or intracranial) hemorrhage. Once daily dosing with half-life 5-13 hours and no monitoring. Clearance: 1/3 renal, 2/3 by P450 enzymes. Could point out the non-inferiority vs. superiority issue. Rivaroxaban was non-inferior by intention-to-treat and per protocol analysis. By per protocol without protocol violations it was superior. Intention-to-treat considered gold standard and therefore non-inferior. Factor Xa inhibition. ROCKET-AF and AVVEROES are not FDA approved agents and are NOT on the market in the US. Do NOT discuss using these agents during the cases as they would not be applicable and would be off label!! NEJM")
50
2011 ACCF/AHA/HRS Focused Update on the Management of Patients with Atrial Fibrillation (Update on Dabigatran) Emphasize contraindication for prosthetic valves and renal and liver failure

51
Chronic paroxysmal AF patient managed by a primary care physician with a moderately-high bleeding risk. The patient is currently only on aspirin.

53
Case 1 – 76-year-old Female with Dyspnea
Chronic paroxysmal AF patient managed by a primary care physician with a moderately-high bleeding risk. The patient is currently only on aspirin.

54
HPI PMH Shortness of breath and DOE for several months
Denies palpitations, chest pain, or dizziness PMH Obesity, diabetes, HTN, chronic kidney disease, hyperlipidemia, DJD Does not smoke or drink Meds: diltiazem, celecoxib, metformin, pravastatin

55
PE Data VS: BP 164/92, HR 94 CV: irregularly irregular, no murmurs
ECG: atrial fibrillation with controlled VR, LVH by voltage BUN/Cr: 36/2.1, other labs incl LFTs nl CXR: mild cardiomegaly, o/w normal Stress echo: nl LV function, mild LVH, no sig valve dz, no ischemia

56
Question What is her risk of stroke? High (~8-18%) Medium (~4-6%)
c) Low (~2-3%)
 Low (~2-3%)")
57
Stroke Risk in AF ACP/AAFP Guidelines
CHADS2 Score Adjusted Stroke Rate* (95% CI) CHADS2 Risk Level 1.9 ( ) Low Aspirin 1 2.8 ( ) Low Aspirin/Warfarin 2 4.0 ( ) Moderate 3 5.9 ( ) Moderate 4 8.5 ( ) High Warfarin 5 12.5 ( ) High 6 18.2 ( ) High *Expected rate of stroke per 100 patient-years Snow V, et al. Ann Intern Med. 2003;139: 57 57
 CHADS2 Risk Level. 1.9 ( ) Low. Aspirin ( ) Low. Aspirin/Warfarin ( ) Moderate ( ) Moderate ( ) High. Warfarin ( ) High ( ) High. *Expected rate of stroke per 100 patient-years. Snow V, et al. Ann Intern Med. 2003;139:")
58
CHA2DS2-VASc Clinical Feature Points CHF 1 HTN Age ≥ 75 2
Diabetes mellitus Stroke, TIA, or embolism Female gender Age Vascular disease (prior MI, PVD, aortic plaque)
")
59
ESC Guidelines for Antithrombotic Therapy
CHA2DS2VASc score Adjusted stroke rate (%/year) Recommended antithrombotic therapy ASA mg or no therapy. No therapy preferred 1 1.3 Either oral anticoagulation or ASA mg daily, anticoagulation preferred 2 2.2 Oral anticoagulation 3 3.2 4 4.0 5 6.7 6 9.8 7 9.6 8 9 15.2 Europace 2010; 12:
 Recommended antithrombotic therapy. ASA mg or no therapy. No therapy preferred Either oral anticoagulation or ASA mg daily, anticoagulation preferred Oral anticoagulation Europace 2010; 12:")
60
Question What is her risk of bleeding with anticoagulation? High
Medium Low

61
HAS-BLED Score Clinical Feature Points SBP ≥ 160 mmHg 1 Abnormal renal function Abnormal liver function Prior CVA Bleeding Labile INRs Age > 65 Taking antiplatelets/NSAIDs Alcohol intake Clinically tied to CHADS-VASC, but not exernally validated. HAS-BLED score ≥3 indicates increased one year risk of intracranial bleed, bleed requiring hospitalization, or drop in hemoglobin ≥2gm/L or requiring transfusion.

