Download presentation
Presentation is loading. Please wait.

1
An Overview of Oral Medicine

2
WHAT IS ORAL MEDICINE? “The specialty of dentistry concerned with the oral health care of patients with chronic, recurrent and medically related disorders of the oral and maxillofacial region, and with their diagnosis and non-surgical management.”

3
Some conditions are very common e. g
Some conditions are very common e.g. mouth ulcers, white patches and infections (usually viral and fungal) Some conditions are very distressing e.g. orofacial granulomatosis and Sjogren’s syndrome Some conditions are persistent and difficult to manage e.g. psychogenic facial pain
 Some conditions are very distressing e.g. orofacial granulomatosis and Sjogren’s syndrome. Some conditions are persistent and difficult to manage e.g. psychogenic facial pain.")
4
The mouth - what’s it got to do with medicine?
An entity in its own right – dentistry ! The upper end of the GIT- gastroenterology ! In continuity with the skin – dermatology ! Often reflects haematological problems at an early stage Oral mucosa not dissimilar to genital mucosa – combinations of oral, genital and conjunctival problems occur Can frequently be affected by side effects of medication – dryness, ulceration, pigmentation etc. Has a lot of sensory cortex devoted to it - oral problems are often very distressing– psychiatry !

5
Which One Is Potentially Serious

6
Three key questions What is it ? What is its significance ?
What should be done about it ?

7
What is it ? History Examination Investigations Biopsy Haematological
Imaging Etc

8
What is its significance ?
Local (single/multiple) General (systemic) Benign (nuisance) Malignant (serious) A Syndrome
 General (systemic) Benign (nuisance) Malignant (serious) A Syndrome.")
9
What should be done about it ?
Leave +/- review Treat Refer

10
Surgical sieve Congenital – developmental , hereditary/familial
Traumatic - physical/chemical/thermal Inflammatory – acute / chronic Neoplastic – benign / malignant Other

11
History and investigation (eg. Biopsy) are often essential
Oral mucosa Limited ways it can react to an insult It can breakdown – (ulceration) It can thicken – (white patches) It can blister – (vesiculobullous disorders) It can pigment – (eg. with melanin) Consequently many oral disorders can appear very similar ! History and investigation (eg. Biopsy) are often essential
 It can thicken – (white patches) It can blister – (vesiculobullous disorders) It can pigment – (eg. with melanin) Consequently many oral disorders can appear very similar ! History and investigation (eg. Biopsy) are often essential.")
12
Oral Ulceration

13
Causes of Oral Ulceration
Traumatic Recurrent aphthous stomatitis Viral disease Dermatological conditions Malignancy

14
Traumatic Mechanical (toothbrush, dentures) Chemical (aspirin burn)
Thermal (pipe smoking, hot food)
")
15
Traumatic Mechanical (toothbrush, dentures) Chemical (aspirin burn)
Thermal (pipe smoking, hot food)
")
16
Traumatic Mechanical (toothbrush, dentures) Chemical (aspirin burn)
Thermal (pipe smoking, hot food)
")
17
Management of traumatic oral ulceration
Try to identify and remove the cause Review in 2 weeks If not healed, reconsider diagnosis e.g. if it is a solitary ulcer, consider carcinoma and requires biopsy

18
Recurrent Aphthous Stomatitis
Occurs in 20% of the population Definite cause unknown, but some precipitating factors or triggers have been identified Mainly “minor aphthous stomatitis” (80%) but also “major” & “herpetiform” (20%) stomatitis
 but also major & herpetiform (20%) stomatitis.")
19
Minor RAS < 1cm round/oval ulcers - painful
Occur in crops, variable with ulcer free periods Last up to 10 days & heal without scarring Never occur on keratinised mucosa (hard palate or attached gingiva)
")
20
Major Aphthous Ulceration
> 1cm, irregular, deep ulcers Heal after several weeks with scarring Destructive Occur anywhere on the oral mucosa Can mimic malignancy!

