Download presentation
Presentation is loading. Please wait.

1
HIGH ALTITUDE PULMONARY EDEMA
EXTREME PHYSIOLOGY HIGH ALTITUDE PULMONARY EDEMA Abundio Balgos, M.D., MHA, FPCP, FPCCP, FCCP Agatep Tolete Professor of Medicine Associate Dean for Planning and Research U.P. College of Medicine 1

2
Disclosures Currently a Professor at the College of Medicine, University of the Philippines, Manila Active Pulmonary Consultant at Manila Doctors’ Hospital and Associate Active Consultant at Makati Medical Center Has done studies, and given lectures in relation to these studies, for Astra Zeneca, Glaxo Smith Kline, Eli Lilly, Pfizer, United Laboratories, Pharmacia, Pfizer, Bayer, and Otsuka; these have no bearing on the lecture on High Altitude Diseases

3
140M people reside at altitudes >2500m
DO WE NEED TO KNOW HIGH ALTITUDE DISEASE? High altitude data: 140M people reside at altitudes >2500m There are telescopes at >5000m and mines at >4500m 30 to 50,000 workers in the Tibet railroad project worked at >4000m Skiers and mountain trekkers go to 3000m mostly, some to >8000m West, JB. Annals Intern Med, 2004, 141: 3

4
Can anyone climb Mt. Everest?
Up to 2004, Himalayan database showed that: Mt. Everest summit was reached 2251 times 130 of these ascents were without supplemental oxygen 4

5
Who really was the first Filipino to reach the summit of Mt. Everest?
Leo Oracion Erwin Emata Romy Garduce Dale Abenojar 5

6
HOW HIGH IS HIGH-ALTITUDE ?
High altitude: m above sea level Very high altitude: m Extreme altitude: above 5000m For sea level visitors, m = highest acceptable level for permanent habitation For high altitude residents, m = highest so far recorded Tibetan plateau & Himalayan valleys (8848m) Andes (6962m) Highest peak of Ethiopia : Ras Dashau Highest peak of Central Andes of Chile/Argentina : Aconcagua, Ethiopian highlands (4620m) 6
 Andes (6962m) Highest peak of Ethiopia : Ras Dashau. Highest peak of Central Andes of Chile/Argentina : Aconcagua, Ethiopian highlands (4620m) 6.")
8
2085 Palawan Mt. Mantaling 2117 Panay Mt. Madiaas 2430 Negros
Kanlaon Mountain 2938 Mindanao Mt. Katanglad 2462 Luzon Mayon Volcano 2582 Mindoro Mt. Halcon 2922 Mt. Pulog 2954m Mt. Apo 8

9
LECTURE OUTLINE Review of basic physiological principles of respiration as they relate to changes in pressure and temperature Animal and human adaptations to high altitude What happens when acclimatization fails ? Acute mountain sickness High altitude pulmonary edema High altitude cerebral edema At high altitude, respiration extracts utilizes a high proportion of the overall energy expenditure. In spite of a slight decrease in the work of breathing resulting from the lower density of the ambient air at high altitude, much greater volumes of air are necessary to supply enough oxygen to the body from atmospheric air, in which the level of oxygen is reduced. Delivery of oxygen is further impaired by a diffusion limitation of oxygen from the air to the blood, which increases with altitude. At extreme altitudes, a disabling sense of dyspnea is compounded by cerebral hypoxia, which may further limit exercise. Climbers to these heights have reported taking as many as 10 breaths per step as the rate of ascent progressively and tortuously slows. Reinhold Messner wrote of his first ascent of Mount Everest (8828m, barometric pressure 33.3kPa) without supplemental oxygen that ‘I am nothing more than a single narrow, gasping lung, floating over the mists and summits’. Thus, we come back to the lung as the primary and essential organ for human function and survival at high altitude without which the first step up could not be taken. 9
 without supplemental oxygen that ‘I am nothing more than a single narrow, gasping lung, floating over the mists and summits’. Thus, we come back to the lung as the primary and essential organ for human function and survival at high altitude without which the first step up could not be taken. 9.")
10
External Respiration 10

