Download presentation
Presentation is loading. Please wait.

1
ECMO, LVADs, and the ethics of innovative surgery with innovative devices
John D. Lantos M.D. Children’s Mercy Bioethics Center University of Missouri – Kansas City @COPYRIGHT 2012

2
Central tension: science v. ethics
How much to modify the science in order to meet the demands of ethics. We want progress We want to not harm people in the process’ We have our own conflicts We want to make money, get famous, be respected, earn the gratitude of suffering families, etc.

3
We regulate ourselves, sorta
Well-defined system for new drugs. Less well-defined system for new devices. No system for new operations. VADS: New operations using new devices. i.e. an ethical and regulatory morass.

4
Berlin heart A paracorporeal pulsatile device
Stroke volumes of 10, 25, 30, 50, and 60 ml Synchronous, asynchronous, and independent modes Rechargeable 5hr battery Can be used as outpatient device. Univentricular (right or left) or biventricular support.
 or biventricular support.")
7
Regulatory approvals European Union – 1996 Canada – 2009 USA – 2011
As of January 2011, 900 patients implanted worldwide with over 187 patient years of support.

8
But what do we really know?
Do we know enough? Was the approval process appropriately cautious? Or idiotically risk-averse? What will happen now? (In the US, unlike Europe or Canada, once something is approved, the free market takes over.)
")
9
Good science (gold standard): Prospective RCT
Impossible with BH: Patients are at death’s door. Often already on ECMO. Nobody would agree to be randomized.

10
So what was the basis for approval?
Berlin heart vs. an historical control group that received ECMO. ECMO group matched in age, size, and illness severity with BH group. Two cohorts, (BSA <0.7, >0.7)
")
11
Berlin Heart patients younger
Age at initiation days 0 (0%) (0%) 30d – 2yrs 20 (83%) 30 (62%) 2 to 10yrs 4 (17%) 18 (37%) 10 to 16yrs 0 (0%) 0 (0%) Berlin heart ECMO p- value
 0 (0%) d – 2yrs 20 (83%) 30 (62%) 2 to 10yrs 4 (17%) 18 (37%) 10 to 16yrs 0 (0%) 0 (0%) Berlin heart ECMO p- value.")
12
Berlin heart ECMO/ELS P-value
Age (months) Mean ± Std ± ± Median Min – Max – 43.7
 Mean ± Std 15.4 ± ± Median Min – Max –")
13
Many SAEs with BH Most prevalent SAEs major infections 56% (27/48)
major bleeding 46% (22/48) hypertension % (20/48), neurological dysfunction 29% (14/48)
 hypertension 42% (20/48), neurological dysfunction 29% (14/48)")
14
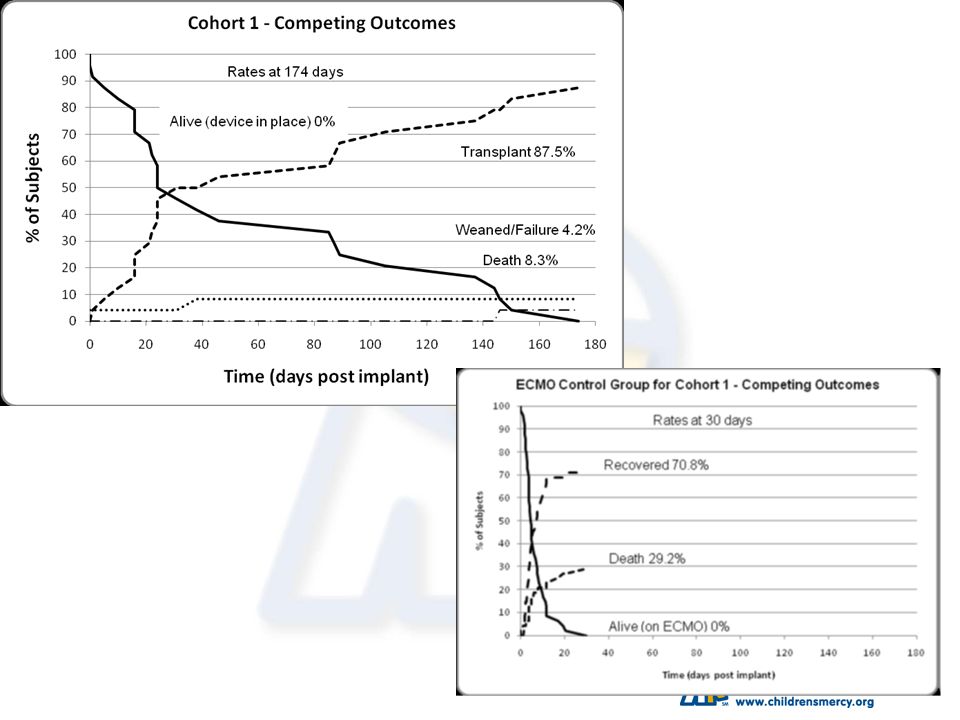
Better survival than ECMO (Cohort I – smaller babies)
")
15
Survival – Cohort II