21
Aetiology Idiopathic Complex genetic (multifactorial) disease Genetic
hypersensitivity Stress/ Smoking cessation Hormonal Microbial (Viral?)
")
22
RAS……known triggers Haematinic deficiency in 20%, with 60% positive response following appropriate supplementation Check Hb, ferritin, Vit.B12 & Folate Psychological factors Allergies (preservatives e.g. benzoic acid E ), fizzy drinks
, fizzy drinks.")
23
Trauma (penetrating) (crisps, also preservatives!)
Cessation of smoking (reverts mucosa to normal non-keratinised state) Drugs Family history (not genetic) Endocrine Immunological factors No microbiological association
 Drugs. Family history (not genetic) Endocrine. Immunological factors. No microbiological association.")
24
Bowel problems associated with RAS
Crohn’s disease Ulcerative colitis Coeliac disease

25
Gluten Enteropathy – Coeliac Disease
Allergy to wheat products Starts during early childhood - weaning Lose villi Malabsorption Fatty stools – steatorrhoea Failure to thrive Aphthous ulcers (Dermatitis herpetiformis)
")
26
Systemic history for RAS
Lassitude Weakness Breathlessness Abdominal pain Frequency and type of stool Weight loss ANAEMIA GIT problems

27
Management of RAS Confirm diagnosis by eliminating any systemic underlying cause Check for haematinic deficiency If suspect systemic involvement refer to specialist Therapy How severe are the symptoms How frequent are the ulcers Location of the ulcer

28
Treatment options No treatment
Prevention/treatment of/for possible causes Sodium Lauryl Sulfate-Free Toothpastes Sharp edges, ill fitting prosthesis, calculus Topical therapy Systemic therapy Referral for severe disease

29
RAS management Pain relief – lignocaine lollipops, Gengigel, Aloclair, Difflam Address precipitating factors e.g. replacement therapy & investigation of underlying cause. Often asking children to eliminate (individually) fizzy drinks, crisps & chocolate helps Treatment can include Corlan pellets, steroid in orobase (protects and a small amount of steroid) Tetracycline mouthwash in adults (not pregnant)
 fizzy drinks, crisps & chocolate helps. Treatment can include Corlan pellets, steroid in orobase (protects and a small amount of steroid) Tetracycline mouthwash in adults (not pregnant)")
30
Gengigel (Hyaluronic acid) gives good pain relief and accelerates healing – useful in children as non-irritant More severe cases require a steroid inhaler or betnesol mouthwashes (occasional use) Systemic steroids on rare occasions (short course)
 Systemic steroids on rare occasions (short course)")
31
Systemic therapy Prednisolone Immunomodulator
Burst therapy (5-30mg once in morning for 5 days) Immunomodulator Azathioprine Colchicine Thalidomide (TNF- inhibitor)
 Immunomodulator. Azathioprine. Colchicine. Thalidomide (TNF- inhibitor)")
32
Guidelines for prescribing topical steroids for oral lesions
Topical medications are effective on contact therefore anything by mouth should be avoided for ½ -1 hr Gel applied directly on lesion after meals & at bedtime 3-4 times daily Could apply it on gauze for large lesions for min

33
Guidelines for prescribing systemic steroids for oral lesions
Tapering of prednisolone is not necessary with 5-7 days burst therapy Tapering of prednisone is not necessary with alternate day therapy if dose did not exceed 20 mg 30-60 mg AM X 5 days followed by 5-20 mg AM every other day

34
Behcet’s Syndrome RAS Ocular – uveitis,optic atrophy,retinal vasculitis Genital ulceration Dermatological eg. Pustules Neurological – symptoms like MS Joint disease – recurrent arthralgia Others – eg.depression Strong association with HLA B5

35
Epidemiology The usual onset of the disease is in the third and fourth decade of life. Male to female ratio is approximately equal.

