Download presentation
Presentation is loading. Please wait.

1
Block 11 Board Review Part 1 of 4
Neurology/Heme-Onc 11April2014 Chauncey D. Tarrant, M.D. Chief of Residents 13-14

2
3% of Initial Certifying Exam!!!

3
Pediatrics In Review Articles
Headaches Encephalitis

4
PIR Quiz

5
1. A 4-year-old boy comes in with a complaint of headache
1. A 4-year-old boy comes in with a complaint of headache. His father asks whether a “brain scan” should be performed. Which of the following characteristics would be the strongest indication for a magnetic resonance imaging study of this child’s brain? A. Age under 5 years. B. Detection of a slight limp on examination. C. Headache that awakens him from sleep. D. Male gender. E. Unilateral headache.

6
1. A 4-year-old boy comes in with a complaint of headache
1. A 4-year-old boy comes in with a complaint of headache. His father asks whether a “brain scan” should be performed. Which of the following characteristics would be the strongest indication for a magnetic resonance imaging study of this child’s brain? A. Age under 5 years. B. Detection of a slight limp on examination. C. Headache that awakens him from sleep. D. Male gender. E. Unilateral headache.

7
2. A 12-year-old girl presents to your office with a history of frequent headaches that sometimes make her miss school. You are trying to differentiate between migraine and tension headache. Which of the following statements is true and will help you to differentiate? A. Migraine headaches are more likely to affect boys. B. Migraine headaches are relieved by exercise. C. Migraine headaches cause a “band-like pressure” on the head. D. Migraine headaches typically last for several hours. E. Migraine pain is throbbing and severe.

8
2. A 12-year-old girl presents to your office with a history of frequent headaches that sometimes make her miss school. You are trying to differentiate between migraine and tension headache. Which of the following statements is true and will help you to differentiate? A. Migraine headaches are more likely to affect boys. B. Migraine headaches are relieved by exercise. C. Migraine headaches cause a “band-like pressure” on the head. D. Migraine headaches typically last for several hours. E. Migraine pain is throbbing and severe.

9
3. A 15-year-old girl who has just started to take acne medication presents to your office with poorly localizing daily headaches, blurry vision, and tinnitus. Of the following, which diagnosis is most likely to explain the findings above? A. Idiopathic intracranial hypertension. B. Medulloblastoma. C. Migraine headache. D. Tension headache. E. Trigeminal autonomic cephalalagia (cluster headache).
.")
10
3. A 15-year-old girl who has just started to take acne medication presents to your office with poorly localizing daily headaches, blurry vision, and tinnitus. Of the following, which diagnosis is most likely to explain the findings above? A. Idiopathic intracranial hypertension. B. Medulloblastoma. C. Migraine headache. D. Tension headache. E. Trigeminal autonomic cephalalagia (cluster headache).
.")
11
4. You are counseling a parent of a 17-year-old boy who has frequent tension headaches. The family and young man would prefer to try lifestyle interventions before proceeding to medications. Which of the following lifestyle interventions might be helpful in promoting headache reduction? A. Coffee or tea with breakfast daily. B. Limiting fluid intake to 40 ounces daily. C. Regular aerobic exercise. D. Skipping breakfast during weekends to allow for extra sleep. E. Television watching before sleep.

12
4. You are counseling a parent of a 17-year-old boy who has frequent tension headaches. The family and young man would prefer to try lifestyle interventions before proceeding to medications. Which of the following lifestyle interventions might be helpful in promoting headache reduction? A. Coffee or tea with breakfast daily. B. Limiting fluid intake to 40 ounces daily. C. Regular aerobic exercise. D. Skipping breakfast during weekends to allow for extra sleep. E. Television watching before sleep.

13
5. A 14-year-old girl has been diagnosed as having migraine
5. A 14-year-old girl has been diagnosed as having migraine. The headaches occur twice weekly and have caused her to miss school at least once per month. The family is interested in a prophylactic medication to prevent her attacks, and you plan to start amitriptyline. Of the following studies, which is indicated as part of amitriptyline therapy? A. Chest radiograph. B. Complete blood count. C. Electrocardiogram. D. Serum alanine aminotransferase. E. Serum creatinine.

14
5. A 14-year-old girl has been diagnosed as having migraine
5. A 14-year-old girl has been diagnosed as having migraine. The headaches occur twice weekly and have caused her to miss school at least once per month. The family is interested in a prophylactic medication to prevent her attacks, and you plan to start amitriptyline. Of the following studies, which is indicated as part of amitriptyline therapy? A. Chest radiograph. B. Complete blood count. C. Electrocardiogram. D. Serum alanine aminotransferase. E. Serum creatinine.