62
HAS-BLED score in the SPORTIF cohort
% Gregory Y. H. Lip, MD,* Lars Frison, PHD,† Jonathan L. Halperin, MD,‡ Deirdre A. Lane, PHD* Birmingham, England; Mölndal, Sweden; and New York, New York Objectives The purpose of this study was to investigate predictors of bleeding in a cohort of anticoagulated patients and to evaluate the predictive value of several bleeding risk stratification schemas. Background The risk of bleeding during antithrombotic therapy in patients with atrial fibrillation (AF) is not homogeneous, and several clinical risk factors have been incorporated into clinical bleeding risk stratification schemas. Current risk stratification schemas for bleeding during anticoagulation therapy have been based on complex scoring systems that are difficult to apply in clinical practice, and few have been derived and validated in AF cohorts. Methods We investigated predictors of bleeding in a cohort of 7,329 patients with AF participating in the SPORTIF (Stroke Prevention Using an ORal Thrombin Inhibitor in Atrial Fibrillation) III and V clinical trials and evaluated the predictive value of several risk stratification schemas by multivariate analysis. Patients were anticoagulated orally with either adjusted-dose warfarin (target international normalized ratio 2 to 3) or fixed-dose ximelagatran 36 mg twice daily. Major bleeding was centrally adjudicated, and concurrent aspirin therapy was allowed in patients with clinical atherosclerosis. Results By multivariate analyses, significant predictors of bleeding were concurrent aspirin use (hazard ratio [HR]: 2.10; 95% confidence interval [CI]: 1.59 to 2.77; p ); renal impairment (HR: 1.98; 95% CI: 1.42 to 2.76; p ); age 75 years or older (HR: 1.63; 95% CI: 1.23 to 2.17; p ); diabetes (HR: 1.47; 95% CI: 1.10 to 1.97; p 0.009), and heart failure or left ventricular dysfunction (HR: 1.32; 95% CI: 1.01 to 1.73; p ). Of the tested schemas, the new HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score performed best, with a stepwise increase in rates of major bleeding with increasing HAS-BLED score (ptrend ). The c statistic for bleeding varied between 0.50 and 0.67 in the overall entire cohort and 0.68 among patients naive to warfarin at baseline (n 769). Conclusions This analysis identifies diabetes and heart failure or left ventricular dysfunction as potential risk factors for bleeding in AF beyond those previously recognized. Of the contemporary bleeding risk stratification schemas, the new HASBLED scheme offers useful predictive capacity for bleeding over previously published schemas and may be simpler to apply. (J Am Coll Cardiol 2011;57:173–80) © 2011 by the American College of Cardiology Foundation Score Lip et al JACC 2011
 is not homogeneous, and several clinical risk factors have been incorporated into clinical bleeding risk stratification schemas. Current. risk stratification schemas for bleeding during anticoagulation therapy have been based on complex scoring systems. that are difficult to apply in clinical practice, and few have been derived and validated in AF cohorts. Methods We investigated predictors of bleeding in a cohort of 7,329 patients with AF participating in the SPORTIF (Stroke. Prevention Using an ORal Thrombin Inhibitor in Atrial Fibrillation) III and V clinical trials and evaluated the predictive. value of several risk stratification schemas by multivariate analysis. Patients were anticoagulated orally. with either adjusted-dose warfarin (target international normalized ratio 2 to 3) or fixed-dose ximelagatran. 36 mg twice daily. Major bleeding was centrally adjudicated, and concurrent aspirin therapy was allowed in. patients with clinical atherosclerosis. Results By multivariate analyses, significant predictors of bleeding were concurrent aspirin use (hazard ratio [HR]: 2.10; 95% confidence interval [CI]: 1.59 to 2.77; p 0.001); renal impairment (HR: 1.98; 95% CI: 1.42 to 2.76; p 0.001); age 75 years or older (HR: 1.63; 95% CI: 1.23 to 2.17; p ); diabetes (HR: 1.47; 95% CI: 1.10 to 1.97; p ), and heart failure or left ventricular dysfunction (HR: 1.32; 95% CI: 1.01 to 1.73; p 0.041). Of the tested. schemas, the new HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score performed best, with a stepwise increase in rates of major. bleeding with increasing HAS-BLED score (ptrend ). The c statistic for bleeding varied between 0.50 and in the overall entire cohort and 0.68 among patients naive to warfarin at baseline (n 769). Conclusions This analysis identifies diabetes and heart failure or left ventricular dysfunction as potential risk factors for bleeding. in AF beyond those previously recognized. Of the contemporary bleeding risk stratification schemas, the new HASBLED. scheme offers useful predictive capacity for bleeding over previously published schemas and may be simpler. to apply. (J Am Coll Cardiol 2011;57:173–80) © 2011 by the American College of Cardiology Foundation. Score. Lip et al JACC")
63
What is her risk of stroke/bleeding?
Question What is her risk of stroke/bleeding? CHADS2 score=3 (annual stroke risk=5.9%) CHADS2VASc=5 (annual stroke risk=6.7%) 3. HASBLED score=4 (annual bleeding risk=5.6%)
 CHADS2VASc=5 (annual stroke risk=6.7%) 3. HASBLED score=4 (annual bleeding risk=5.6%)")
64
Question Which anticoagulation regimen is most appropriate for her?
Aspirin Warfarin Dabigatran 75mg twice daily Dabigatran 150 mg twice daily Aspirin/clopidogrel