36
Epidemiology Prevalence in Turkey 80-370:100,000
Prevalence in UK ( ):100,000
:100,000.")
37
Behcet’s Affects persons of Mediterranean, Middle Eastern, or Japanese decent Easily confused with Stevens-Johnson syndrome or Reiter’s disease Need referral for systemic treatment

38
Treatment Multidisciplinary approach Systemic therapy Corticosteroid
Azathioprine Colchicine Thalidomide (TNF- inhibitor)
")
39
Viral Oral Ulceration Tends to be all over the mouth, including keratinised epithelium Usually extensive ulceration If primary HSV, may be preceded by flu-like illness and no previous history of cold sores If secondary HSV, should be history of cold sores

40
Dermatological causes of oral ulceration
Lichen planus Lupus Vesiculobullous disorders Erythema multiforme

41
Oral Lichen Planus A common chronic inflammatory mucocutaneous disorder which affects the skin and mucous membranes (mainly mouth) Occurs in approximately 1% of the population, usually in middle age and is slightly more common in females

42
Clinical presentation
Reticular – often symptoms of roughness rather than pain Papular – raised white areas of 1-2mm in diameter Plaques – homogeneous leukoplakia, more usual in smokers Atrophic – thin mucosa, red but not ulcerated and often painful Erosive – frank painful ulcers Bullous – vesicles or small blisters within white patches

43
Ulcerative Lichen Planus
Erosive or desquamative types Intermittent ulcers for up to 20 years If unilateral may be lichenoid - ? Related to old amalgam or other contact allergy Can be drug related Usually striae present

44
If lichenoid try to eliminate allergen, whereas treat LP symptomatically & attempt to eliminate ulceration Attempt to maintain intact mucosa i.e. revert to white patch or striae Use potent steroids with caution in case of potential risk of malignant change

45
OLP – malignant transformation risk
Erosive & plaque variants ~ 1% over 5-10 year period Dysplastic lichen planus

46
Lupus Discoid (DLE) Systemic (SLE) “Butterfly” rash on face
Oral red/white patches Sunray appearance Oral ulceration Sjogren’s & TMJ disease - autoimmune Oral malignancies

47
Vesiculobullous disorders
Pemphigus Pemphigoid Erythema multiforme (also under allergy)
")
48
Pemphigus An autoimmune disorder characterised by widespread bullous or blistering eruptions of skin and mucous membranes Potentially fatal as there is gross loss of fluids and electrolytes as well as wound infections 70% present in mouth first (50% in mouth only)
")
49
Usually the elderly Rarely see blisters – usually irregular ulcers and skin tags Usually on areas of pressure (e.g. denture) May present as a sore throat Ulcers differ from RAS as bigger, present in older people and are persistent. Most common type of oral presentation is P. vulgaris Need to treat for life as potentially fatal and autoimmune.

50
Pemphigus Not easily distinguished from pemphigoid, which is not fatal, but can cause blindness as can involve eyes and scarring causes opacity (symblepharon)
")
51
Mucous Membrane Pemphigoid vs. Bullous Pemphigoid
BP mainly affects skin with occasional mucosal involvement Elderly (>60) Starts with pruritus then fluid filled bulla develop 20% shows oral lesions (desquamative gingivitis) 51
 Starts with pruritus then fluid filled bulla develop. 20% shows oral lesions (desquamative gingivitis) 51.")
52
Desquamative Gingivitis
Hypersensitivity Lichen planus Pemphigoid or pemphigus Requires good oral hygiene!

53
Soft palate usually involved Unknown cause
Idiopathic oral blood blisters (angina bullosa haemorrhagica) Clinical presentation Sudden onset Soft palate usually involved Unknown cause Eating Dental treatment Self limiting 53
 Clinical presentation. Sudden onset. Soft palate usually involved. Unknown cause. Eating. Dental treatment. Self limiting. 53.")
54
Erythema Multiforme An acute, self limiting eruption of the skin and mucous membranes Antigen can be HSV, EBV, Mycoplasma, sulphonamides, phenytoin, other drugs (including alcohol) May be prodromal flu-like symptoms followed by widespread vesiculobullous eruptions of skin, oral, genital & ocular mucosa
 May be prodromal flu-like symptoms followed by widespread vesiculobullous eruptions of skin, oral, genital & ocular mucosa.")
55
Ulcers all over mouth and lips (crusting)
Skin lesions are either bullous or “target” lesions Usually resolves in days Management is supportive – no particular diagnostic test or treatment (topical anaesthetic & betnesol mouthwash). Ensure fluid intake is adequate Recurs, but each episode is less severe Severe form is Stevens – Johnson Syndrome
. Ensure fluid intake is adequate. Recurs, but each episode is less severe. Severe form is Stevens – Johnson Syndrome.")
56
Importance of History in Oral Ulceration
Have the patients had previous ulcers and are they cyclical or persistent Age of patient Site of ulcers - ? On keratinised or non-keratinised mucosa Has the patient had herpes in the past? Has the patient any known allergies?

