Download presentation
Presentation is loading. Please wait.

1
ANATOMICAL FACTS AND MANAGEMENT GUIDELINES
OFFICE ORTHOPAEDICS ANATOMICAL FACTS AND MANAGEMENT GUIDELINES

2
THE NON-SPECIFIC ACHES AND PAIN SYNDROMES
COMMONEST Low back pain Interscapular pain Shoulder pain Anterior knee pain Multiple bony pains

3
LESS COMMON PAINFUL AREAS
Elbow Heel and back of ankle Wrist, first carpometacarpal joint Neck Coccyx

4
Your bones reflect what you eat and what you do for a lifetime
Your bones reflect what you eat and what you do for a lifetime! (Nutrition and activity are the key points of musculoskeletal health.)
")
5
ALL ACHES AND PAINS DIRECTLY RELATED TO
1.Lifetime and current status of nutrition ( Poor nutrition related pains) (obesity related pains) 2.Lifetime and current status of physical activity 3.Medical illness/Psychological make up
 (obesity related pains) 2.Lifetime and current status of physical activity. 3.Medical illness/Psychological make up.")
6
EFFECTS OF THE THREE FACTORS-favourable/unfavourable
Long standing alteration in the strength and mechanics of the bones, joints and muscles. range of movement of joints. Changes in the attitude towards physical activity (‘ I can’t move’)
")
7
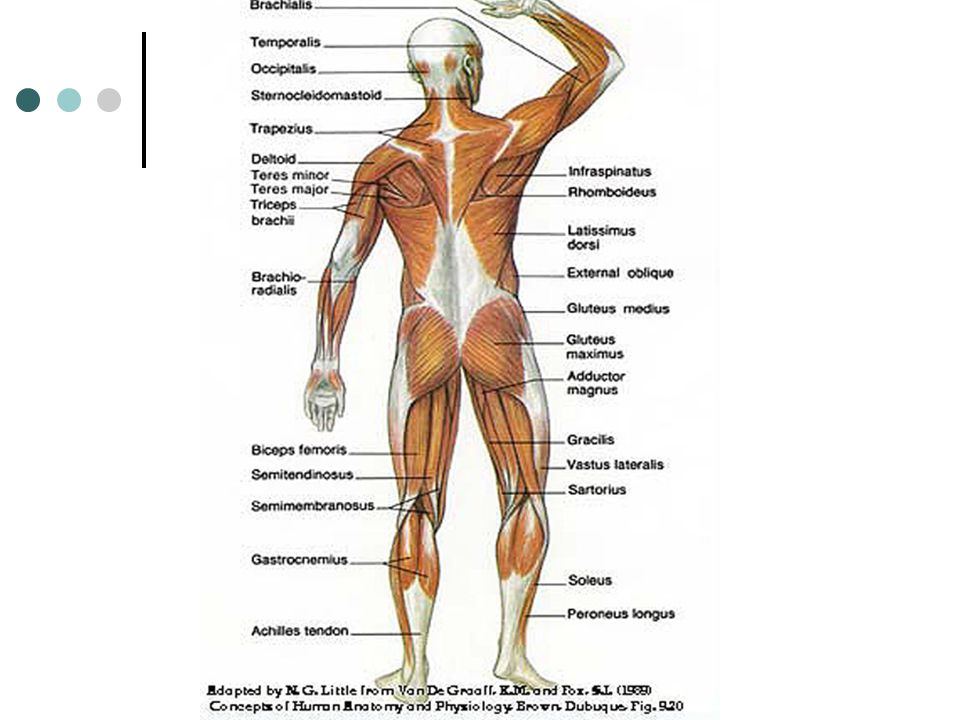
Understanding the basic muscle development
The upright human posture has best of extensors developed as compared to the quadrupeds. All placed on the dorsal side except quadriceps and tibialis anterior. Need active, full and lifetime use to prevent disuse and loss of ROM of concerned joints

8
Flexor pollicis longus
KEY MUSCLES OF UPPER LIMB Trapezius Levator scapulae The rhomboids Extensors of the wrist Flexor pollicis longus Abductor pollicis longus and extensor pollicis brevis

