Download presentation
Presentation is loading. Please wait.

1
University Hospital of Trondheim
St. Olavs Hospital University Hospital of Trondheim Admission to Department of General Internal Medicine or Department of Geriatrics Does it matter? Olav Sletvold

2
Reasons for asking……… Demographics and epidemiological trends
Greying of nations Geriatric giants incidence/prevalence-incidence Concern about future organisation Health care models Hospitals/primary sector Specialties ”Obsolete” traditions Ongoing discussions Journals/associations/health authorities Scientific evidence There are many good reasons for asking, actually. First of all changes in demographics I have called it greying of nations, and the future is ours, definitely. The huge increase in the number of elderly people in the years to come,is mainly due to the upcoming group of baby boomers, of which I am a member myself. Here you see the estimates form Norway.

3
Demographics of Norway Elderly persons > 67 years
You see that for the present we are just at the beginning of the new wave of older persons 67 years and older. Actually this is not a wave because we hardly see the end of the beginning, and not at all the beginning of the end, to paraphrase Winston Churchill. And as we have heard earlier during this congress the situation is the same for most countris to be compared with. Ref: Statistics Norway 2008,

4
Reasons for asking……… Demographical and epidemiological trends
Greying of nations Geriatric giants incidence/prevalence-incidence Concern about future organisation Health care models Hospitals/primary sector Specialties ”Obsolete” traditions Ongoing discussions Journals/associations/health authorities Scientific evidence During this congress we have also heard that in the follow years we will see compression of disability, but at the same time no compression of morbidity. Although there may be differences between countries. In the Clinic of General internal medicine in which I work about 50% of the patients are above 75 years, and 25 % between A rough estimate is that about 30% of medical patients above 75 can be considered as geriatric, characterised by high age of course, acute on severeal chronic diseases, have problems with activities of daily life aso. These trends have created great concern about the financing of health care, and authorities are looking for more cost efficient ways of organising the services. Mainly to reduce the use of money, and definitely not to improve the services. At least in Norway, there has also been a debate on the organisation and content of the specialty of geriatric medicine, initiated by central health officials. And you may all know about the discussion in BMJ, reagring geriatrics as a specialty.

5
”The Malta Definition”
EUGMS

6
“The Malta Definition” of Geriatric Medicine
Geriatric Medicine is a specialty of medicine concerned with physical, mental, functional and social conditions occurring in the acute care, chronic disease, rehabilitation, prevention, social and end of life situations in older patients. This group of patients are considered to have a high degree of frailty and active multiple pathology, requiring a holistic approach. Diseases may present differently in old age, are often very difficult to diagnose, the response to treatment is often delayed and there is frequently a need for social support. Geriatric Medicine therefore exceeds organ orientated medicine offering additional therapy in a multidisciplinary team setting, the main aim of which is to optimise the functional status of the older person and improve the quality of life and autonomy. Geriatric Medicine is not specifically age defined but will deal with the typical morbidity found in older patients. Most patients will be over 65 years of age but the problems best dealt with by the speciality of Geriatric Medicine become much more common in the 80+ age group. It is recognised that for historic and structural reasons the organisation of geriatric medicine may vary between European Member Countries. In May this year the GMS UEMS had their meeting in Malta agreeing on what geriatric medicine really should be, discribing characteristics of geriatric patients, and stating the aims for geriatric care. The declaration is comprehensive, but at the same time very general. Still there are possibilities for great variety. Even within a single country, or in a single health region in Norway there are may different ways of organising the practice of geriatric medicine, also in-hospital services. Ref: Minutes GMS UEMS-meeting Malta, accepted 03/5/08