57
Does it involve any other mucosal sites?
Has the patient started new drugs that preceded onset of ulcers Has the patient stopped smoking Is the patient in generally good health

58
Diffuse Lip Swelling Orofacial Granulomatosis Allergic angioedema
Hereditary angioedema

59
Orofacial Granulomatosis
Lip swelling Oral ulceration Mucosal tags Angular cheilitis Cobblestone mucosa Full-width gingivitis

60
Causes of OFG Allergy Crohn’s disease – may not manifest itself until 10 years after onset of OFG! Others – foreign bodies, sarcoidosis

61
Investigations of OFG FBC, B12, Red cell folate, ferritin, LFT’s, CRP
Buccal mucosal biopsy down to muscle Patch testing (Type 4 hypersensitivity) GIT investigations (?Crohn’s)
 GIT investigations ( Crohn’s)")
62
Most common allergens identified on patch testing in OFG are benzoic acid (E ) found in fizzy drinks and tomatoes & cinammonaldehyde Chocolate is commonly a cause Negative patch tests do not confirm absence of allergy

63
Allergic Angioedema Type 1 Hypersensitivity
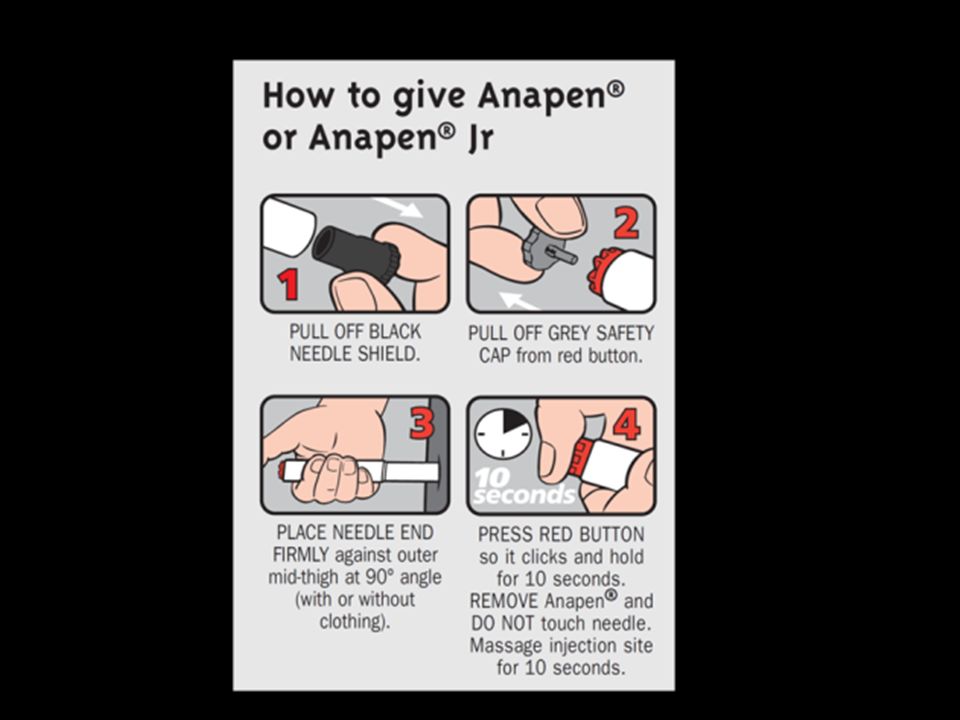
Speed of onset Swelling of lips, cheeks, tongue, throat, itch within minutes Oedema of larynx, GIT involvement (vomiting & diarrhoea), urticaria, vasodilatation & bronchospasm Adrenaline (followed by hydrocortisone) is required for bronchospasm & acute drop in BP
, urticaria, vasodilatation & bronchospasm. Adrenaline (followed by hydrocortisone) is required for bronchospasm & acute drop in BP.")
64
Management Tests: Skin prick tests & RAST (Radioallergosorbent test)
Control by: Avoidance of allergen Antihistamines in mild cases and adrenaline/steroids in severe cases