9
Key muscles of non specific aches and pains
BACK and LOWER LIMB Erector spinae Gluteus maximus Rectus femoris Vastus medialis Tendo achilis

10
THE COMMON FACTOR Remember the motor milestones of a child? Flexors are fetal muscles,extensors develop later from head to toe.(Neck holding to tiptoe standing) If you do not use ALL extensors daily, fully, they can cause pain due to disuse and subsequent fibrosis.
 If you do not use ALL extensors daily, fully, they can cause pain due to disuse and subsequent fibrosis.")
11
PATHOLOGY OF FIBROSIS Normal healing response,leading to scar formation. NOT a part of normal aging or degeneration. BUT can occur due to disuse of joints and muscles. Loss of intermediate gliding tissue planes due to fibrosis.

12
Pathophysiology of stiffness/contracture
Disuse- obliteration of gliding planes- fibrosis of intermediate ‘white’ tissues i.e.loose areolar tissue, joint capsule, ligaments, tendons, fascia etc.- Gradual loss of mobility- permanent stiffness RED tissue does not lead to contracture by itself

13
WHAT ABOUT DEGENERATION?
Natural aging process is NOT painful normally. Lifestyle throughout the life makes it painful. Diet and activity related. Contractures are not normal with age.

14
WHAT IS SPONDYLOSIS AND OSTEOARTHROSIS?
Symptom complex originating from a combination of factors including aging But not solely blamed on aging Radiological changes only? ‘Dustbin diagnosis’ for aches and pains

15
When to consider radiological degeneration really seriously?
A) In the spine- When it shows OBJECTIVE neural signs ( Cervical spondylotic myelopathy, Lumbar canal stenosis)and gross malalingment.
 In the spine- When it shows OBJECTIVE neural signs ( Cervical spondylotic myelopathy, Lumbar canal stenosis)and gross malalingment.")
16
Contd. B) In other joints- When it causes MECHANICAL MALALIGNMENT of the joint( Scoliosis, kyphosis,Genu varum, Planovalgus foot, Hallux valgus etc.)
 In other joints- When it causes MECHANICAL MALALIGNMENT of the joint( Scoliosis, kyphosis,Genu varum, Planovalgus foot, Hallux valgus etc.) .")
17
Clinical or radiological entity?
Changes in the alignment of a joint make it painful. Localized sclerosis an indirect indicator. Osteophytes alone are NOT a cause of pain. Careful correlation needed between symptoms and x-ray findings. Mostly mismatching.

18
TWO BROAD CATEGORIES OF PATIENTS
1.Nutritionally low, manual worker or housewife with multiple pregnancies. 2.Well to do, well-fed, comfort loving urban patient living a mechanized life.

19
NOTE BEFORE EXAMINATION
Is it a child? Adult?Old person?Male? Female? Where does the pt come from? Urban area? Rural area? hilly area? What has been the occupation of the patient? Play? Sports?Table work?Manual work? housewife?Machine worker? computer worker?

20
What is the patient’s social/nutritional status?
What is the duration of complaints? Any relation to the obstretic history in case of a young female pt? Alcoholic? Medical illness? Diabetic? On steroids? Already treated and no relief? What is most difficult to do?

21
TRY TO ASSESS Mentality of the patient-
Doctor should give a medicine that works like magic! Investigate me by all possible modalities including MRI I am a very sick patient and cannot improve. I can do anything that you tell me.

22
DIFFERENTIATE THE SINISTER FROM THE NON SPECIFIC PAINS
‘NO FINDINGS, ONLY PAIN’ Early sign of an infection or a pathological fracture? Missing a significant injury? Deep seated neoplasm? Reflection of a medical condition?

23
Low back pain Commonest problem in office orthopedics faced by adults.
Sinister in children and adolescents. Most confusing symptom for decision making.

24
THE first look examination
SPEND TIME ON INSPECTION Show me how you walk. Can you hold your arms up in the air? Look up to the ceiling.