8
Comprehensive geriatric assessment (CGA)
Key components of geriatric medicine Co-ordinated multidisciplinary assessment Identification of medical, functional, social and psychological problems The formation of a plan of care including appropriate rehabilitation The ability to directly implement treatment recommodations made by the multidisciplinary team Long term follow-up Ref: Ellis G, Whitehead M, Robinson D, O’Neill D, Langhorne P. Comprehensive geriatric assessment for older adults admitted to hospital: a systematic review (prototcol) (2006). The Cochrane Library 2008, Issue 3 When we are up to compare geriatric medicine vs internal medicine, it is important to make short brussh-up of what geriatric medicine actually is: Hopefully most of you know the key components of comprehensive geriatric assessment, here as listed in the Cochrane protocol of Graham Ellis, when he and his group is planning to do a systematic review on in-hospital geriatric assessment. We also know that within internal medicine specialties, this is far from what is going on, especially regarding the first 3 items. The organ-oriented medical practice rules!!! But a department of geriatric medicine is not a department of medicine is not a department of geriatric medicine….
 (2006). The Cochrane Library 2008, Issue 3. When we are up to compare geriatric medicine vs internal medicine, it is important to make short brussh-up of what geriatric medicine actually is: Hopefully most of you know the key components of comprehensive geriatric assessment, here as listed in the Cochrane protocol of Graham Ellis, when he and his group is planning to do a systematic review on in-hospital geriatric assessment. We also know that within internal medicine specialties, this is far from what is going on, especially regarding the first 3 items. The organ-oriented medical practice rules!!! But a department of geriatric medicine is not a department of medicine is not a department of geriatric medicine….")
9
Categorisation of CGA programmes
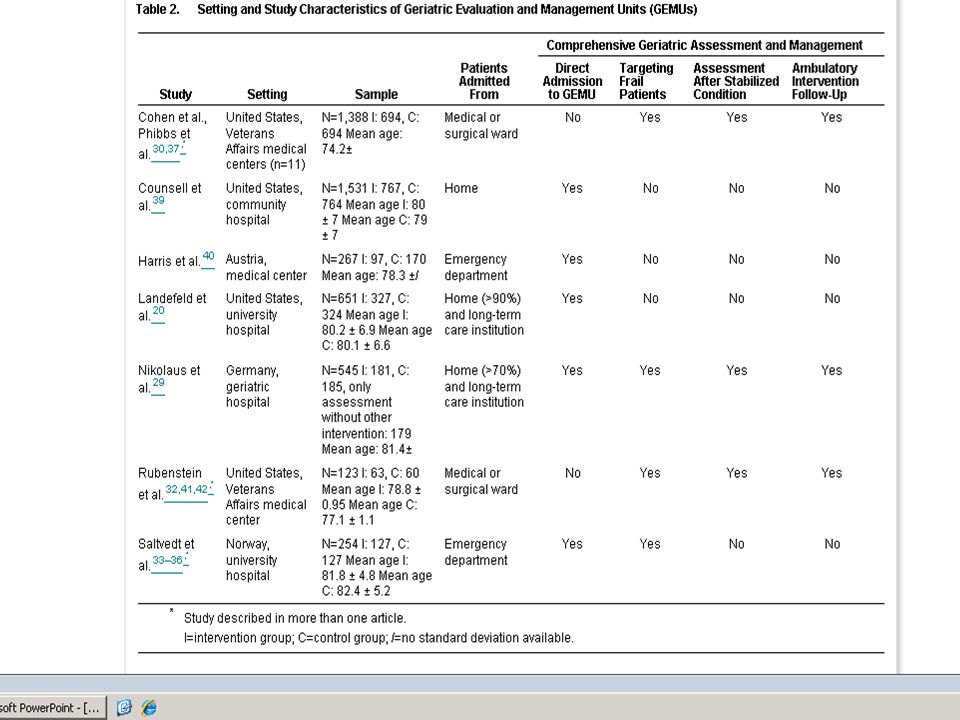
GEMU Hospital geriatric evaluation and management unit, a designated inpatient unit for CGA and rehab IGCS Inpatient geriatrics consultation service, non-designated units where CGA is provided to hospital patients on a consultative basis HAS Home assessment service, in-home CGA for community dwelling persons HHAS Hospital home assessment service, in-home assessment for recently discharged patients OAS Outpatient assessment service, CGA in outpatient settings Ref: Stuck AE, Siu AL, Wieland, GD, Adams J, Rubenstein LZ. Comprehensive geriatric assessment: a metaanalysis of controlled trials. Lancet, 1993,342: Digging up the evidence for if it makes a difference if geriatric patients are admitted to a hospital Department of General Internal Medicine or Geriatrics, however, leads us into a difficult terrain. The components may be present, but what about organisation and models. Here you see how Stuck categorised the different programmes. In real life you will will find combinations of facilities Eksempler

10
Structure of specialities
Internal Medicine Independent main specialty (most countries) Including subspecialties of Geriatrics Cardiology Hematology Pulmology Nephrology Endocrinoloy Gastroenterology Infectious diseases General Internal Medicine (i.e. Denmark) Geriatrics Independent main specialty (many countries) (UK, Sweden) Independent subspeciality of Internal Medicine (Norway) Variants Independent specialty/subspecialty (Finland) Diploma/certification (USA) No specialty Portugal Talking about internal medicine vs geriatric medicine may also seem easy when we think about spcialties: Although medical specialities, in this case internal medicine and geriatrics, to some extent defined, even in a European context, they are not yet sufficiently homogenous across national borders to talk about European geriatrics. As you see here, even in the Nordic countries the entrance into the specialty may differ substantially, and differences as for content should also be noted, So both organisation and content of specialty are important premises for the validity of existing evidence as to the question in the title
 Including subspecialties of. Geriatrics. Cardiology. Hematology. Pulmology. Nephrology. Endocrinoloy. Gastroenterology. Infectious diseases. General Internal Medicine (i.e. Denmark) Geriatrics. Independent main specialty (many countries) (UK, Sweden) Independent subspeciality of. Internal Medicine (Norway) Variants. Independent specialty/subspecialty (Finland) Diploma/certification (USA) No specialty. Portugal. Talking about internal medicine vs geriatric medicine may also seem easy when we think about spcialties: Although medical specialities, in this case internal medicine and geriatrics, to some extent defined, even in a European context, they are not yet sufficiently homogenous across national borders to talk about European geriatrics. As you see here, even in the Nordic countries the entrance into the specialty may differ substantially, and differences as for content should also be noted, So both organisation and content of specialty are important premises for the validity of existing evidence as to the question in the title.")
11
Admission to Department of General Internal Medicine or Department of Geriatrics
Does it really matter? So do we actually know if it matters? In my opinion we have strong, very strong evidence.