15
1. Mosquito control will most likely reduce the frequency of encephalitis caused by A. Adenoviruses. B. Flaviviruses. C. Herpesviruses. D. Myxoviruses. E. Picornaviruses.

16
1. Mosquito control will most likely reduce the frequency of encephalitis caused by A. Adenoviruses. B. Flaviviruses. C. Herpesviruses. D. Myxoviruses. E. Picornaviruses.

17
2. A 10-year-old child presents with the signs of acute encephalitis
2. A 10-year-old child presents with the signs of acute encephalitis. While no pattern of brain involvement is exclusively produced by a single microbiologic agent, the possibility of herpes simplex being the causative agent is enhanced substantially by an MRI finding of lesions concentrated in the A. Basal ganglia. B. Frontal lobes. C. Midbrain. D. Temporal lobes. E. Thalamus.

18
2. A 10-year-old child presents with the signs of acute encephalitis
2. A 10-year-old child presents with the signs of acute encephalitis. While no pattern of brain involvement is exclusively produced by a single microbiologic agent, the possibility of herpes simplex being the causative agent is enhanced substantially by an MRI finding of lesions concentrated in the A. Basal ganglia. B. Frontal lobes. C. Midbrain. D. Temporal lobes. E. Thalamus.

19
3. A 17-year-old boy has acute encephalitis associated with weakness in the right arm. He is clinically stable. He had experienced a febrile illness 3 weeks before presenting with signs of encephalitis, but had apparently recovered fully. An MRI demonstrated scattered multifocal abnormalities in both gray and white matter within the brain. Evaluation of serum and CSF has been unrevealing. His most likely diagnosis is A. Acute disseminated encephalomyelitis. B. Enteroviral encephalitis. C. Herpes simplex encephalitis. D. Mycoplasma encephalitis. E. Multiple sclerosis.

20
3. A 17-year-old boy has acute encephalitis associated with weakness in the right arm. He is clinically stable. He had experienced a febrile illness 3 weeks before presenting with signs of encephalitis, but had apparently recovered fully. An MRI demonstrated scattered multifocal abnormalities in both gray and white matter within the brain. Evaluation of serum and CSF has been unrevealing. His most likely diagnosis is A. Acute disseminated encephalomyelitis. B. Enteroviral encephalitis. C. Herpes simplex encephalitis. D. Mycoplasma encephalitis. E. Multiple sclerosis.

21
4. The form of encephalitis shown to benefit most from the use of high-dose glucocorticosteroids is A. Acute disseminated encephalomyelitis. B. Enteroviral encephalitis. C. Herpes simplex encephalitis. D. Saint Louis encephalitis. E. West Nile virus encephalitis.

22
4. The form of encephalitis shown to benefit most from the use of high-dose glucocorticosteroids is A. Acute disseminated encephalomyelitis. B. Enteroviral encephalitis. C. Herpes simplex encephalitis. D. Saint Louis encephalitis. E. West Nile virus encephalitis.

23
5. The likelihood of full recovery from encephalitis most depends upon A. Availability of specific treatment. B. Causative agent. C. Duration of fever. D. Initial CSF findings. E. Timeliness of specific diagnosis.

24
5. The likelihood of full recovery from encephalitis most depends upon A. Availability of specific treatment. B. Causative agent. C. Duration of fever. D. Initial CSF findings. E. Timeliness of specific diagnosis.

25
Headaches

26
What are the physical characteristics of a headache due to increased ICP?

27
What are the physical characteristics of a headache due to increased ICP?
progressive may cause nighttime wakening are worse with the Valsalva maneuver or exertion. persistent vomiting neurologic deficits Lethargy personality change Papilledema Palsies of the third, fourth, or sixth cranial nerves, resulting in eye movement or pupillary abnormalities

28
What elements of the history characterize a migraine?

29
What elements of the history characterize a migraine?
Migraine without aura A. At least five attacks fulfilling criteria B–D B. Headache attacks lasting 1–72 hours (untreated or unsuccessfully treated) C. Headache has at least two of the following characteristics: 1. Unilateral location, although may be bilateral or frontal (not exclusively occipital) in children 2. Pulsing quality 3. Moderate or severe pain intensity 4. Aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs) D. During headache at least one of the following: 1. Nausea and/or vomiting 2. Photophobia and phonophobia (which may be inferred from behavior) E. Not attributed to another disorder
 C. Headache has at least two of the following characteristics: 1. Unilateral location, although may be bilateral or frontal (not exclusively occipital) in children 2. Pulsing quality 3. Moderate or severe pain intensity 4. Aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs) D. During headache at least one of the following: 1. Nausea and/or vomiting 2. Photophobia and phonophobia (which may be inferred from behavior) E. Not attributed to another disorder")
30
What neurologic defects can be associated with a migraine?