25
The Real Physical examination
All back and lower limb patients must be examined first standing and then made to lie down. Upper limbs, neck and hands can be examined with the patient sitting and you standing at the back of the patient.

26
The Standing patient Flat back Hyperlordotic curve
CURVES OF THE BACK (especially the lumbar curve) Flat back Hyperlordotic curve Kyphotic dorsal spine Scoliotic list Prominence of sacrococcygeal junction
 Flat back. Hyperlordotic curve. Kyphotic dorsal spine. Scoliotic list. Prominence of sacrococcygeal junction.")
27
What Importance is to the curve?
Major cause of mechanical back pain Indicative of inner problems like acute or chronic disc prolapse Developmental anomalies of the spine

28
Functions of the spinal curves
Spring loading effect in vertical posture- not a loaded pillar. Permits elongation and shortening of the stature to some extent. Acts like a shock absorber for every activity

29
The Evolution of The Back- Theirs and Ours
The primitive back- A loading surface on four pillars. No axial loading. Very stable design Permits speed in mobility Compromised mobility of the spine per se. No true vertical posture.

30
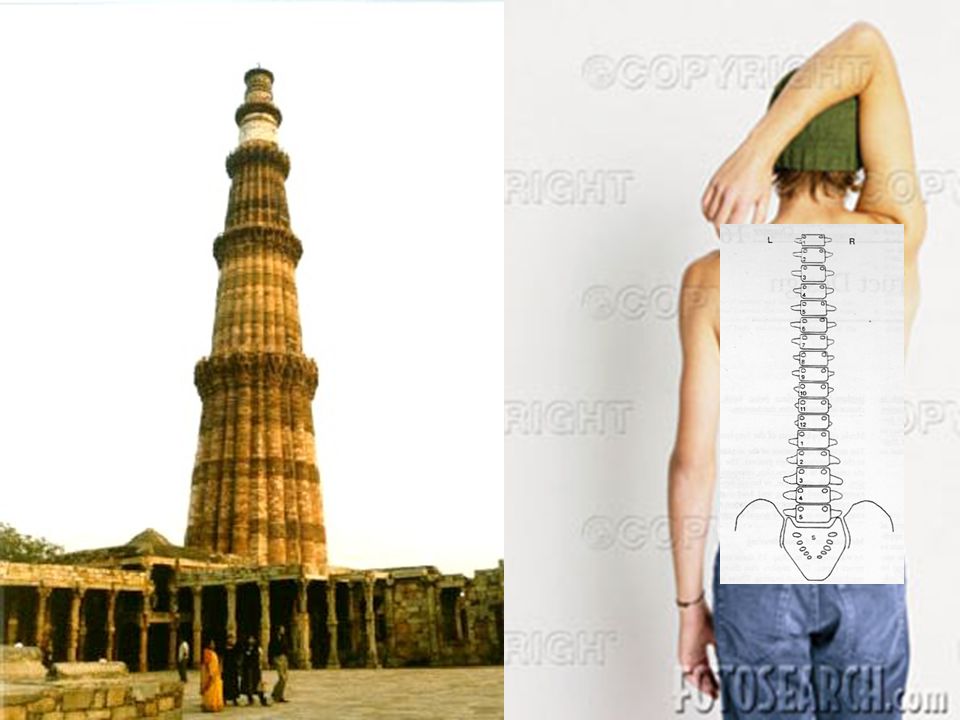
The Human spine-Broad based vertical pillar with spring effect
Looks like a minaret but has tremendous flexibility and load carrying capacity under bent positions. Efficient protective mechanism by the strong front and back muscles that spare the bony column from excessive loading.

33
Review of basic concepts
Human spine- Phylogenetically the best evolved, vertical spine amongst all vertebrates. Basic function- Painless axial loading an all positions of movements WITHOUT ACTUAL OR POTENTIAL RISK TO THE NUERAL ELEMENTS.