12
Selected references Geriatrics vs. internal medicine
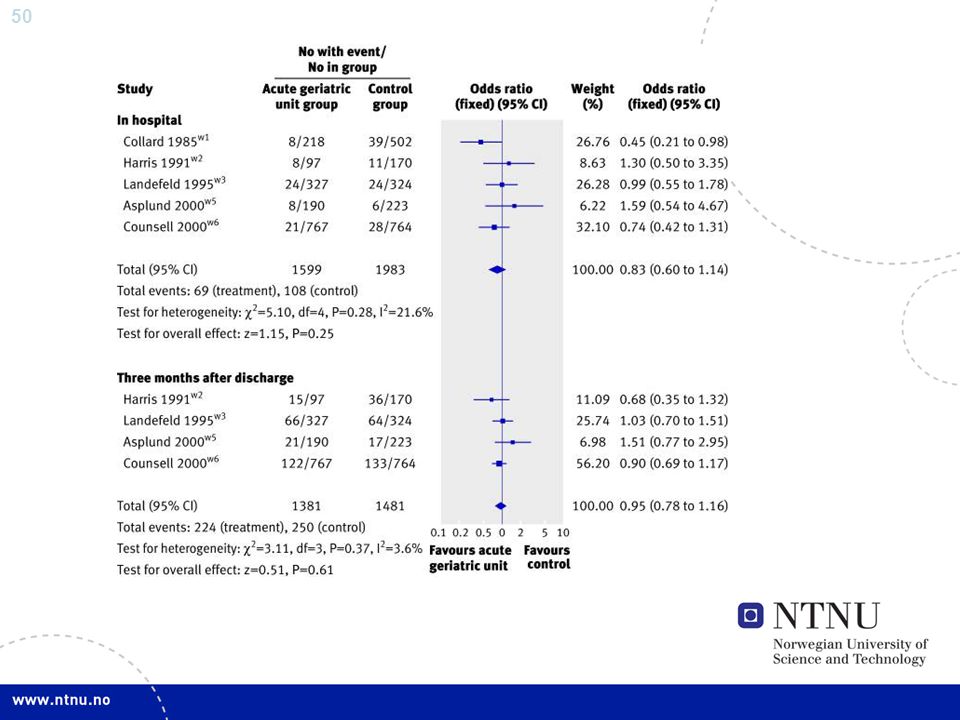
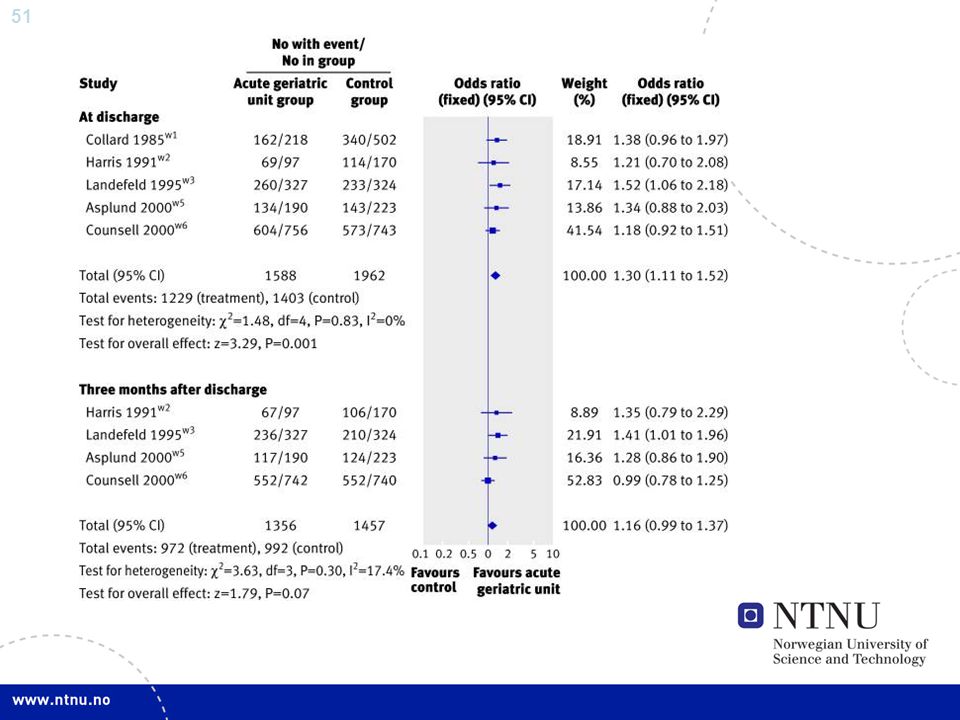
Rubenstein LZ, Josephson KR, Wieland GD, English PA, Sayre JA, Kane RL. Effectiveness of a geriatric evaluation unit. A randomized clinical study. N Engl J Med, 1984, 311: Harris RD, Hevnscke PJ, Popplewell PY, Radford AJ, Bond MJ, Turnbull RJ, Hobbin ER, Chalmers JP, Tonkin A, Stewart AM. A randomised study of outcomes in a defined group of acutely ill elderly patients managed in a geriatric assessment unit or a general medical unit. Aus NZ J Med, 1991, 21: Counsell SR, Holder CM, Liebenauer LL, Palmer RM Fortinsky RH, Kresevic DM , Quinn LM, Allen KR, Covinsky KE, Landefeld CS. Effect of a multicomponent intervention on functional outcomesand process of care in hospitalized older patients: a randomized controlled trial of Acute Care for Elders (ACE) in a community hospital. J Am Ger Soc 2000, 48: Asplund K, Gustafson Y, Jacobsson C, Bucht G, Wahlin, A, Peterson J, Blom JO, Ängquist KA. Geriatric-based versus general wards for older acute medical patients:a randomized comparison of outcomes and use of resources. J Am Ger Soc 2000, 48: I Saltvedt, ES Opdahl Moe, P Fayers, S Kaasa, O Sletvold. Reduced mortality in treating acutely sick, frail elderly patients in a geriatric and evaluation and management unit. J Am Ger Soc 2002, 50: But what about geriatric medicine vs internal medicine? What evidence do we have? This slide shows you selected references from single studies, and I will spend most of the remaining time on two studies: Namely the Sepulveda-study of Rubenstein published 1984, and the first report from the Trondheim-study published by Saltvedt as first author in 2002. And she is in the audience to-day!
 in a community hospital. J Am Ger Soc 2000, 48: Asplund K, Gustafson Y, Jacobsson C, Bucht G, Wahlin, A, Peterson J, Blom JO, Ängquist KA. Geriatric-based versus general wards for older acute medical patients:a randomized comparison of outcomes and use of resources. J Am Ger Soc 2000, 48: I Saltvedt, ES Opdahl Moe, P Fayers, S Kaasa, O Sletvold. Reduced mortality in treating acutely sick, frail elderly patients in a geriatric and evaluation and management unit. J Am Ger Soc 2002, 50: But what about geriatric medicine vs internal medicine What evidence do we have This slide shows you selected references from single studies, and I will spend most of the remaining time on two studies: Namely the Sepulveda-study of Rubenstein published 1984, and the first report from the Trondheim-study published by Saltvedt as first author in And she is in the audience to-day!")
13
Trials not considered RCTs on Non-RCTs CGA in combined units
Casemix of both medical and surgical patients Discharge-planning teams Extended care services Hospital-based Outpatient clinics Home-based services Non-RCTs I have strictly chosen to report from two studies comparing in-hospital care of geriatric patients targeted for frailty, and to avoid studies possibly used as evidence of the first presentation today. I do not report from studies on models involving extended or home-based care, alone or in combination with in-hospital care, also studies including a surgical casmix. And not non-RCTs.