11
Atmospheric composition at sea level
GAS PERCENT NITROGEN OXYGEN ARGON CARBON DIOXIDE HYDROGEN NEON HELIUM 11

12
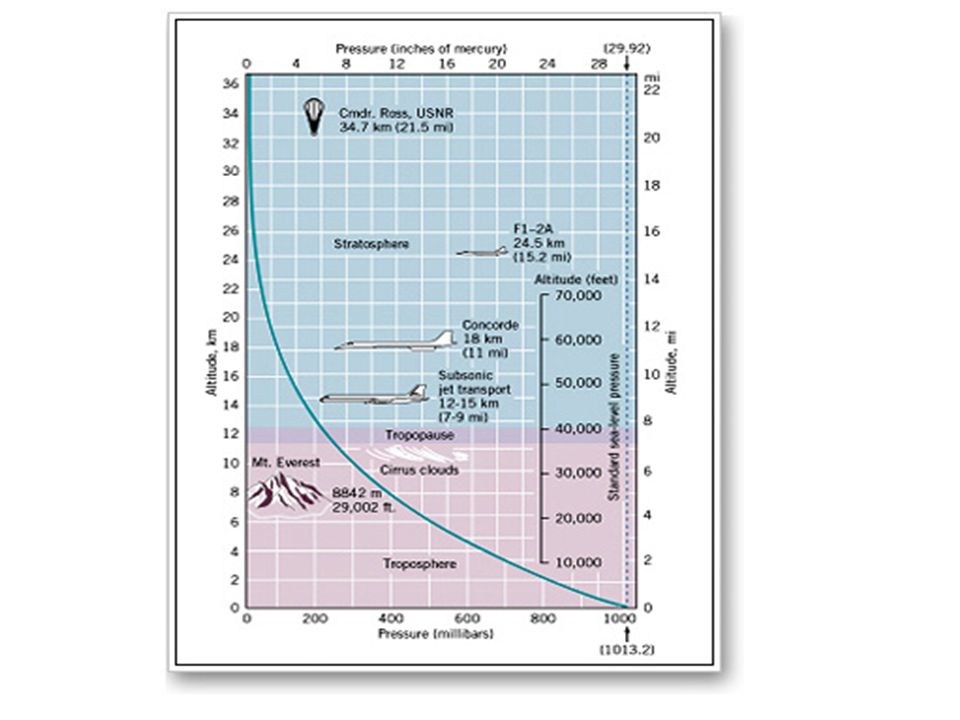
Atmospheric Pressure declines with altitude
Sea level: 1 atm = 14.7 lbs/inch2 (psi) 18,000 ft (5,486 m): 0.5 atm = 7.35 psi 12
 18,000 ft (5,486 m): 0.5 atm = 7.35 psi. 12.")
13
Atmosphere Hydrosphere Reduction in Pressure And O2
m Mount Everest Pressure reduced to 1/2 atm Reduction in Pressure And O2 m Human Settlement, Tibet 0.1 atm reduction every 1km 2954 m Mt. Apo Sea Level = 1 atm Hydrosphere 13 atm -130 m Increase in Pressure And Gas Solubility 370 atm -3700 m average depth of oceans 1 atm increase every ~10 m 1086 atm m Mariana Trench 13

14
Baguio City Mt. Apo Pressure differences are enormous, leading to differences in oxygen supply for air-breathers

15
Adaptations to high altitude
High altitude mammals: More pigment in blood High affinity hemoglobin Birds: (1) Cross-current flow of air and blood allowing higher O2 concentration in blood than in exhaled air (2) Tolerate low CO2 in blood (Alkalosis) (3) Normal blood flow to the brain at low blood PCO2 (4) Total respiratory volume is 3X that of mammals 15
 Cross-current flow of air and blood allowing higher. O2 concentration in blood than in exhaled air. (2) Tolerate low CO2 in blood (Alkalosis) (3) Normal blood flow to the brain at low blood PCO2. (4) Total respiratory volume is 3X that of mammals. 15.")
16
Evolution of hemoglobin function
Highland Camelids (llama, vicuña, alpaca) display lower P50 (higher affinity) than lowland Asian/African camels Amino acid substitutions in - globin chains which reduce the effect of DPG binding A small number of substitutions are sufficient to adapt the functional properties of hemoglobin to severely hypoxic conditions
 display lower P50 (higher affinity) than lowland Asian/African camels. Amino acid substitutions in - globin chains which reduce the effect of DPG binding. A small number of substitutions are sufficient to adapt the functional properties of hemoglobin to severely hypoxic conditions.")
17
Adaptation vs Acclimation/Acclimatization
1) Short Term Acclimation Mountain climbers who are able to maintain normal blood pH at low oxygen 2) Developmental Acclimation A person reared at high altitude: larger lung volume Higher concentration of red blood cells 3) Adaptation Llamas: Blood with high Oxygen affinities
 Short Term Acclimation. Mountain climbers who are able to maintain normal blood pH at low oxygen. 2) Developmental Acclimation. A person reared at high altitude: larger lung volume. Higher concentration of red blood cells. 3) Adaptation. Llamas: Blood with high Oxygen affinities.")
18
High Altitude: Humans Developmental Acclimation (Mountain People)
Larger lung volumes 40% higher ventilation rate in populations at 4500m (≠ maladapted hyperventilation) Increase number of blood cells (5 million/mm3 --> 8 million/mm3 at 4000m) Increase myoglobin concentration in muscles Effect on Enzymatic pathways not understood Increase in number of muscle capillaries and mitochondria Whether Adaptive differences occur in Humans is not known 18
 Increase number of blood cells. (5 million/mm3 --> 8 million/mm3 at 4000m) Increase myoglobin concentration in muscles. Effect on Enzymatic pathways not understood. Increase in number of muscle capillaries and mitochondria. Whether Adaptive differences occur in Humans is not known. 18.")
19
High Altitude: Humans Highest permanent settlement: 5000m mining camp in Andes RESPONSE TO LOW O2: Hyperventilation leading to low PCO2 Chronic Hypoxia 19