31
What neurologic defects can be associated with a migraine?
Acute confusional state Benign paroxysmal vertigo Benign paroxysmal torticollis Cyclic vomiting Hemiplegic migraine Basilar Ophthalmoplegic Retinal Alice-In-Wonderland

32
What elements of the history characterize a headache due to stress/tension/emotion?

33
What elements of the history characterize a headache due to stress/tension/emotion?
may last for 1 hour or for several days described as “band-like,” pressure, or tightening Triggers include stress, fatigue, illness, muscle pain, tension, particularly in the neck and shoulders may be episodic (<15 days per month) or chronic (>15 days per month)
 or chronic (>15 days per month)")
34
Can depression cause headaches? T or F

35
Can depression cause headaches? T or F

36
What elements of the history characterize a headache due to increased ICP?

37
What elements of the history characterize a headache due to increased ICP?
Progressive causes nighttime wakening worse with the Valsalva maneuver or exertion. persistent vomiting neurologic deficits Lethargy personality change Papilledema Palsies of the third, fourth, or sixth cranial nerves, resulting in eye movement or pupillary abnormalities

38
What signs and symptoms of a headache indicate follow-up with MRI or CT scan?

39
What signs and symptoms of a headache indicate follow-up with MRI or CT scan?

40
What are the values and limitations of ancillary neurodiagnostic tests when evaluating headaches?

41
What are the values and limitations of ancillary neurodiagnostic tests when evaluating headaches?
Brain MRI can help investigate potential structural abnormalities, infection, inflammation, and ischemia CT is good if there is a concern for hemorrhage or fracture Limitations No good guidelines to use

42
What are some abortive treatments for acute migraines?

43
What are some abortive treatments for acute migraines?
Tylenol Ibuprofen Naproxen Triptans

44
How do you treat a stress/tension/emotion headache?

45
How do you treat a stress/tension/emotion headache?
Modification of lifestyle (sleep, hydration, stressors, etc) Acute treatments
 Acute treatments.")
46
What are complications of using narcotics, sedatives, and NSAIDS when treating chronic or recurrent headaches?

47
What are complications of using narcotics, sedatives, and NSAIDS when treating chronic or recurrent headaches? Rebound headaches

48
What are prophylactic treatments for recurrent migraines?

49
What are prophylactic treatments for recurrent migraines?
Periactin TCAs AEDs Antihypertensives Supplements Riboflavin Melatonin Coenzyme Q

50
Encephalitis

51
What are the common causes of encephalitis?

52
What are the common causes of encephalitis?
Infectious (viral, bacterial, fungal, parasitic) Parainfectious/Immune Mediated (ADEM, acute cerebellar ataxia) Systemic Infalmmatory (Lupus) Malignancy (paraneoplastic)
 Parainfectious/Immune Mediated (ADEM, acute cerebellar ataxia) Systemic Infalmmatory (Lupus) Malignancy (paraneoplastic)")
53
What are the signs and symptoms of herpes encephalitis?

54
What are the signs and symptoms of herpes encephalitis?
Basal frontal and mesial temporal lobes with prominent lesions on MRI in older children and adults Hemorrhagic meningoencephalitis >50% ofcases in individuals >20 y causes up to 30% of neonatal meningoencephalitis

55
What are the clinical symptoms of encephalitis?

56
What are the clinical symptoms of encephalitis?
Seizures, upper-motor-neuron weakness Sensory disturbances Lethargy coma Weakness, hyperkinetic (dystonia, choreoathetosis) or parkinsonian movement abnormalities, apathetic or disinhibited behavior Salt and water disturbances (eg, syndrome of inappropriate antidiuretic hormone, diabetes insipidus) adrenal and thyroid failure Paroxysmal autonomic dysfunction postural abnormalities
 or parkinsonian movement abnormalities, apathetic or disinhibited behavior. Salt and water disturbances (eg, syndrome of inappropriate antidiuretic hormone, diabetes insipidus) adrenal and thyroid failure. Paroxysmal autonomic dysfunction. postural abnormalities.")
57
What is the role of neurodiagnostic testing in the evaluation of a child with encephalitis?