14
1984 Ref: Rubenstein & al N Engl J Med, 1984
So let us og back to the to most important single trials: 1984 was the year after I started as a research-fellow in Bergen, looking into cell-cycle kinetics and stem cells in aging mice. I was just to finish my training in hematology and internal medicine. On that occasion my superviser said: First you finish your project, and then you train for geriatric medicine. There was no geriatrician in Bergen at that time. No way, I said I will do the research, but I will never become a geriatrician! The next year L. Rubenstein provied some very important evidence showing the huge reduction in mortality using CGA-technology. 3 years later I was doing my training in geriatric medicine, and I have never felt any regrets about that. So 1984 was an important year. Many of you have of course seen this figure before. To me it represented the mental turning point! Ref: Rubenstein & al N Engl J Med, 1984

15
2002 2002 was another important year a for creating evidence for geriatric medicine. That year I had the privilege to be the senior author and the leader of a group publishing the report from the establishment of geriatric medicine in an acute hospital in Trondheim, Norway. And the report was to some extent confirming the findings of Rubenstein, 18 years earlier, here indicating the same huge reduction of mortality But I will show you more later on this! (p= at 3 months, p=0.02 at 6 months, and p=0.06 after 12 months) Ref: I Saltvedt & al J Am Ger Soc 2002
 Ref: I Saltvedt & al J Am Ger Soc")
16
Rubenstein & al N Engl J Med, 1984
Geriatric Unit (15 beds) of the Sepulveda VA Medical Center Intermediate care (non-acute) area of the hospital Inclusion criteria All persons admitted to acute-care services of a VA medical center still in hospital after one week Patients 65 + years with continued medical, functional or psychological problems preventing discharge home Exclusion criteria Patients with severe dementia, terminal illness, other severe conditions resistant to treatment, inevitably nursing home placement. Those well enough to return home without further support services Now we go back to the Rubenstein study. It is important to note that it was done in a VA setting, and therefore including mainly men. The geriatric ward was also located in an intermediate care area. And, the patients to be included were still in the hospital one week after admission! And all patients had functional problems, as a frailty indicator!
 of the Sepulveda VA Medical Center. Intermediate care (non-acute) area of the hospital. Inclusion criteria. All persons admitted to acute-care services of a VA medical center still in hospital after one week. Patients 65 + years with continued medical, functional or psychological problems preventing discharge home. Exclusion criteria. Patients with severe dementia, terminal illness, other severe conditions resistant to treatment, inevitably nursing home placement. Those well enough to return home without further support services. Now we go back to the Rubenstein study. It is important to note that it was done in a VA setting, and therefore including mainly men. The geriatric ward was also located in an intermediate care area. And, the patients to be included were still in the hospital one week after admission! And all patients had functional problems, as a frailty indicator!")
17
Rubenstein & al N Engl J Med, 1984
Intervention group After randomisation patients were admitted to the Geriatric unit intervention usually within 48 hours Geriatric work-up Interdisciplinary team Control group Usual hospital acute care services Age >70 years (79 vs 77 years) Male-VA (95 vs 96 %) LOS (55 vs 44 days) Here you see an additional delay of 2 days before intervenyion, the implication of which is that the patients had been 9 days in hospital before intervention. Nearly the mean LOS for patients in our department in 2008. The intervention group also had some follw-up in the outpatient clinic, indicating that the design was not ”clean” as we say. The male predominance makes the findings non-valid for women of course, and the mean length of stay is an exception in our department in 2008! Therefore the external validity for Europe 2008 may be questioned.
 Male-VA (95 vs 96 %) LOS (55 vs 44 days) Here you see an additional delay of 2 days before intervenyion, the implication of which is that the patients had been 9 days in hospital before intervention. Nearly the mean LOS for patients in our department in The intervention group also had some follw-up in the outpatient clinic, indicating that the design was not clean as we say. The male predominance makes the findings non-valid for women of course, and the mean length of stay is an exception in our department in 2008! Therefore the external validity for Europe 2008 may be questioned.")
18
Findings in favour of GU
At one year Lower mortality (23.8 vs 48.3%) Fewer had initially been discharged to a nursing home (12.7 vs 30.0%) Patients were less likely having spent time in a nursing home (26.9 vs 46.7) They more likely had improvement of functional status Lower direct costs However, the findings were impressive! Both regarding mortality, nursing home placement and functional improvement! So it mattered in Sepulveda! Ref: Rubenstein & al N Engl J Med, 1984
 Fewer had initially been discharged to a nursing home (12.7 vs 30.0%) Patients were less likely having spent time in a nursing home (26.9 vs 46.7) They more likely had improvement of functional status. Lower direct costs. However, the findings were impressive! Both regarding mortality, nursing home placement and functional improvement! So it mattered in Sepulveda! Ref: Rubenstein & al N Engl J Med,")
19
Ref: Rubenstein N Engl J Med, 1984
Here we go back to the mortality curve. By the years of course, the curves met, but who lives forever! Not even male Americans! Ref: Rubenstein N Engl J Med, 1984