35
The built-in protectors

37
The IAR and the neutral zone

38
The line of weight transmission in spine-
Cer. Spine- lateral mass and partly posterior elements Dorsal spine- vertebral bodies Lumbar spine- posterior elements (facet joints are not a part of normal weight bearing) Change over in juctional areas
 Change over in juctional areas.")
39
Effects of Sedentary life style
Loss of in built protectors Lets the stresses pass on to areas that are not meant for. Sets in degeneration that encroaches on to the neural space- nerve roots. Loss of compressile strength of the vertebral bone.

40
THE ‘RADIATING’ LEG PAIN
Anatomical-Pertains to a definite neural segment, extends up to or distal to ankle with signs of root compression. Non-anatomical- confusion of the sensory cortex due to limb bud rotation. Extends only up to the back of the thigh and knee. No neural signs

41
The diffuse back pain- from the superficial layer of muscles
Not related to spine if not in the DEAD midline. Pain that spreads along the top of posterior iliac crest – disuse of latissimus dorsi. Pain in the dorsolumbar and interscapular area- disuse of trapezius.

42
INTERSCAPULAR AND SHOULDER PAINS
Different from NECK PAIN- midline location (Neck pain is a much more sinister sign. Pain in the area of upper trapezius, Levator scapulae and the rhomboids) ‘Radiation’ to the arm -Truly anatomical? Non- anatomical ‘Drag pain’ all over the limb
 ‘Radiation’ to the arm -Truly anatomical Non- anatomical ‘Drag pain’ all over the limb.")
43
Investigations Mostly required to check the bone quality
1. Nutritional osteoporosis 2. Disuse osteoporosis 3. Drug or disease related osteoporosis Good quality x rays of spine and pelvis, DEXA, biochemical investigations

44
X rays of the affected joints/spine
Mechanical alignment of the bones in weight bearing areas- -Lumbosacral inclination -cervical curvature -knee alignment-genu varum/valgum -foot arches -sacrococcygeal junction

45
Ask for X ray pelvis AP view Lumbosacral spine AP and Lateral views
Ultrasonographic bone densitometry Biochemical investigations not very useful Blood sugar in relevant cases.

46
Remember! No investigation will give you a diagnosis or a cause of pain that you have not clinically suspected.

47
Management Aim at definitive treatment i.e. permanent and lasting relief by treating the root cause if possible. NSAIDs ARE NOT A DEFINITIVE TREATMENT! IT MAY BE LIFESTYLE ITSELF!

48
The link must be treated together
Muscles and bones cannot be treated separately for aches and pains. Each area has a key muscle that needs to be specifically targeted. Identify that.

49
THE TREATMENT Prolonged, persistent and specific to the cause.
Keystones Initial pain relief Calcium and its utilization Antiosteoporotic drugs Osteogenesis- Sureshot only by exercise.

50
PHYSIOTHERAPY Machines expected to do miracles? Traction, diathermy
Ultrasound TENS LASER (Acute phase relievers)
")
51
Exercises-active and passive
What the patient does by himself is the best physiotherapy. Can be taught to the patient pertaining to his problem right in the outdoor Should target the extensor of the painful area.

52
The basic rule of muscle activity
Full initial passive stretch before the muscle begins an effective contraction. Strengthening exercise must begin with stretching exercises Two joint muscles like Rectus femoris need special attention Daily floor level activity stretches many muscles

53
Basic types of exercises- Isotonic and isometric
Repetitive exercise- cause muscle hypertrophy, good for wasted muscles. Endurance exercises- Sustaining the contraction up to the level of fatigue. Increases the fatigue strength which must come to normal.

54
FLAWS IN EXERCISE PRESCRIPTIONS
Wrong muscle and wrong exercise chosen Absence of initial stretching exercises Too little exercise Trick movements Reaching a static level of exercise Too short a period of exercise Organic pathology missed out-e.g. stiff joint

55
How long to exercise? Preferably for the rest of the life time. Make it a routine. At least till the muscle gets back its full length and strength(3-6 MONTHS), progressively increasing.
, progressively increasing.")
56
WHAT ABOUT ORTHOSES? Collars, corsets, arch supports and the like.
Good for acute pain relief and doubtful diagnosis under investigation. Prolonged use causes wasting of muscles and aggravation of pain. Psychological dependency on the orthosis both for the surgeon and the patient.