66
Hereditary Angioedema
Hereditary (more common) or acquired (usually in middle age) angioedema Genetic defect of inhibitor of first component of C1 (C1 esterase inhibitor) Repeated episodes of swelling of deep dermis, subcutaneous tissues and mucous membranes Uncontrolled activation of classical complement pathway & excess release of vasoactive agents
 or acquired (usually in middle age) angioedema. Genetic defect of inhibitor of first component of C1 (C1 esterase inhibitor) Repeated episodes of swelling of deep dermis, subcutaneous tissues and mucous membranes. Uncontrolled activation of classical complement pathway & excess release of vasoactive agents.")
67
Clinical manifestations
Swelling poorly circumscribed, no-pitting and not associated with urticaria or pruritis Precipitated by trauma (including dentistry) anxiety, emotional upset, physical exertion and sometimes spontaneously Develops over hours with tingling and tightness and usually over hours
 anxiety, emotional upset, physical exertion and sometimes spontaneously. Develops over hours with tingling and tightness and usually over hours.")
68
Involves the extremities, face, oropharynx and can compromise the airway
Treatment: stanazol (androgenic steroid) or antifibrinolytics 1 week before planned dentistry Emergency dental treatment may require fresh frozen plasma Rarely responds to antihistamines or steroids
 or antifibrinolytics 1 week before planned dentistry. Emergency dental treatment may require fresh frozen plasma. Rarely responds to antihistamines or steroids.")
69
Intraoral White Patches

70
Leukoplakia Clinical term for persistent adherent white patch (histology unknown and no attributable diagnosis) Prevalence of keratosis is 3-4% 15% of leukoplakias regress and 3-6% undergo malignant transformation over 10 years

71
Leukoplakia Homogenous leukoplakias are prevalent in the buccal mucosa and have a low pre-malignant potential Nodular or speckled leukoplakias are more serious Leukoplakias in the floor of mouth or undersurface of tongue have a high risk of malignant change

72
Risk factors Smoking Alcohol Diet Immunosuppression
Presence of Candida

73
Local Causes Frictional keratosis Smokers keratosis
Idiopathic keratosis Papillomas Carcinomas Burns Skin grafts

74
Systemic causes White sponge naevus Geographic tongue
Lichen planus / lupus erythematosis Candidosis / candidal leukoplakia Hairy leukoplakia

75
Biopsy of lesions To confirm diagnosis
Essential in non-healing ulcerated areas, nodular areas, areas with red flecks, if there are associated lymph nodes, in “at risk” sites or at risk patients or if the white patch is fixed and indurated

76
Mucosal Biopsy Should it be undertaken in general dental practice?
Yes it could be with: Being interested in minor OS procedures Adequate training Good links with a pathology service Good resource to feed back results ( & implications) to patient But no if any suspicion of oral cancer
 to patient. But no if any suspicion of oral cancer.")
77
Management of Leukoplakia
Biopsy and other investigations Reduction of pre-disposing factors Definitive management e.g. excision, laser or regular review with records and re-biopsy

78
Papillomas Keratinised papillomas appear as white nodules
Commonly appear like cauliflowers, frequently on soft palate Diagnosis is obvious, but biopsy is recommended in case they are the more rare venereal wart intraorally