20
Saltvedt & al J Am Ger Soc 2002
Section of Geriatrics (9 beds), Department of Internal Medicine, St. Olav University Hospital of Trondheim Acute hospital Inclusion criteria Age > 75 years Admitted as an emergency to the Department of Internal Medicine Having at least one of Winograd’s targeting criteria Exclusion criteria Living in nursing home, previously independent and expected to be so without geriatric intervention, cancer with metastasis, or other disorder with short living expectation, advanced dementia, need for specific treatment in another ward The I go back to my own place and the study published by Ingvild Saltvedt. She did a tremendous amount of work. Those who have not done a study like that do not know how much work it is in it! I am very grateful to Ingvild, and strangely enough we are still friends after all these years, with frustrations and fighting, and fun! Our patients were somewhat older than Rubensteins, and we used specified targeting criteria.
, Department of Internal Medicine, St. Olav University Hospital of Trondheim. Acute hospital. Inclusion criteria. Age > 75 years. Admitted as an emergency to the Department of Internal Medicine. Having at least one of Winograd’s targeting criteria. Exclusion criteria. Living in nursing home, previously independent and expected to be so without geriatric intervention, cancer with metastasis, or other disorder with short living expectation, advanced dementia, need for specific treatment. in another ward. The I go back to my own place and the study published by Ingvild Saltvedt. She did a tremendous amount of work. Those who have not done a study like that do not know how much work it is in it! I am very grateful to Ingvild, and strangely enough we are still friends after all these years, with frustrations and fighting, and fun! Our patients were somewhat older than Rubensteins, and we used specified targeting criteria.")
21
Targeting criteria Acute impairment of single ADL Imbalance, dizziness
Impaired mobility Chronic disability Weight loss, malnutrition Falls during the last 3 months Prolonged bedrest Depression Confusion Mild / moderate dementia Urinary incontinence Polypharmacy Vision or hearing impairment Social / family problems This slide shows the Winograd targeting criteria that have been shown to predict prolonged hospital stays, increased mortality and nursing home placement among elderly patients. These criteria were used to target frail patients in this study. Ref : Winograd & al J Am Ger Soc 1991

22
Baseline characteristics Age - mean SD Female - no (%)
Widowed/living alone - no(%) Living location Private home - no(%) Sheltered housing - no(%) Days in hospital before inclusion - median (iqr*) No. of targeting criteria GEMU (n=127) 82 5 81 (64) 93 (73) 115 (91) 12 (9) 2 (1;5) 4 (3;5) MW (n=127) 82 5 84 (66) 85 (67) 110 (87) 17 (13) 3 (1;6) 4 (3;5) Looking into the baseline characteristics shows you the following: There were no statistically significantly differences in the baseline characteristics. Mean age in both groups was 82 years. About two thirds were women, and about 70% were living alone Most patients were living in their private homes although 9% of the GEMU and 13% of the MW patients were living in sheltered housing. The GEMU patients stayed median 2 days in the medical department before inclusion in the study as compared to 3 days in the MW group. In both groups the median number of targeting criteria was 4. *iqr= interquartile range
 Living location. Private home - no(%) Sheltered housing - no(%) Days in hospital before inclusion. - median (iqr*) No. of targeting criteria. GEMU. (n=127) 82 (64) 93 (73) 115 (91) 12 (9) 2 (1;5) 4 (3;5) MW. (n=127) 82 (66) 85 (67) 110 (87) 17 (13) 3 (1;6) 4 (3;5) Looking into the baseline characteristics shows you the following: There were no statistically significantly differences in the baseline characteristics. Mean age in both groups was 82 years. About two thirds were women, and. about 70% were living alone. Most patients were living in their private homes although 9% of the GEMU and 13% of the MW patients were living in sheltered housing. The GEMU patients stayed median 2 days in the medical department before inclusion in the study as compared to 3 days in the MW group. In both groups the median number of targeting criteria was 4. *iqr= interquartile range.")
23
Saltvedt & al J Am Ger Soc 2002
Intervention group After randomisation patients were transferred to the Geriatric unit the same day Geriatric work-up Interdisciplinary team Control group Usual acute hospital care services LOS (19 vs 13 days)(median) As compared with Rubesteins study, the intervention patients were transferred on the day of randomisation. And be especially aware of the length of stay that is considerably shorter than Rubensteins, but definitely longer that ie Asplund and Gustafsons. This fact indicates in my opinion a different casemix from ours! In 2008 the mean lenth of stay for geriatric in-patients is about 10 days.
(median) As compared with Rubesteins study, the intervention patients were transferred on the day of randomisation. And be especially aware of the length of stay that is considerably shorter than Rubensteins, but definitely longer that ie Asplund and Gustafsons. This fact indicates in my opinion a different casemix from ours! In 2008 the mean lenth of stay for geriatric in-patients is about 10 days.")
24
Time to discharge At randomisation it was a premise that the patient should be needing hospital treatment for at least 2 another days. Here you see that 18 of the patients from the control group actually were discharged within 2 days! Whether this had any impact on the results is difficult to say, but lets og to the next slide…..