20
High Altitude: Humans Acclimation (or Acclimatization)
Change in response of respiratory center (in hypothalamus) Adjust bicarbonate concentration in blood to maintain normal blood pH at low PO2 (and low PCO2 that arises from hyperventilation) 20
 Adjust bicarbonate concentration in blood to maintain normal blood pH at low PO2 (and low PCO2 that arises from hyperventilation) 20.")
21
ACCLIMATIZATION Process by which people gradually adjust to high altitude Determines survival and performance at high altitude Series of physiological changes O2 delivery hypoxic tolerance +++ Acclimatization depends on severity of the high-altitude hypoxic stress rate of onset of the hypoxia individual’s physiological response to hypoxia 21

22
High Altitude: Humans (1) In response to low O2, ventilation increases
Hyperventilation (negative feedback) (1) In response to low O2, ventilation increases (2) But then this reduces PCO2 (3) pH increases, reducing normal stimulation in the respiratory center (4) Reduces ventilation (5) Decrease oxygen supply (6) More increased ventilation to gain O2 Hypoxia: Brain damage after 4-6 minutes of oxygen deprivation 22
 (1) In response to low O2, ventilation increases. (2) But then this reduces PCO2. (3) pH increases, reducing normal stimulation in the respiratory center. (4) Reduces ventilation. (5) Decrease oxygen supply. (6) More increased ventilation to gain O2. Hypoxia: Brain damage after 4-6 minutes of oxygen deprivation. 22.")
23
Heart and Pulmonary Circulation at High Altitude
Penaloza, D and vier Arias-Stella J. Circulation. 2007;115: )
")
24
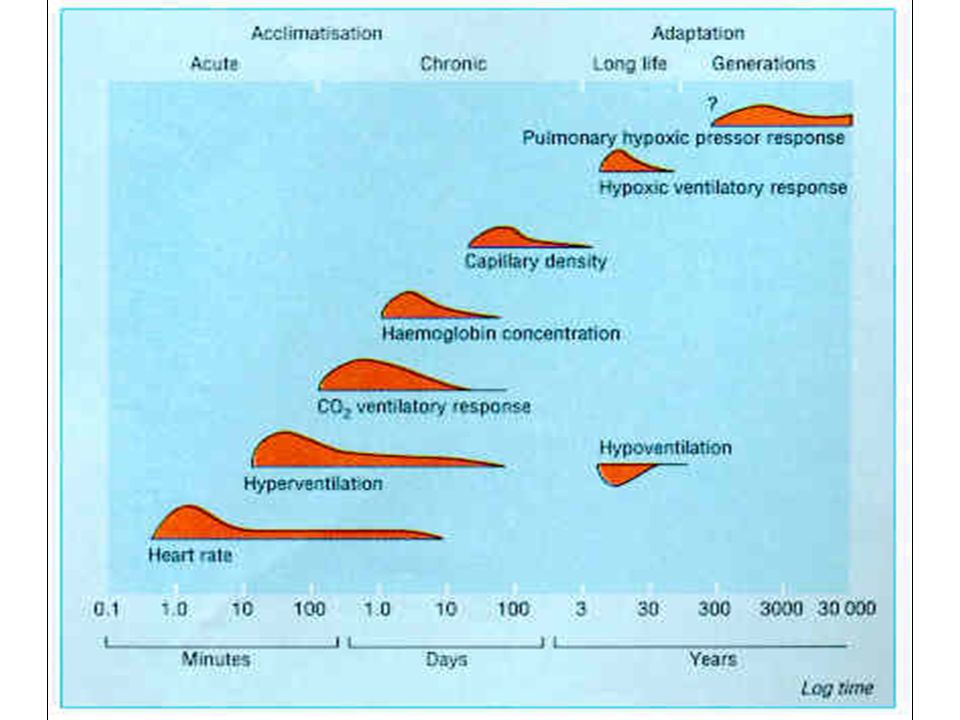
VENTILATORY ACCLIMATIZATION
Hypoxic ventilatory response = VE Starts within the 1st few hours of exposure 1500m Mechanism Ascent to altitude Hypoxia Decreased PCO2 Carotid body stimulation On arrival at altitude, increased carotid body activity attempts to increase ventilation, and thereby to raise the arterial oxygen pressure back to the sea level value. However, this presents the body with a dilemma. An increase in breathing causes an increased excretion of carbon dioxide in the exhaled air. When CO2 is in body tissues, it creates an acid aqueous solution, and when it is lost in exhaled air, the body fluids, including blood, become more alkaline, thus altering the acid-base balance in the body. The dilemma is that ventilation is regulated not only to keep oxygen pressure constant, but also for acid- base balance. CO2 regulates breathing in the opposite direction from oxygen. Thus when the CO2 pressure (i.e., the degree of acidity somewhere within the respiratory centre) rises, ventilation rises, and when it falls, ventilation falls. On arrival at high altitude, any increase in ventilation caused by the low oxygen environment will lead to a fall in CO2 pressure, which causes alkalosis and acts to oppose the increased ventilation. Therefore, the dilemma on arrival is that the body cannot maintain constancy in both oxygen pressure and acid-base balance. Human beings require many hours and even days to regain proper balance. Respiratory centres stimulation Increased ventilation CO2 + H2O H2CO3 HCO3- + H+ Improved hypoxia 24
 rises, ventilation rises, and when it falls, ventilation falls. On arrival at high altitude, any increase in ventilation caused by the low oxygen environment will lead to a fall in CO2 pressure, which causes alkalosis and acts to oppose the increased ventilation. Therefore, the dilemma on arrival is that the body cannot maintain constancy in both oxygen pressure and acid-base balance. Human beings require many hours and even days to regain proper balance. Respiratory centres stimulation. Increased ventilation. CO2 + H2O H2CO3 HCO3- + H+ Improved hypoxia. 24.")
25
ADJUSMENT OF RESPIRATORY ALKALOSIS
alkaline bicarbonate excretion in the urine but slow process ! Progressive increase in the sensitivity of the carotid bodies After several hr to days at altitude (interval of ventilatory acclimatization): cerebrospinal fluid pH adjustment to the respiratory alkalosis new steady state One method for rebalancing is for the kidneys to increase alkaline bicarbonate excretion in the urine, which compensates for the respiratory loss of acidity, thus helping to restore the body's acid-base balance toward the sea-level values. The renal excretion of bicarbonate is a relatively slow process. For example, on going from sea level to 4,300 m (14,110 ft), acclimatization requires from seven to ten days (figure 37.3). This action of the kidneys, which reduces the alkaline inhibition of ventilation, was once thought to be the major reason for the slow increase in ventilation following ascent, but more recent research assigns a dominant role to a progressive increase in the sensitivity of the hypoxic sensing ability of the carotid bodies during the early hours to days following ascent to altitude. This is the interval of ventilatory acclimatization. The acclimatization process allows, in effect, ventilation to rise in response to low arterial oxygen pressure even though the CO2 pressure is falling. As the ventilation rises and pressure falls with acclimatization at altitude, there is a resultant and concomitant rise in oxygen pressure within the lung alveoli and the arterial blood. 25