65
AF and Strokes 15% of ischemic strokes are due to cardioemboli => 75,000 events/year 45% of cardioemboli are due to atrial fibrillation Risk of stroke 5-7x increased in patients with atrial fibrillation 65

66
Which Anticoagulation Regimen is Most Appropriate for Her?
Peter Loewen-Vancouver Coastel Health

67
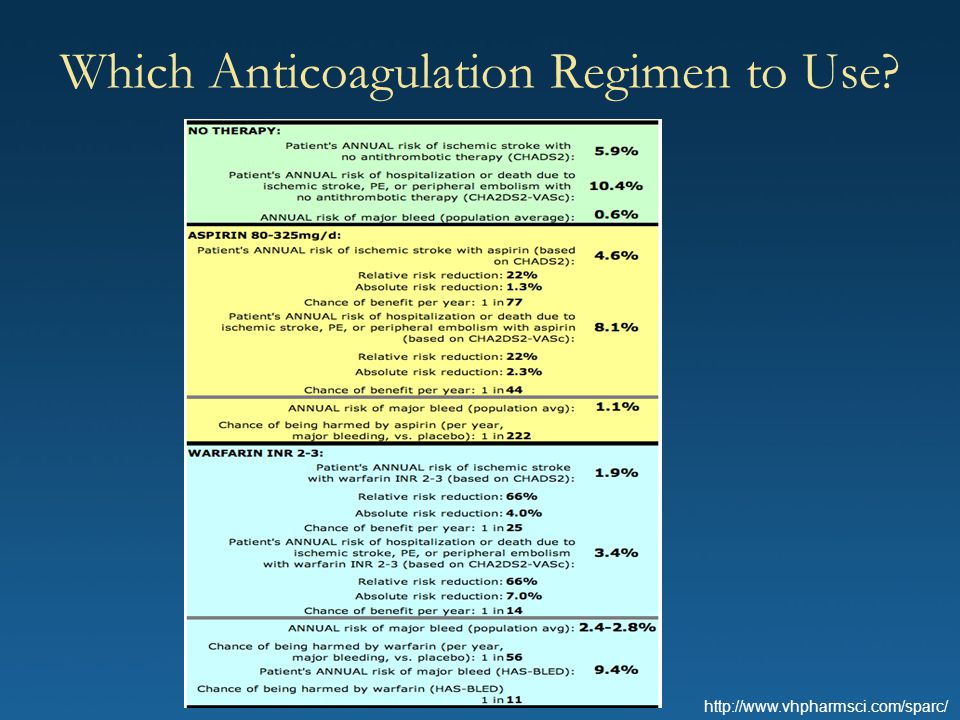
Which Anticoagulation Regimen to Use?
68
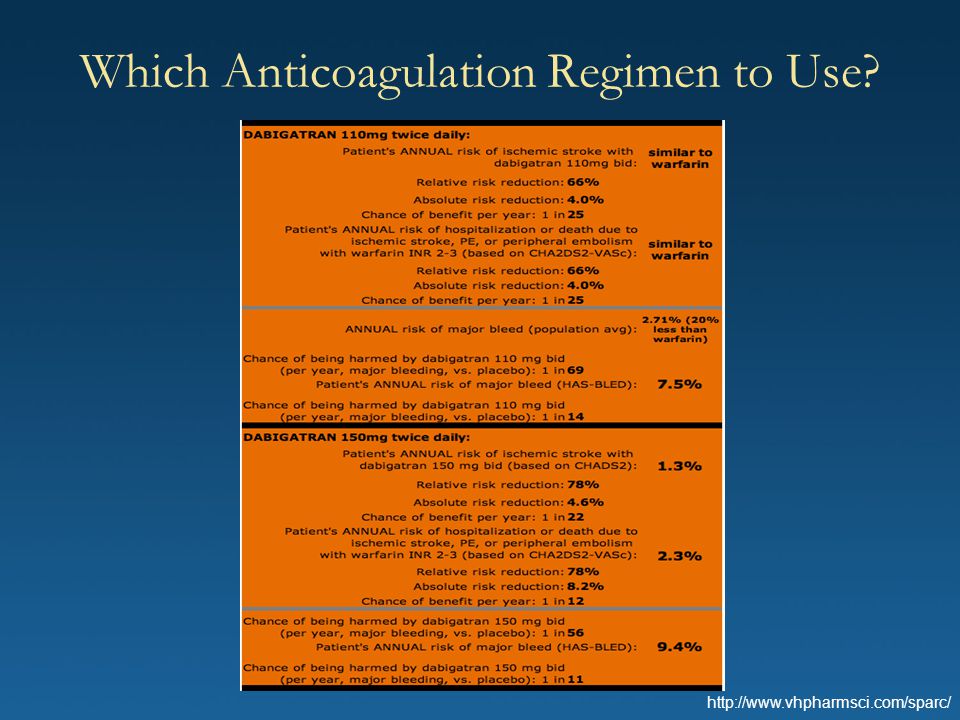
Which Anticoagulation Regimen to Use?
69
Case 1 Teaching Points When using oral anticoagulants, balancing the risks of bleeding vs the risks of stroke can be difficult. Scoring systems that predict risk (CHADS2, CHA2DS2Vasc, HASBLED) can help with decision making.
 can help with decision making.")
70
Questions and Answers

71
Case 2 – 59-year-old Man Presents with Acute Chest Pain
Discussion of triple vs. dual therapy and various agents. Good review in JACC article on importance of triple therapy and why it’s needed with some patients A post-PCI patient with significant ischemic disease, NYHA class III heart failure and atrial fibrillation. The patient is currently on clopidogrel and aspirin, in addition to standard HF therapies.

72
Past History - 10 years ago first diagnosed with hypertension - 5 years ago acute inferior MI Cath showed - 95% RCA % LAD % OM1 Underwent CABG x month f/u - EF 40% by echo with inferior and posterior severe hypokinesia

73
Past History (Cont.) - 4 years ago nuclear stress showed EF 35-40%, inferior and posterior scar without ischemia diminished functional status - 6 months ago maintained on Lisinopril 40 mgqd, Carvedilol 20 q12h, Aspirin 81mgqd, Simvastatin 40 mgqd, NYHA Class III CHF symptoms - 3 months ago presented on OV with atrial fibrillation with controlled rate; warfarin begun What is the risk of stroke? What are anticoagulation options currently?