25
Cumulative survival Here you see the most important findings:
At 3 months the mortality in the GEMU group was 12 % as compared to 27% in the MW group. At 6 months it was 16% in the GEMU group and 29% in the MW group. In other words the mortality during the first 6 months was reduced by about 50%, which was statistically significant. After 12 months there was a trend for better survival in the GEMU group. The median survival in both groups was about 2 years. (p= at 3 months, p=0.02 at 6 months, and p=0.06 after 12 months)
")
26
Looking into the causes of death, you also see interesting differences.
IE. Fewer patients died from heart diseases in the intervention group as compared to the controls. The cardiologist did not facy these result at all. And most patients in the trial were primarily admitted to the wards of cardiology. But still, what is best: dying from an infection, or from an emergency of cardiology?

27
Readmissions are an important parameter.
However, there were no differences between the groups.

28
Number of patients living at home
3 months 6 months GEMU (n=127) (80%) 92 (73%) MW (n=127) (64%) 76 (61%) HR : 2.1 (1.3; 3.4) after 3 months. HR : 1.7 (1.1; 2.6) after 6 months. This slide shows you the number of patients living at home the first 6 months. And the HR is defintely in favour of the intervention group.
 101 (80%) 92 (73%) MW (n=127) 80 (64%) 76 (61%) HR : 2.1 (1.3; 3.4) after 3 months. HR : 1.7 (1.1; 2.6) after 6 months. This slide shows you the number of patients living at home the first 6 months. And the HR is defintely in favour of the intervention group.")
29
Partitioned survival curves
Nursing home The partitioned survival curves show the proportion of time the patients stayed in hospital, nursing homes and in their own homes during 6 months of follow up. The upper figure is the GEMU group. The dark blue field is the proportion of time spent in hospital. The GEMU group spent more time in hospital initially. This is due to the index stay that was 6 days longer in the GEMU group, which is statistically significant. The proportion of time spent in nursing homes which is the light blue field, was similar in both groups. The white field shows the proportion of time spent at home which is higher in the GEMU group. Nursing home Time (months)
")
30
Poor outcomes % 3 months 6 months 12 months
Composite outcomes are difficult to handle. In this slide you see combinations of different poor outcomes. The trend are obvious, but not statisticalle significant! Figure 2a. Proportion of the total number of patients in the GEMU and MW group who experienced a poor outcome (dead , dead or Barthel Index scores below 12, and dead or MMSE scores below 20).
.")
31
Positive outcomes 3 months 6 months 12 months %
This slide gives you an overview of differet functional variables. However, only the differences in survival were statistically significant! Figure 2b. Proportion of the total number of all patients recruited to the Geriatric Evaluation and Management Unit (GEMU) (n=127) and general medical wards (MW) (n=127) who experienced a positive outcome defined as surviving, having normal scores for Mini Mental Status Examination (MMSE), Barthel Index or Instrumental Activities of Daily Living (IADL). Differences in survival were statistically significant at 3 (p= 0.004) and 6 months (p=0.02). None of the other differences were statistically significant.
 (n=127) and general medical wards (MW) (n=127) who experienced a positive outcome defined as surviving, having normal scores for Mini Mental Status Examination (MMSE), Barthel Index or Instrumental Activities of Daily Living (IADL). Differences in survival were statistically significant at 3 (p= 0.004) and 6 months (p=0.02). None of the other differences were statistically significant.")
32
Drug use in favour of GEMU
More often discontinued Anticholinergic drugs CV-drugs Digitoxin Psychotrope dugs Neuroleptics More drugs started (trend): Antidepressants Estriol Reduction of patients on potential drug-drug interactions
: Antidepressants. Estriol. Reduction of patients on potential drug-drug interactions.")
33
Conclusion Treatment of acutely sick frail elderly patients in
a geriatric evaluation and management unit (GEMU) gave considerable reduction of mortality increased the patients’ chances of being able to live in their own homes So, what are tha conclusions? Definitely, the patients are far better off in a geriatric unit, than in wards of internal medicine! Ref: I Saltvedt & al J Am Ger Soc 2002
 gave. considerable reduction of mortality. increased the patients’ chances of being able to live in their own homes. So, what are tha conclusions Definitely, the patients are far better off in a geriatric unit, than in wards of internal medicine! Ref: I Saltvedt & al J Am Ger Soc")
34
Does it matter? Therefore, it matters!
I would to add that, if I had a drug with similar effects as performing CGA, reducing mortality with 50% making you able to live in your own home, I am sure that the public and society would have been willing to pay for it, especially if I had been young and not 82 years of age. That is the sad part of it! The good thing, however, is that the rational for what we geriatricians do performing CGA, the raison d’etre, is based on firm evidence!

35
Knowing where to go is important, also in geriatric medicine.
And as Vaupel stated yesteday, ”The future is ours” It is good to know that what we do as clinicians, works! And it works better than most drugs on the market! The challenge is to convince policymakers and officials that it is worh while, because many of our patients have enormous benefit may have huge benefit of in-hospital CGA as an alternative to internal medicine.