: cerebrospinal fluid pH adjustment to the respiratory alkalosis. new steady state. One method for rebalancing is for the kidneys to increase alkaline bicarbonate excretion in the urine, which compensates for the respiratory loss of acidity, thus helping to restore the body s acid-base balance toward the sea-level values. The renal excretion of bicarbonate is a relatively slow process. For example, on going from sea level to 4,300 m (14,110 ft), acclimatization requires from seven to ten days (figure 37.3). This action of the kidneys, which reduces the alkaline inhibition of ventilation, was once thought to be the major reason for the slow increase in ventilation following ascent, but more recent research assigns a dominant role to a progressive increase in the sensitivity of the hypoxic sensing ability of the carotid bodies during the early hours to days following ascent to altitude. This is the interval of ventilatory acclimatization. The acclimatization process allows, in effect, ventilation to rise in response to low arterial oxygen pressure even though the CO2 pressure is falling. As the ventilation rises and pressure falls with acclimatization at altitude, there is a resultant and concomitant rise in oxygen pressure within the lung alveoli and the arterial blood. 25.")
26
VENTILATORY RESPONSE TO EXERCISE
Varies with hypoxia ventilatory response (HVR) at rest at sea level Larger ventilatory response climbing performance but, at extreme altitude, larger work of breathing altitude trade-off Although the actual increase in the sensitivity of the carotid body to hypoxemia during the course of acclimation is not fully understood, it appears that each individual’s HVR, as measured at sea level, is roughly proportional to the ventilatory response to exercise at high altitude (Schoene et al., 1984; Schoene et al., 1990). In other words, subjects with a low HVR at rest measured at sea level have a relatively more blunted ventilatory response to exercise at high altitude than those with a high HVR, and vice versa. A large ventilatory response to exercise conveys a greater respiratory alkalosis and higher arterial oxygen saturation and may confer a better climbing performance at very high altitudes (Schoene et al., 1984) (Fig.2). However, individuals with very large HVRs may incur a greater work of breathing at extreme altitude. Thus, there may be a trade-off between increased arterial blood oxygenation and the increased work of breathing in these individuals. Schoene et al., 1984 26
 at rest at sea level. Larger ventilatory response climbing performance. but, at extreme altitude, larger work of breathing altitude trade-off. Although the actual increase in the sensitivity of the carotid body to hypoxemia during the course of acclimation is not fully understood, it appears that each individual’s HVR, as measured at sea level, is roughly proportional to the ventilatory response to exercise at high altitude (Schoene et al., 1984; Schoene et al., 1990). In other words, subjects with a low HVR at rest measured at sea level have a relatively more blunted ventilatory response to exercise at high altitude than those with a high HVR, and vice versa. A large ventilatory response to exercise conveys a greater respiratory alkalosis and higher arterial oxygen saturation and may confer a better climbing performance at very high altitudes (Schoene et al., 1984) (Fig.2). However, individuals with very large HVRs may incur a greater work of breathing at extreme altitude. Thus, there may be a trade-off between increased arterial blood oxygenation and the increased work of breathing in these individuals. Schoene et al.,")
27
LUNG DIFFUSION Definition High altitude O2 diffusion, because of
Process by which O2 moves from the alveolar gas into the pulmonary capillary blood, and CO2 moves in the reverse direction High altitude O2 diffusion, because of a lower driving pressure for O2 from the air to the blood a lower affinity of Hb for O2 on the steep portion of the O2/Hb curve and inadequate time for equilibration High altitude imposes a diffusion limitation of oxygen from the air to the blood (Fig.6). This diffusion limitation is secondary to several factors: (i) a lower driving pressure for oxygen from the air to the blood, (ii) a lower affinity of hemoglobin for oxygen on the steep portion of the oxygen/hemoglobin curve, and (iii) a decreased and inadequate time for equilibration of oxygen as the red blood cell traverses the pulmonary capillary. As mentioned above, the decreased