74
Present Coronary Anatomy
Native coronaries % RCA % prox LAD % OM % proximal LCx stenosis - Patent LIMA and LAD, graft to PDA Occluded graft to OM Placed on clopidogrel full dose aspirin and underwent PCI of LCx with bare metal stent

75
Question What would you do next?
a) Continue warfarin indefinitely with aspirin, clopidogrel for one year b) Substitute dabigatran with aspirin, clopidogrel for one year c) Stop warfarin, aspirin and clopidogrel for one month and resume warfarin d) Stop warfarin, aspirin and clopidogrel for one month then add dabigatran
 Continue warfarin indefinitely with aspirin, clopidogrel for one year b) Substitute dabigatran with aspirin, clopidogrel for one year c) Stop warfarin, aspirin and clopidogrel for one month and resume warfarin d) Stop warfarin, aspirin and clopidogrel for one month then add dabigatran.")
76
Bleeding and Mortality in a Danish Registry after MI
Triple Rx: Bleeding and Mortality in a Danish Registry after MI Sorensen et al Lancet 2009

77
Question What would you do next?
a) Continue warfarin indefinitely with aspirin, clopidogrel for one year b) Substitute dabigatran with aspirin, clopidogrel for one year c) Stop warfarin, aspirin and clopidogrel for one month and resume warfarin d) Stop warfarin, aspirin and clopidogrel for one month then add dabigatran
 Continue warfarin indefinitely with aspirin, clopidogrel for one year b) Substitute dabigatran with aspirin, clopidogrel for one year c) Stop warfarin, aspirin and clopidogrel for one month and resume warfarin d) Stop warfarin, aspirin and clopidogrel for one month then add dabigatran.")
78
Guidelines for the Management of Atrial Fibrillation
Guidelines for the Management of Atrial Fibrillation. European Heart Journal 2010; 31:

79
Guidelines for the Management of Atrial Fibrillation
Guidelines for the Management of Atrial Fibrillation. European Heart Journal 2010; 31:

80
Stent Thrombosis vs. Bleeding vs. Stroke
Risk Management: Stent Thrombosis vs. Bleeding vs. Stroke Faxon et al Hemostasis and Thrombosis 2011.

81
Managing Risk Stent Thrombosis Discontinuing DAPT
Procedural: TIMI < 3, Discontinuing DAPT, residual dissection, bifurcations stents, incomplete stent apposition, stent length, proximal dz Patient: Malignancy, diabetes, renal failure Bleeding HAS-BLED Stroke CHADS2 or CHA2DS2-VASc

82
Stent Thrombosis vs. Bleeding vs. Stroke
Risk Management: Stent Thrombosis vs. Bleeding vs. Stroke Faxon et al Hemostasis and Thrombosis 2011.

83
Randomized Trials on Triple Therapy
ISAR-TRIPLE: 600 patients after DES will be randomized to either a short course (6 weeks) or long course (6 months), followed by aspirin and warfarin. 1°: Composite of death, MI, definite stent thrombosis, or major bleeding at 9 months WOEST: 496 patients randomized oral anticoagulation and clopidogrel or triple therapy. 1°: Bleeding at 1 year MUSICA-2: 304 patients (CHADS≤ 2) randomized to DAPT or triple Rx
 or long course (6 months), followed by aspirin and warfarin. 1°: Composite of death, MI, definite stent thrombosis, or major bleeding at 9 months. WOEST: 496 patients randomized oral anticoagulation and clopidogrel or triple therapy. 1°: Bleeding at 1 year. MUSICA-2: 304 patients (CHADS≤ 2) randomized to DAPT or triple Rx.")
84
Case 2 Teaching Points Choose BMS if patient will require anti-thrombotic therapy long term Presentation with ACS implies that patient should ideally be treated with dual anti-platelet therapy for 1 year but needs to be judged relative to bleeding risk Data on triple therapy is limited No data on dabigitran in this setting and nothing in guidelines

85
Questions and Answers

86
Mind the Gap: Summary Atrial fibrillation is going to become more common Stroke is the most devastating complication of atrial fibrillation Old and new options Managing patients in “real life” is difficult

88
Case 3 – 80-year-old Male with Renal Cell Cancer
Bridging in afib patients Peri-operative management Who do we bridge and how do we bridge? What INR do you go to? What’s an appropriate level of anticoagulation? What should be your target INR? What kinds of procedures need bridges? Bleeding complications?