57
Local applications and fomentation
Only temporary, symptomatic treatment. Good for initiation of exercises, hot packs better. Wean off quickly, if you prescribe . Help in acute painful conditions with no skin inflammation, for superficial areas. No definite relief for deeper areas like back. May help psychologically.

58
Specific exercises and target muscles
Lower back- Lumbar fascia and erector spinae stretching, abdominal muscle strengthening. Interscapular area- Upper trapezius, Rhomboids and levator scapulae- Overhead abduction of arms, shoulder bracing.

59
For the knee joint- Anterior knee pain- Rectus femoris stretching prone position, sustained vastus medialis exercise. Straight leg raising- for vastus medialis contraction. Hamstring stretching in specific situations

60
Difficult areas- areas of ‘white tissue abundance’
Red muscle fibers easy to stretch. Relative lack of elasticity in ‘white’ tissues-fascia, tendons, ligaments, capsule, fibrous tissue Areas of loose areolar tissue Loss of gliding planes between different tissues.

61
The more difficult areas
1.FROZEN SHOULDER-Extensive fibrosis in the anteroinferior capsule (an area full of ‘white’ tissues) 2.HAND- Abundant loose areolar tissue right in the subcutaneous planes for extensive skin mobility, lost by fibrosis. 3.COCCYX- vestigial structure with ? bilateral sensory cortical representation.
 2.HAND- Abundant loose areolar tissue right in the subcutaneous planes for extensive skin mobility, lost by fibrosis. 3.COCCYX- vestigial structure with bilateral sensory cortical representation.")
62
Specific Physiotherapy for a stiff shoulder
Daily passive stretching and active assisted exercises in the direction of first EXTERNAL ROTATION , then ABDUCTION in supine position (Abduction essentially involves external rotation).
.")
63
Scapulothoracic rhythm
Abduction initiated by supraspinatus Taken over by deltoid upto 90 degrees Glenohumeral joint adducted by the short muscles to make a single unit Scapulothoracic movement by trapezius and other major muscles

64
Reversal of scapulothoracic rhythm
Stiff glenohumeral joint moves as one unit. No true abduction. Pt cannot do this movement on his own. Needs passive/ active assisted stretching of glenohumeral joint.

66
For the hand Quick mobilization at the earliest opportunity. Do not waste time. Devices like wax bath, under water exercises help significantly. Passive assisted flexion of the MP and IP joint helps initially. ‘Thumb in palm’ grip exercises for CMC jt.

67
Heel pain Entrapment neuropathy of medial planter nerve under the flexor retinaculum. Water logging during non activity. (Arches normal, plum patients ) Flat foot/planovalgus foot with abnormal heel stresses- needs correction.
 Flat foot/planovalgus foot with abnormal heel stresses- needs correction.")
68
Flat foot pain Flexible flat foot- arch flattens on weight bearing.
Tib. Post. comes under undue stretch. Leads to TP tendinitis or enthesitis. Walking in inversion, local heat and arch support help.

69
General exercises for foot problems
Tip toe walking, heel walking, walking in inversion. Gripping small objects in toe- marbles, cloth- for intrinsic muscle exercises. Must be weight bearing exercises. Activates the peripheral pump of calf muscles.

70
Other useful modalities
For heel pain- Medial calcaneal nerve block followed by inversion exercises, intrinsic foot muscle exercises Multiple cutaneus branches supply the heel pad. Point of exit of the nerves to be blocked.

71
Elbow pain- Tennis/Golfer’s elbow.
Lack of overhead, antigravity gripping activity. Always acted upon by gravity, leads to drag pain. Treated by overhead elbow extension exercises with wrist dorsiflexion and grip exercises.

72
Non specific wrist pain and De’quervain’s disease
Lack of compressile loading of radiocarpal joint. Grip exercises Stenosing tenosynovitis of thumb abductors and extensors. ‘Thumb in palm’ grip exercises along with sheath infiltration.