58
What is the role of neurodiagnostic testing in the evaluation of a child with encephalitis?
LOCALIZATION! MRI can yield false negative results early in course CT for identifying substantial cerebral edema, midline shift or hemorrhage Generally not sufficient for workup

59
What diagnostic tests are useful in a child with encephalitis?

60
What diagnostic tests are useful in a child with encephalitis?
MRI (with and without contrast) CBC, CMP, UA LP Acute treatment if indicated* EEG*
 CBC, CMP, UA. LP. Acute treatment if indicated* EEG*")
61
How do you manage encephalitis?

62
How do you manage encephalitis?
Supportive care, unless causative agent is identified

63
What are some common sequelae of encephalitis?

64
What are some common sequelae of encephalitis?
Depends on causative agent Can have neuro deficits or none at all

65
PREP

66
A 10-year-old boy is at school when his teacher notices that he is staring out the window. She can’t get him to stop staring or respond to her, so he is brought to the emergency department. No other children had similar symptoms. On arrival, his physical examination reveals a temperature of 37.2°C, blood pressure of 100/60 mm Hg, heart rate of 85 beats/min, and a respiratory rate of 20 breaths/min. The boy is awake and seems restless. He follows one-step commands (eg, “take off your shoes”), but does not follow two-step commands. He knows his name, but not where he is. The remainder of the physical examination findings is unremarkable. Results of computed tomography of the head without contrast, serum sodium and glucose, and serum and urine toxicology testing are normal. As you are completing your examination, the boy’s parents arrive and report no known ingestions at home, no history of seizures or headaches, and no similar prior events. The boy is adopted and no family history is known. After 2 hours of observation, he is alert and responding normally to commands, but complains of a headache and vomits. Of the following, the MOST likely diagnosis is

67
A. acute psychosis B. carbon monoxide poisoning C. confusional migraine D. postictal state E. pseudotumor cerebri

68
B. carbon monoxide poisoning C. confusional migraine
A. acute psychosis B. carbon monoxide poisoning C. confusional migraine D. postictal state E. pseudotumor cerebri PREP Pearls Confusional migrane is characterized by an abrupt onset of altered consciousness. Initial evaluation of altered level of consciousness could include serum chemistries, toxicology, infectious evaluation, or central nervous system imaging based on the history and physical examination.

69
A 3-year-old girl suddenly refuses to walk
A 3-year-old girl suddenly refuses to walk. There is no reported history of injury or ingestions. She has been well, although several children in her preschool class have been absent because of illness. Physical examination shows a temperature of 37.8°C, blood pressure of 88/62 mm Hg, heart rate of 96 beats/min, and respiratory rate of 20 breaths/min. She is crying loudly but calms down when her mother holds her. The girl’s neck is supple and there are no skin lesions. Her neurologic examination shows conjugate eye movements in all directions. She has strong, symmetric facial movements when crying and strong, symmetric limb movements when she is resisting examination. After being calmed again, her deep tendon reflexes are found to be absent. She can sit independently, but, when placed standing, she wobbles, immediately adopts a wide-based stance, refuses to take steps, and collapses to the floor while crying. Results of magnetic resonance imaging of the brain with and without contrast are normal. Of the following, the MOST likely diagnosis is

70
A. acute cerebellar ataxia B. ataxia telangiectasia C
A. acute cerebellar ataxia B. ataxia telangiectasia C. Friedreich ataxia D. Guillain-Barré syndrome E. opsoclonus-myoclonus-ataxia syndrome

71
A. acute cerebellar ataxia B. ataxia telangiectasia C
A. acute cerebellar ataxia B. ataxia telangiectasia C. Friedreich ataxia D. Guillain-Barré syndrome E. opsoclonus-myoclonus-ataxia syndrome PREP Pearls Acute cerebellar ataxia is a common cause of acute ataxia in toddlers generally considered postviral. Diagnostic evaluation for acute ataxia should include brain imaging to evaluate for acute stroke or tumor. Computed tomography is the best modality in an unstable patient but magnetic resonance imaging will give more information.