alveolar partial pressure of oxygen at high altitude is in part minimized by ongoing ventilatory acclimation. This response to acclimation, however, is never adequate to overcome the ambient hypobaria. But, because of the large volume of gas that is required to supply an adequate quantity of oxygen, especially during the high metabolic demands of exercise, the lung is well designed to minimize the diffusion limitation in that the alveolar–capillary interface provides a large surface area for gas exchange that is instantly adaptable (West and Mathieu-Costello, 1992). Oxygen flux depends on the demand for oxygen, and the greater the ratio of diffusion capacity to perfusion the more successful is the loading of oxygen to the blood. 27
. This diffusion limitation is secondary to several factors: (i) a lower driving pressure for oxygen from the air to the blood, (ii) a lower affinity of hemoglobin for oxygen on the steep portion of the oxygen/hemoglobin curve, and (iii) a decreased and inadequate time for equilibration of oxygen as the red blood cell traverses the pulmonary capillary. As mentioned above, the decreased alveolar partial pressure of oxygen at high altitude is in part minimized by ongoing ventilatory acclimation. This response to acclimation, however, is never adequate to overcome the ambient hypobaria. But, because of the large volume of gas that is required to supply an adequate quantity of oxygen, especially during the high metabolic demands of exercise, the lung is well designed to minimize the diffusion limitation in that the alveolar–capillary interface provides a large surface area for gas exchange that is instantly adaptable (West and Mathieu-Costello, 1992). Oxygen flux depends on the demand for oxygen, and the greater the ratio of diffusion capacity to perfusion the more successful is the loading of oxygen to the blood. 27.")
28
CONSEQUENCE O2 DIFFUSION
arterial O2 saturation Arterial oxygen saturation thus decreases with exercise at high altitude, as has been documented in a number of human studies in both field and laboratory settings (Gale et al., 1985; Torre-Bueno et al., 1985; Wagner et al., 1986; Wagner et al., 1987; West et al., 1983) (Fig.7). Using sophisticated evaluations of gas exchange (the multiple inert gas elimination technique, MIGET), investigators have been able to apportion the decline in arterial oxygen saturation by looking at ventilation/perfusion relationships as well as diffusion characteristics (Fig.8). During acute hypobaric hypoxia to simulate an altitude of 4700m, Gale et al. (Gale et al., 1985), Torre-Bueno et al. (Torre-Bueno et al., 1985) and Wagner et al. (Wagner et al., 1986) showed both a ventilation/perfusion inequality and a diffusion limitation in the lung, both of which accounted for worsening hypoxemia with increasing work loads at higher altitudes. In Operation Everest II, the assimilated ascent to 8828m (PO2, approximately 33.3kPa) demonstrated that the ventilation/perfusion heterogeneity persisted to a modest degree while the diffusion limitation of oxygen became greater with increasing altitude (Wagner et al., 1987) (Fig.8). The increase in diffusion limitation was thought to be secondary to the marked decrease in driving pressure for oxygen from the air to the blood at these extreme simulated altitudes. West et al., 1983 Wagner et al, Mt. Everest II project,1995 28
 (Fig.7). Using sophisticated evaluations of gas exchange (the multiple inert gas elimination technique, MIGET), investigators have been able to apportion the decline in arterial oxygen saturation by looking at ventilation/perfusion relationships as well as diffusion characteristics (Fig.8). During acute hypobaric hypoxia to simulate an altitude of 4700m, Gale et al. (Gale et al., 1985), Torre-Bueno et al. (Torre-Bueno et al., 1985) and Wagner et al. (Wagner et al., 1986) showed both a ventilation/perfusion inequality and a diffusion limitation in the lung, both of which accounted for worsening hypoxemia with increasing work loads at higher altitudes. In Operation Everest II, the assimilated ascent to 8828m (PO2, approximately 33.3kPa) demonstrated that the ventilation/perfusion heterogeneity persisted to a modest degree while the diffusion limitation of oxygen became greater with increasing altitude (Wagner et al., 1987) (Fig.8). The increase in diffusion limitation was thought to be secondary to the marked decrease in driving pressure for oxygen from the air to the blood at these extreme simulated altitudes. West et al., Wagner et al, Mt. Everest II project,")
29
VA/Q HETEROGENEITY Varies from zero to infinity
Zero : perfusion but no ventilation O2 and CO2 tensions in arterial blood, equal those of mixed venous blood because there is no gas exchange in the capillaries Infinity: ventilation but no perfusion no modification of inspired air takes place due to over- ventilation or under-perfusion 29