79
White Sponge Naevus Benign, hereditary mucosal condition of no consequence Very roughened “shaggy Carpet” appearance Some reports of improvement with antibiotics

80
Geographic Tongue Also known as benign migratory glossitis & erythema migrans Red and white patches that change position from time to time White patches are hyperkeratinised areas and red the atrophic areas Often associated with fissures and can be painful Treat symptomatically (? Use of zinc)
")
81
Oral Candidosis Clinical types that are white are pseudomembranous, occasionally midline glossitis and candidal leukoplakia (premalignant) Management by addressing underlying cause such as dietary deficiency, excess sugar in diet, denture hygiene, use of steroid inhalers or identification of underlying cause

82
Oral Candidosis Management:
address underlying cause e.g. dietary deficiency, excess sugar in diet, denture hygiene, use of steroid inhalers or identification of underlying cause

83
Oral Hairy Leukoplakia
EBV – has been implicated in the aetiology of hairy leukoplakia OHL is useful prognostic indicator in HIV and can also be seen in immunosuppressed transplant patients

84
Salivary Problems Saliva plays an essential role in numerous functions of the mouth. Usual complaint is of dryness Can c/o too much – sialorrhoea Sore mouth Neurological – poor neuromuscular co-ordination etc. Medication Psychogenic

85
Sjögren’s syndrome A common autoimmune “rheumatic” disease.
Women >40 yo Can occur on its own (primary) or as a complication of other connective tissue diseases (secondary Sjögren’s syndrome). The most common symptoms are extreme tiredness, along with dry eyes (keratoconjunctivitis sicca) and dry mouth (xerostomia). Up to 90% of individuals with Sjögren’s syndrome have antibodies targeting the Ro and La autoantigens Can have other systemic symptoms – GIT, vulval etc.
 or as a complication of other connective tissue diseases (secondary Sjögren’s syndrome). The most common symptoms are extreme tiredness, along with dry eyes (keratoconjunctivitis sicca) and dry mouth (xerostomia). Up to 90% of individuals with Sjögren’s syndrome have antibodies targeting the Ro and La autoantigens. Can have other systemic symptoms – GIT, vulval etc.")
86
Diagnostic criteria for S.S (European/American & Japanese)
Ocular symptoms Oral symptoms Ocular signs Histopathology Salivary gland involvement Salivary flow Parotid sialography Salivary scintigraphy Autoantibodies E.g. dry eyes and mouth for 3/12 Requires a score to meet the Diagnostic criteria – see Ann Rheum Dis 2002;61:54-558

87
General complications
Caries (often rampant) Periodontal disease Candidosis – should be checked ! Bacterial sialadenitis ulceration
 Periodontal disease. Candidosis – should be checked ! Bacterial sialadenitis. ulceration.")
88
Non-Hodgkin’s B-cell lymphoma
Occurs in ~1% of patients with Sjögren’s syndrome. Usually, this is a slow growing, low-grade malignancy Pseudolymphoma in ~10%

89
Xerostomia Clinical History Hx Radiotherapy Radiation Xerostomia
Dry mouth N Y Primary S.S Secondary S.S Reduced saliva flow N Y Pharmacological Xerostomia Connective Tissue Disorder Medication N Y European & American Guidelines for Sjogren’s Syndrome Dry Eyes

90
Management Identify a likely cause! Referral Artificial saliva
Oral medicine – Sjogren’s syndrome? Rheumatology Ophthalmology Artificial saliva Salivary stimulating agents (gum, pilocarpine) Meticulous oral hygiene management Regular dental care
 Meticulous oral hygiene management. Regular dental care.")
91
Summary The mouth can be a useful site for early diagnosis of systemic disease Painful conditions of the orofacial region can be debilitating and lead to nutritional and fluid intake problems Because of its constant use the mouth is exposed to trauma, allergens and carcinogens and must be checked routinely.

Similar presentations











 Pathogenesis` (Mechanisms:inflammation) Clinical Features (Signs and Symptoms) Fever,>")






 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")