72
A 16-year-old boy has had constant daily headache for 1 month
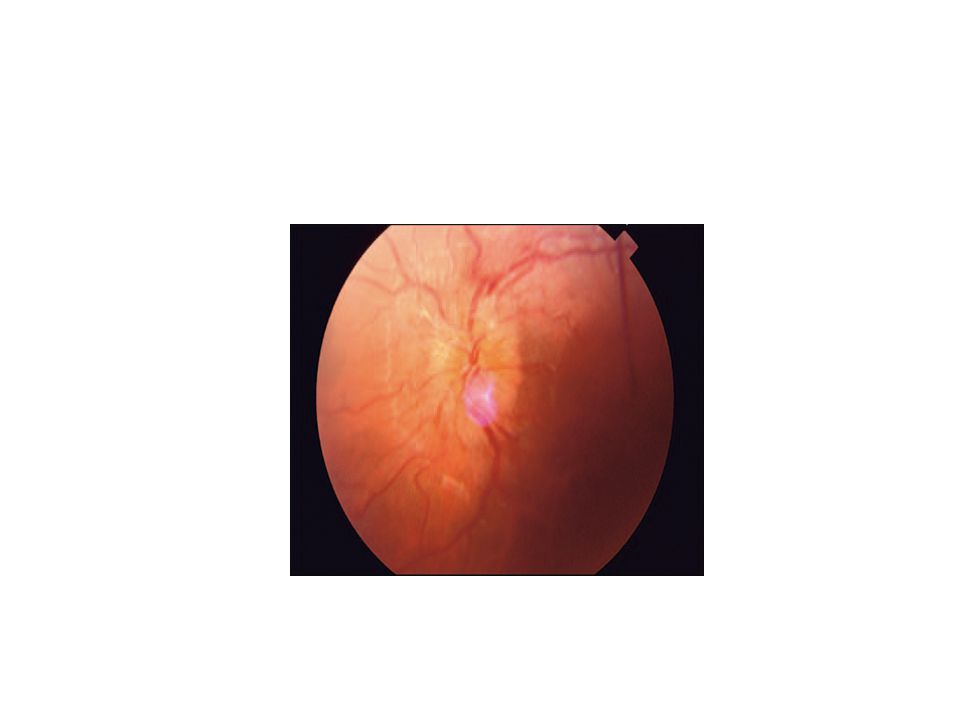
A 16-year-old boy has had constant daily headache for 1 month. The headache is all over his head; it comes and goes but never fully resolves. The pain worsens with coughing, sneezing, and laughing. He has mild nausea and photophobia and ringing in his ears. He reports that his vision “grays out” sometimes but he does not have tunnel vision or visual loss. His past medical history is notable for acne, asthma, and attention-deficit/hyperactivity disorder (ADHD). He is currently taking oral isotretinoin for his acne, oral montelukast and inhaled fluticasone for his asthma, and atomoxetine for his ADHD. He also takes vitamin B12 supplements and riboflavin as natural remedies for headache. There is no family history of migraine. On physical examination, his weight is 65 kg, height is 178 cm, and blood pressure is 102/76 mm Hg. His funduscopic examination is shown in Item Q102 (both eyes exhibit similar findings). The remainder of his physical examination findings is normal. Results of magnetic resonance imaging of the brain are normal. Lumbar puncture is performed in the lateral decubitus position with legs extended, and the opening pressure is 340 mm H20. Cerebrospinal fluid protein is 13 mg/dL and glucose is 64 mg/dL, and there are 3 white blood cells/µL and 204 red blood cells/ µL. Of the following, the medication MOST likely to cause the boy’s symptoms and signs is
. He is currently taking oral isotretinoin for his acne, oral montelukast and inhaled fluticasone for his asthma, and atomoxetine for his ADHD. He also takes vitamin B12 supplements and riboflavin as natural remedies for headache. There is no family history of migraine. On physical examination, his weight is 65 kg, height is 178 cm, and blood pressure is 102/76 mm Hg. His funduscopic examination is shown in Item Q102 (both eyes exhibit similar findings). The remainder of his physical examination findings is normal. Results of magnetic resonance imaging of the brain are normal. Lumbar puncture is performed in the lateral decubitus position with legs extended, and the opening pressure is 340 mm H20. Cerebrospinal fluid protein is 13 mg/dL and glucose is 64 mg/dL, and there are 3 white blood cells/µL and 204 red blood cells/ µL. Of the following, the medication MOST likely to cause the boy’s symptoms and signs is.")
74
A. atomoxetine B. isotretinoin C. montelukast D. riboflavin E
A. atomoxetine B. isotretinoin C. montelukast D. riboflavin E. vitamin B12

75
A. atomoxetine B. isotretinoin C. montelukast D. riboflavin E
A. atomoxetine B. isotretinoin C. montelukast D. riboflavin E. vitamin B12 PREP Pearls Risk factors for developing pseudotumor cerebri include weight gain, obesity, and common medications such as isotretinoin and tetracycline. Initial diagnostic evaluation for pseudotumor cerebri includes neuroimaging followed by lumbar puncture.