30
VA/Q HETEROGENEITY O2 At rest At high altitude interstitial edema
The ventilation/perfusion heterogeneity was attributed to interstitial edema from high intervascular pressures, which correlated with the increase in pulmonary artery pressures. Much controversy exists regarding the effect on gas exchange of increased intervascular pressures during exercise at high altitude. During acute hypoxia, extravasation of fluid from the intra- to the extravascular space has been documented both at high altitude and at sea level in human and equine experiments (Hopkins et al., 1997; Pascoe et al., 1981; Seaman et al., 1995; Whitwell and Greet, 1984). O2 - Inhaled air is not evenly distributed to alveoli - Composition of gases is not uniform throughout lungs - Different areas of the lungs have different perfusion - Differences are less in recumbent position 30
. O2. - Inhaled air is not evenly distributed to alveoli. - Composition of gases is not uniform throughout lungs. - Different areas of the lungs have different perfusion. - Differences are less in recumbent position. 30.")
31
Penaloza, D and vier Arias-Stella J. Circulation. 2007;115:1132-1146.)
")
32
MIGET evaluation of Ventilation-perfusion relationships during induced polycythemia (with no pulmonary hypertension) Hct Range Hct Midpoint Log SD Perfusion Mean Perfusion Log SD Ventilation Mean Ventilation 30-39 35 0.56 1.66 40-49 45 1.05 2.20 50-59 55 1,22 2.87 60-69 65 1.97 3.44 70-79 75 2.72 3.96 Balgos A, Willford D, West JB. J Appl Physiol, 65(4): , 1988
: ,")
34
Maximal oxygen consumption at high altitude
85% of sea level values, at 3000m; 60% at 5000m, and only 20% at 8000m Ascribed to reduction in mitochondrial PO2 Could also be due to central inhibition from brain Most likely not due to pulmonary hypertension Elite mountaineers tend to have an insertion variant of angiotensin-converting enzyme gene West, JB. Annals Intern Med, 2004, 141:

35
Effects on Mental performance
Most people working at >4000m experience increased arithmetic error, reduced attention span, and increased mental fatigue Visual sensitivity (night vision) decreased at 2000m, and up to 50% at 5000m Molecular and cellular mechanisms of these effects of hypoxia are poorly understood Suggested mechanisms: altered ion homeostasis, changes in calcium metabolism, alterations in neurotransmitter metab., and impaired synapse function West, JB. Annals Intern Med, 2004, 141:
 decreased at 2000m, and up to 50% at 5000m. Molecular and cellular mechanisms of these effects of hypoxia are poorly understood. Suggested mechanisms: altered ion homeostasis, changes in calcium metabolism, alterations in neurotransmitter metab., and impaired synapse function. West, JB. Annals Intern Med, 2004, 141:")
36
Effects on Sleep Sleep impairment common and most distressing: frequent awakenings, unpleasant dreams, do not feel refreshed on waking up in the morning Periodic breathing,which occurs at >4000m is most likely an important causative factor Possible reasons for periodic breathing: instability of of control system for hypoxic drive, or response to CO2, as well as low levels of PaO2 after apneic episodes West, JB. Annals Intern Med, 2004, 141:

37
WHEN ACCLIMATIZATION FAILS
Altitude syndromes Acute mountain sickness (AMS): the least-threatening and most common High altitude pulmonary edema High altitude cerebral edema All these syndromes have several features in common respond to descent or oxygen potentially lethal form of AMS 37
: the least-threatening and most common. High altitude pulmonary edema. High altitude cerebral edema. All these syndromes have. several features in common. respond to descent or oxygen. potentially lethal form of AMS. 37.")
38
ACUTE MOUNTAIN SICKNESS
Major symptoms Headache Fatigue Dizziness Anorexia Dyspnea (but tricky!) Incidence and severity depend on Rate of ascent Altitude attained Length of time at altitude Degree of physical exertion Individual’s physiological susceptibility Treatment hardly needed Only a problem if progression of symptoms to those of HAPE HACE 38
 Incidence and severity depend on. Rate of ascent. Altitude attained. Length of time at altitude. Degree of physical exertion. Individual’s physiological susceptibility. Treatment hardly needed. Only a problem if progression of symptoms to those of. HAPE. HACE. 38.")
39
HIGH ALTITUDE PULMONARY EDEMA (HAPE)
Noticed only after 24-48hr and occurs after the 2nd night Occurs in otherwise healthy people without known cardiac or pulmonary disease 1:50 climbers on McKinley succumb to HAPE (Hackett et al., 1990) Occurs when people go rapidly to high altitude Extravasation of fluid from the intra- to extravascular space in the lung 39
 Occurs when people go rapidly to high altitude. Extravasation of fluid from the intra- to extravascular space in the lung. 39.")
40
WHY DOES HAPE OCCUR ? Hypothesis 1. Pulmonary hypertension
Strong relationship between the development of HAPE in people with Mild pulmonary hypertension at rest Accentuated pulmonary vascular response to hypoxia or exercise But pulmonary hypertension alone is not enough to result in HAPE (Sartori et al., 2002) There is strong evidence that HAPE is due to patchy capillary damage due to pulmonary hypertension (West JB, 2004) 40
 There is strong evidence that HAPE is due to patchy capillary damage due to pulmonary hypertension. (West JB, 2004) 40.")
41
WHY DOES HAPE OCCUR ? Hypothesis 2. Pulmonary endothelium barrier fragility Pulmonary endothelium barrier susceptible to Mechanical stress Stretching of the endothelium gaps passage of proteins and red blood cells Inflammation Mediators release permeability gaps passage of proteins, red blood cells and inflammatory mediators Questions: inflammation = 1st culprit High pressure alone enough to result in extra vascular leak ? 41