36
Comprehensive geriatric assessment (CGA)
Key components of geriatric medicine (CGA) Co-ordinated multidisciplinary assessment Identification of medical, functional, social and psychological problems The formation of a plan of care including appropriate rehabilitation The ability to directly implement treatment recommodations made by the multidisciplinary team Long term follow up Additional premises (?) for improved prognosis Targeting (age & frailty) Clinical skills and dedication Why does it work? The key components presented at the start of my lecture still holds true, I think In addition, I think that targeting patients with frailty, and not to forget dedication and clinical skill, should be added to the list!
 Co-ordinated multidisciplinary assessment. Identification of medical, functional, social and psychological problems. The formation of a plan of care including appropriate rehabilitation. The ability to directly implement treatment recommodations made by the multidisciplinary team. Long term follow up. Additional premises ( ) for improved prognosis. Targeting (age & frailty) Clinical skills and dedication. Why does it work The key components presented at the start of my lecture still holds true, I think. In addition, I think that targeting patients with frailty, and not to forget dedication and clinical skill, should be added to the list!")
37
From GEMU to acute geriatric care
St. Olav University Hospital 2010

38
Why? Asplund K, Gustafson Y, Jacobsson C, Bucht G, Wahlin, A, Peterson J, Blom JO, Ängquist KA. Geriatric-based versus general wards for older acute medical patients:a randomized comparison of outcomes and use of resources. J Am Ger Soc 2000, 48: Baztan JJ & al. Effecticeness of acute geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: Metaanalysis. BMJ 2009;338:b50 doi:101136/bmj.b50

40
Elderly patients referred to St. Olav University Hospital
At admittance in Emergency Department Initial assessment Physician on call ECG, urin analysis, blood testing, preliminary X-ray Triage Evaluating patients according to geriatric giants At admittance in Geriatric Ward (80-90% from ED) Initial evaluation and management Acute assessment and care by nurse and physician (geriatrician) Check lists Establish links with PHCS Preliminary assessments by other team members Informal consultations MD vs RN vs OT vs PT vs XX
 Initial evaluation and management. Acute assessment and care by nurse and physician (geriatrician) Check lists. Establish links with PHCS. Preliminary assessments by other team members. Informal consultations. MD vs RN vs OT vs PT vs XX.")
41
Geriatrics at St. Olav University Hospital
Day 1-2 More extensive geriatric assessment, and management Pre-ward round Evaluation by team members Follow-up of check-lists Treatment guidelines Ward round Informal consultations Formal meeting (2 PM, 5-15 min) All team members report their results from their own preliminary evaluation Agree on work-up and management (aims, care plan, discharge prerequisits, estimated LOS)
 All team members report their results from their own preliminary evaluation. Agree on work-up and management (aims, care plan, discharge prerequisits, estimated LOS)")
42
Geriatrics at St. Olav University Hospital
Day 2-3-x Continuous evaluation and management Daily routines Pre-ward round Ward round Follow-up of check-lists Treatment according to guidelines Informal consultations Formal meetings Evaluation of work-up and management (aims, discharge planning, estimated LOS) Networking with primary care professionels
 Networking with primary care professionels.")
43
Nurse General condition and needs Checklists Care plan
Patient & caregivers Situation at home Contact with the PHCS Report on functional limitations, resources i.a. Structured observations BP, BMI, Barthel ADL-index i.a. Checklists Case history/observations/evaluations/planning of nursing care/discharge/reporting Care plan Follow-up

44
Physiotherapist PT work-up Evaluation of Mobility aids
Falls, balance problems, immobility, physical activity limitations Mobility aids Compression stockings Hip protectors Exercise classes Potential for rehab

45
Consequences of CGA Additional interventions
Internal referrals More-targeted interventions Development of individual care plans Early start of discharge planning Timely rehabilitation Post discharge follow-up Outpatient geriatric clinic Work-up on cognitive decline etc (Interdisciplinary home intervention team)
")
46
Meta-analyses and reviews Comprehensive Geriatric Assessment
Stuck AE & al, Comprehensive geriatric assessment: a metaanalysis of controlled trials. Lancet, 1993, 342: Day & Rasmussen What is the evidence for the effectiveness of specialist geriatric services in acute, post-acute and sub-acute settings? New Zealand Health Technology Assessment Report 2004;7(3). Baztan JJ & al. Effecticeness of acute geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: Metaanalysis. BMJ 2009;338:b50 doi:101136/bmj.b50 Van Craen K & al. The effectiveness of inpatient geriatric evaluation and management units: A systematic review and metaanalysis. J Am Ger Soc 2010, 58,1:88-92 Bachmann S & al. Inpatient rehabilitation designed for geriatric patients: Systematic review and meta-analysis of randomised controlled trials. BMJ 2010; 340:c1718 doi: /bmj.c1718 In the following slides you see some selected publications. The evidence for the effectivenesss of CGA has been evaluated in at least one metaanalysis and several reviews as you see here. But compared with the number of papers on treating hypertension in the elderly, they are few, absolutely So far the Lancet-pubblication of Andreas Stuck has been the most important for the development, at least in Norway and Nordic countries. However, his metaanalysis did not specifically look into geriatric medicine vs. Internal medicine. And on previous occasions I may have used it for more than it is worth. But his overall conclusion was positive. CGA works! However, it is a long time since 1993! And Adreas put apples, pears and tomatoes into the same basket! I therefore look very much forward to Graham Ellis’ initiative on a systematic Cochrane review. Still, it is also worth while looking into the report from New Zealand. By the way, 1993 was an important year, the year when the Department of geriatrics in Trondheim was established
. Baztan JJ & al. Effecticeness of acute geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: Metaanalysis. BMJ 2009;338:b50 doi:101136/bmj.b50. Van Craen K & al. The effectiveness of inpatient geriatric evaluation and management units: A systematic review and metaanalysis. J Am Ger Soc 2010, 58,1: Bachmann S & al. Inpatient rehabilitation designed for geriatric patients: Systematic review and meta-analysis of randomised controlled trials. BMJ 2010; 340:c1718 doi: /bmj.c1718. In the following slides you see some selected publications. The evidence for the effectivenesss of CGA has been evaluated in at least one metaanalysis and several reviews as you see here. But compared with the number of papers on treating hypertension in the elderly, they are few, absolutely. So far the Lancet-pubblication of Andreas Stuck has been the most important for the development, at least in Norway and Nordic countries. However, his metaanalysis did not specifically look into geriatric medicine vs. Internal medicine. And on previous occasions I may have used it for more than it is worth. But his overall conclusion was positive. CGA works! However, it is a long time since 1993! And Adreas put apples, pears and tomatoes into the same basket! I therefore look very much forward to Graham Ellis’ initiative on a systematic Cochrane review. Still, it is also worth while looking into the report from New Zealand. By the way, 1993 was an important year, the year when the Department of geriatrics in Trondheim was established.")
48
Takk for meg