89
HPI Renal cell cancer recently diagnosed Nephrectomy is planned Urologic surgeon requests peri-op cardiac management PMH Permanent atrial fibrillation for > 5 years, managed with metoprolol and warfarin Meds: metoprolol, warfarin, lisinopril, pravastatin, aspirin

90
Physical Exam VS: BP 134/68, HR 78 irreg irreg CV: irregularly irregular, no murmurs Data ECG: atrial fibrillation with controlled VR INR 2.3

91
Question In preparation for surgery, you should:
Admit the patient to the hospital, stop warfarin and administer IV heparin until the morning of surgery Stop warfarin 5 days prior to surgery and initiate LMWH until the morning of surgery Stop warfarin 5 days prior to surgery without bridging anticoagulation Following discontinuation of warfarin, should the patient’s anticoagulation be bridged with heparin? What are the risks of thromboembolism if heparin is not administered? What are the risks of bleeding if heparin is administered? Is it appropriate to use enoxaparin? What if he were taking dabigatran instead?

92
Risks Associated with Temporary Discontinuation of Warfarin
After warfarin is stopped, it takes about 4 days for the INR to reach 1.5. Once the INR is 1.5 surgery can be safely performed. Therefore, if warfarin is held 4 days before surgery and treatment is started as soon as possible after surgery, patients can be expected to have a subtherapeautic INR for two days before and two days after surgery.

93
ACC/AHA/ESC 2006 Guidelines for Perioperative Management of Atrial Fibrillation
Anticoagulation may be interrupted for a period of up to one week for surgery. In high risk patients (prior stroke, TIA, or systemic embolism) unfractionated or low-molecular-weight heparin may be used.
 unfractionated or low-molecular-weight heparin may be used.")
94
ACCP 8th Edition Evidence-Based Clinical Practice Guidelines: Managing Non-therapeutic INRs
For patients with INRs of ≥ 5.0 but < 9.0 and no significant bleeding: Omit the next one or two doses of warfarin Monitor more frequently Resume therapy at an appropriately adjusted dose when the INR is at a therapeutic level (Grade 1C) Alternatively, omit a dose and administer 1 to 2.5 mg oral vitamin K, particularly if the patient is at increased risk of bleeding (Grade 2A) Barriers to anticoagulation – difficulty maintaining therapeutic inr (too low or too high) Ansell J, et al. Chest. 2008;133:160S-98S.
 Alternatively, omit a dose and administer 1 to 2.5 mg oral vitamin K, particularly if the patient is at increased risk of bleeding (Grade 2A) Barriers to anticoagulation – difficulty maintaining therapeutic inr (too low or too high) Ansell J, et al. Chest. 2008;133:160S-98S.")
95
Peri-operative Management of Dabigatran
With normal kidney function, miss two doses of dabigatran before surgery. With impaired kidney function, miss 3-4 doses of dabigatran before surgery. If surgery carries a high risk of bleeding, consider stopping dabigatran 2 days before surgery with normal renal function and 3-5 days with impaired renal function.

96
a) Initiate a rhythm control drug b) Discharge on beta-blocker alone
Question a) Initiate a rhythm control drug b) Discharge on beta-blocker alone What would you do?
 Initiate a rhythm control drug b) Discharge on beta-blocker alone. What would you do")
97
Case 3 Teaching Points Most patients, unless they have had prior stroke, TIA, or systemic embolism do not require bridging of anticoagulation. Warfarin can be stopped for 5 days prior to surgery while dabigatran can be stopped just 1-2 days prior to surgery.

Similar presentations