73
Coccydynia Related to the pelvic diaphragm musculature.
Squatting stretches these muscles, chair level activity may not. Small synovial joint at the sacro-coccygial junction. Too thin a patient with friction during sitting- congenital exagg. of curvature.

74
Treatment Pelvic diaphragm exercises-levator ani the key muscles.
Sphincter exercises Carbamazepine 100 mgm t.i.d.. may help

75
Therapeutics of aches and pains
Do not depend on the NSAIDs. Just begin and switch on to PT. Calcium alone is not a definitive treatment. Utilization of calcium needs to be improved with supplementation of vit. D. Though fat soluble, the safety margin of vit. D therapy is considerable.

76
Osteoporosis Multifactorial origin Inactivity contributes.
Sustained, combined treatment for MONTHS, not days or weeks. Antiosteoporotic drugs –bisphosphonates, dicerine and other newer drugs.

77
‘The latest drug’ Newer drugs take time to prove their efficacy.
Go slow on jumping into the use of a drug that a MR is ‘teaching’ you! Study the pharmacology well before use. Useful in patients with strong psychological overlay.

78
Remember! There is no miracle drug for a pain arising from the effects of prolonged inactivity of a muscle or a drug to change the bone quality overnight!

79
SPECIAL MODALITIES AVAILABLE
Nerve blocks- for Acute brachialgia Acute disc pain Steroids in acute neuralgic pains Centrally acting drugs –Diazepam, GABApen,carbamazepine etc. Muscle relaxants- Methacarbamol Microvasodilators- Xantinol nicotinate-Complamina Cinnerazine

80
Points to remember The condition is not a short term pathology.
It reflects the lifestyle of an individual. Either nutrition or exercise or both -is the missing link. That does not change in a short time. Have patience and persistence (like ATT!)
")
81
For the paediatric age group
Growth pains in lower limbs very common. Improve the utilization and supply of calcium, providing for reserves as well. BACK PAIN IN A CHILD IS A SINISTER SIGN, UNLESS PROVED OTHERWISE. Investigate fully for any pathology. CHILDREN DO NOT NEED PHYSIOTHERAPY.

82
Role of quick relief? Only in acute painful episodes, use a local heating system and a short term, simple NSAID, even paracetamol ! Do not expect miracles out of NSAIDs, any combination is not the definitive treatment. Keep drugs to minimum possible and motivate the patient to be active. Weight reduction.

83
Best to do Do not restrict the patients normal activities as far as possible. Encourage him to be more active. Concentrate on the muscle which is not used daily. Encourage floor level activity. Target exercises against resistance for the particular extensor muscle of the area.

85
Can diet help? YES! More roughage rich diet, whole grains better than ’factory generated’, packed foods. 2. Diet advice quickly changes the psychology due to traditional values. ‘God made’ (natural) food always better than ‘man-made’ (processed) food!
 food always better than ‘man-made’ (processed) food!")
86
Differentiate the following
Rheumatoid arthritis, Gouty arthritis and nonspecific MULTIPLE JOINT PAINS Acute or chronic disc prolapse. Spondylolisthesis Early infections of spine Malignancies/Tumors of spine and LOW BACK PAIN

87
Summery Aging is not a disease and is NOT painful, inactivity and obesity can be. Bone stock is a reflection of an individual’s life style. Full mobility is the key word to prevent disuse of antigravity ‘human’ muscles and also to maintain the bone quality.

88
REMEMBER All of us are aging. Nobody is immune to degeneration.
Take care of your bone stalk today! Tomorrow may be too late. Cost of Today’s fun with alcohol is being paid through your bones! Today’s comfort loving, machine oriented life is tomorrow’s discomfort. WALK more!

89
The message Good, balanced nutrition and vigorous physical activity is THE orthopaedic prescription for non specific aches and pains for ALL AGES AND ALL PROFESSIONS.

90
TAKE CARE! THANK YOU

Similar presentations















 definition: exercising joints through the available motion to maintain available range.>")