76
An 8-year-old girl has had frequent, severe headaches for the past 8 months. They are bifrontal and associated with nausea, photophobia, and blurry vision. They last 2 to 3 hours and occur 1 to 2 times per week, mostly at the end of a school day. She also has asthma and attention-deficit/hyperactivity disorder. Her father and paternal aunt have migraine headaches. She is typically a good student, but lately her grades have fallen due to absenteeism caused by the headaches. On physical examination, she is a thin, slightly nervous-appearing girl. Her funduscopic examination shows crisp optic disk margins, and extraocular movements are conjugate and intact in all directions. There is no nystagmus. The remainder of her physical examination findings are normal. Of the following, the BEST prophylactic medication for her headaches is

77
A. cyproheptadine B. ergotamine C. fluoxetine D. propranolol E. topiramate

78
A. cyproheptadine B. ergotamine C. fluoxetine D. propranolol
E. topiramate Of the choices listed, cyproheptadine is the best migraine prophylaxis medication for this girl. Potential side effects such as sedation and weight gain are dose dependent, and it is often possible, in a young child, to achieve an adequate dose for migraine prevention without side effects. In addition to medications, a treatment plan for migraine prophylaxis should involve regular, restful sleep, exercise, and a healthy diet. A headache diary can help patients and families identify food triggers and other patterns that may provoke headaches. Ergotamine is an acute treatment for migraine. It is not used for prophylaxis. Selective serotonin reuptake inhibitors like fluoxetine are also not used for migraine prophylaxis. Propranolol is a b-blocker used for migraine prophylaxis but should be avoided in a patient with asthma. Topiramate is an anticonvulsant that is also used for migraine prophylaxis, but can cause weight loss. It is not the first treatment choice for the girl in the vignette.

79
A 15-year-old boy is on a wilderness trip in the desert Southwest, United States, as part of a drug and alcohol rehabilitation program. He develops a fever and stiff neck and then has a generalized seizure. He is transported urgently to the nearest emergency department. On arrival, he has another generalized seizure and is given lorazepam 4 mg intravenously. Physical examination after lorazepam administration reveals a temperature of 39.1°C, blood pressure of 150/76 mm Hg, heart rate of 130 beats/min, and respiratory rate of 14 breaths/min. He is somnolent, there are no signs of trauma, and there are no rashes or insect bites. The remainder of his physical examination findings are normal. Computed tomography of the head without contrast is normal. Lumbar puncture is performed in the lateral recumbent position with legs extended. Cerebrospinal fluid (CSF) opening pressure is 380 mm H20; CSF protein is 182 mg/dL, and glucose is 8 mg/dL; and there are 900 white blood cells/µL (81% of which are polymorphonuclear leukocytes) and 190 red blood cells/µL. Of the following, the MOST likely cause of this boy’s symptoms is

80
A. Coccidioides immitis
B. Enterovirus C. Neisseria meningitidis D. Taenia solium E. West Nile virus

81
A. Coccidioides immitis B. Enterovirus C. Neisseria meningitidis
D. Taenia solium E. West Nile virus With CSF showing a predominance of polymorphonuclear leukocytes, a bacterial cause of meningitis must be considered and treated emergently. Cerebrospinal fluid (CSF) study results can aid in a clinical diagnosis of meningoencephalitis.
 study results can aid in a clinical diagnosis of meningoencephalitis.")
82
Quick Associations

83
Papilledema. Fundus photograph shows blurring of the optic disk margin, elevation and hyperemia of the optic nerve head, and distention of the retinal blood vessels.

84
Cerebral edema. CT performed 24 hours after severe hypoxic–ischemic injury. Note the obliteration of the cerebral ventricles, the loss of gray matter–white matter differentiation, and the homogeneous “ground-glass” appearance

85
Epidural hematoma. In this patient, blunt head trauma was followed by vomiting, progressive obtundation, and decreased movement of the left arm and leg. The CT scan showed a large, lens-shaped epidural hematoma over the right hemisphere.

86
Brain abscess. CT scan demonstrates a low-density mass lesion with an enhancing rim and surrounding edema in an immunosuppressed patient with an Aspergillus abscess. Bacterial abscesses and neoplasms can present a similar CT appearance.

Similar presentations





 in Children>")