18
Data seems compelling

19
All who drink of this treatment recover within a short time, except in those who do not.
Therefore, it fails only in incurable cases --Galen

20
The challenge How can you pick the children
A. Who would die without the BH B. Will survive with it C. Will go on to have a good QOL

21
Analogies between ECMO and the Berlin Heart (or other VADs)
")
22
Historical development of ECMO
First used in adults case report of success in NEJM, 1968 multicenter RCT - 90 patients, 9 centers, no improvement in survival. (Zapol, JAMA, 1979) Early trials in babies continued, no RCTs Bartlett had a series of papers showing improvement over historical controls.
 Early trials in babies continued, no RCTs. Bartlett had a series of papers showing improvement over historical controls.")
23
Bartlett’s survival rates
/13 “moribund” infants /16 (4 “improved”) /29 /45 /100 Many doubters demanded an RCT
 / / /100. Many doubters demanded an RCT.")
24
ECMO in the 1980s Bartlett was not in equipoise, didn’t want to “randomize babies to death” but recognized community equipoise. Developed modified study designs “play the winner” pre-randomization/modified stopping rules Results convince many doubters

25
International differences
ECMO widely adopted in the US UK did a large, prospective, multicenter, RCT.

26
Multicentre RCT in UK 180 babies Two years
Stopped early with clear benefit of ECMO

27
Results of UK trial (p = 0.0005).
30/93 (32%) ECMO infants died compared with 54/92 (59%) controls. (p = ). One child in each group has severe disability. 16 (10 ECMO, 6 controls) have lesser impairments.
 ECMO infants died compared with 54/92 (59%) controls. (p = ). One child in each group has severe disability. 16 (10 ECMO, 6 controls) have lesser impairments.")
28
The ECMO debate Was registry data enough?
Did we need the prospective RCT? Is the RCT enough? Should we do another to confirm? When do we know enough?

29
Two responses to the trial
Essential; now we really know (Silverman) Useless and unethical; we already knew (Lantos)
 Useless and unethical; we already knew (Lantos)")
30
The dilemma “How can we balance the technical challenge of perfecting hardware for life support against medicine’s humane imperative to avoid needless pain and suffering?” William Silverman, Paediatric Perinatol Epidemiolgy, 1997

31
The dilemma “At some point, we have to make a judgment about whether enough is known about a treatment to deem it better, worse, or about the same as another treatment. Lantos, Paed Perinat Epidem 1997

34
Equipoise: a contentious concept
A subject should only be submitted to a randomized, controlled design if there is substantial uncertainty about which treatment is better. Also, horse of the year in 1932!

35
The paradox of equipoise
We must be in equipoise to do an RCT. We know the efficacy of standard treatment. In order to be genuinely uncertain about the innovative treatment, we must know also know something about the innovative treatment. If we know enough to deem it equivalent, we must be able to know enough to deem it better or worse.

36
The inescapable conclusion
Equipoise presupposes the value of historical data in evaluating the safety and efficacy of therapy or the ethical acceptability of a randomized trial.

37
The way things are We always rely on historical data.
We rarely need an RCT. We do need standardized, carefully collected, complete historical data.

38
Two moral imperatives Self-reflection: Separating insecurity, grandiosity, professional aspirations, economic incentives, etc., from our obligations to do what is best for patients Transparency: Being clear, open, and honest with patients, families and colleagues about means, ends, methods, risks, uncertainties.

39
Just because it is not an RCT….
Doesn’t mean there is no… …protocol. …ethical obligation to get informed consent. …need to carefully collect and analyze data.

40
Fallacies to avoid Randomized controlled trials are the only way to know anything for sure Unexpected situations justify repeated breaches of protocol Good intentions lead to good results Tradition is always safer than innovation

Similar presentations











>")



 patients Policy.>")


: 1083-1141.>")