54
Challenges S Shepperd & al. Can We Systematically Review Studies That Evaluate Complex Interventions? PLoS Medicine, August 2009, Vol 6, Issue 8, doi: /journal.pmed t001 Van Ness & al. Gerontologic Biostatistics: The Statistical Challenges of Clinical Research with Older Study Participants. JAGS 2010 Jul;58(7): Epub 2010 Jun 1.
: Epub 2010 Jun 1.")
55
Evaluating and reviewing CGA
Intervention content Describe the content (the active ingredients) Describe any intervention received by the control group, including the content of ”usual care” Describe how the interventions were delivered (and any differences in delivery across included trials” (Describe the contextual similarities and differences between the trials) Intervention fidelity Include details describing whether the interventions (included in a review) do what is intended or if they deviated from the intended shape or form during the course of the implementation Include an assessment of whether an intervention failed because it was poorly implemented or it was not effective Intervention sustainability Include details on the sustainability of interventions ocver time S Shepperd & al. Can We Systematically Review Studies That Evaluate Complex Interventions? PLoS Medicine, August 2009, Vol 6, Issue 8, doi: /journal.pmed t001
 Describe any intervention received by the control group, including the content of usual care Describe how the interventions were delivered (and any differences in delivery across included trials (Describe the contextual similarities and differences between the trials) Intervention fidelity. Include details describing whether the interventions (included in a review) do what is intended or if they deviated from the intended shape or form during the course of the implementation. Include an assessment of whether an intervention failed because it was poorly implemented or it was not effective. Intervention sustainability. Include details on the sustainability of interventions ocver time. S Shepperd & al. Can We Systematically Review Studies That Evaluate Complex Interventions PLoS Medicine, August 2009, Vol 6, Issue 8, doi: /journal.pmed t001.")
56
Evaluating and reviewing CGA ctd.
Roll out/Scaling up of the intervention Report data on accessability, risk of AE, cost-effectiveness, or budget impact of interventions Address the following questions regarding the applicability of the evidence to individual patients: Have biological results (age, co-morbidities) that might modify the treatment respons been excluded? Can consumers comply with the treatment requirements? Can health care providers comply with the treatment requirements Are the likely benefits worth the potential risks and cost? S Shepperd & al. Can We Systematically Review Studies That Evaluate Complex Interventions? PLoS Medicine, August 2009, Vol 6, Issue 8, doi: /journal.pmed t001
 that might modify the treatment respons been excluded Can consumers comply with the treatment requirements Can health care providers comply with the treatment requirements. Are the likely benefits worth the potential risks and cost S Shepperd & al. Can We Systematically Review Studies That Evaluate Complex Interventions PLoS Medicine, August 2009, Vol 6, Issue 8, doi: /journal.pmed t001.")
57
Evaluating and reviewing CGA ctd.
Address the following questions regarding the applicability of the evidence in other health care systems Are there important differences or similarities in the structural elements of health systems or of health services between where the research was done and where it will be applied? Are there important differences in the on-the ground realities and constraints (governance, financial, delivery arrangements)? Are there likely to be important differences in the baseline conditions between where the research was done and other settings? Are there important differences in perspectives and influences of health system stakeholders between where the research was done and where it could be applied that might mean an intervention will not be accepted or taken up in the same way?
 Are there likely to be important differences in the baseline conditions between where the research was done and other settings Are there important differences in perspectives and influences of health system stakeholders between where the research was done and where it could be applied that might mean an intervention will not be accepted or taken up in the same way")
58
Geriatric research-Statistical challenges
Multicomponent interventions Clinical trial design Multiple outcomes Multiple testing procedures State transitions Longitudinal transitions models Floor and ceiling effects Item respons Theory methods and regression models Missing data Qualitative and quantitative data Mixed methods

59
How is real life? J Latour & al. Short term geriatric assessment units: 30 years later. BMC Geriatrics 2010, 10:40

64
Takk for meg

Similar presentations




























 Grants Chapter 6.>")