42
INFLAMMATION IN HAPE ? Schoene et al., 1986, 1998
[Leukotrienes] (marker of inflammation) very high in BAL in subjects acutely ill with HAPE But is inflammation present at the start or as a result of HAPE ? Swenson et al., 2002 RBC and proteins present in BAL in people at onset of HAPE But no inflammatory markers present Inflammation probably not the causative factor Swenson et al., 2002 42
 very high in BAL in subjects acutely ill with HAPE. But is inflammation present at the start or as a result of HAPE Swenson et al., RBC and proteins present in BAL in people at onset of HAPE. But no inflammatory markers present. Inflammation probably not the causative factor. Swenson et al.,")
43
HYPOXIC PULMONARY VASOCONSTRICTION
The stress failure theory (West et Mathieu-Costello, 1998, 99) Alveolar hypoxia Hypoxic pulmonary vasoconstriction (uneven) capillary pressure (some capillaries) VA/Q heterogeneity Damage to capillary wall (stress failure) Exposed basement membrane EDEMA Inflammatory mediators West, JB. Annals Intern Med, 2004, 141: 43
 Alveolar hypoxia. Hypoxic pulmonary vasoconstriction (uneven) capillary pressure (some capillaries) VA/Q heterogeneity. Damage to capillary wall (stress failure) Exposed basement membrane. EDEMA. Inflammatory mediators. West, JB. Annals Intern Med, 2004, 141:")
44
EXERCISE-INDUCED HYPOXEMIA
MORE HYPOXEMIA O2 Alveolar hypoxia Hypoxic pulmonary vasoconstriction (uneven) capillary pressure (some capillaries) VA/Q heterogeneity Damage to capillary wall (stress failure) Exposed basement membrane EDEMA Inflammatory mediators results in about ½ endurance athletes (Powers et al., 1988) 44
 capillary pressure (some capillaries) VA/Q heterogeneity. Damage to capillary wall (stress failure) Exposed basement membrane. EDEMA. Inflammatory mediators. results in about ½ endurance athletes (Powers et al., 1988) 44.")
45
INTEGRITY OF PULMONARY BLOOD-GAS BARRIER IN ATHLETES
Hopkins et al., 1997 BAL in 6 athletes after a 7min exercise at maximal intensity Post exercise: RBC Total protein Albumin Leukotrienes B4 Hopkins et al., 1998 1h at 70% VO2max no signs of alteration Impairment of the integrity of blood-gas barrier only at extreme level of exercise in elite athletes > control subjects at rest We tested the hypothesis that, in elite human athletes, the high capillary pressure that occurs during severe exercise alters the structure and function of the blood-gas barrier. We performed bronchoalveolar lavage (BAL) in six healthy athletes, who had a history suggestive of lung bleeding, 1 h after a 7-min cycling race simulation and four normal sedentary control subjects who did not exercise before BAL. The athletes had higher (p < 0.05) concentrations of red blood cells (0.51 x 10(5) versus 0.01 x 10(5).ml-1), total protein (128.0 versus micrograms/ml), albumin (65.6 versus 53.0 micrograms/ml), and leukotriene B4 (LTB4) (243 versus 0 pg/ml) in BAL fluid than control subjects. The proportion of neutrophils was similar in athletes and control subjects but the proportion of lymphocytes in BAL fluid was reduced (p < 0.05). There were no differences in levels of surfactant apoprotein A, tumor necrosis factor bioactivity, lipopolysaccharide, or interleukin-8 (IL-8) between groups. These results show that brief intense exercise in athletes with a history suggestive of lung bleeding alters blood-gas barrier function resulting in higher concentrations of red cells and protein in BAL fluid. The lack of activation of proinflammatory pathways (except LTB4) in the airspaces supports the hypothesis that the mechanism for altered blood- gas barrier function is mechanical stress. 45
 in six healthy athletes, who had a history suggestive of lung bleeding, 1 h after a 7-min cycling race simulation and four normal sedentary control subjects who did not exercise before BAL. The athletes had higher (p < 0.05) concentrations of red blood cells (0.51 x 10(5) versus 0.01 x 10(5).ml-1), total protein (128.0 versus 94.1 micrograms/ml), albumin (65.6 versus 53.0 micrograms/ml), and leukotriene B4 (LTB4) (243 versus 0 pg/ml) in BAL fluid than control subjects. The proportion of neutrophils was similar in athletes and control subjects but the proportion of lymphocytes in BAL fluid was reduced (p < 0.05). There were no differences in levels of surfactant apoprotein A, tumor necrosis factor bioactivity, lipopolysaccharide, or interleukin-8 (IL-8) between groups. These results show that brief intense exercise in athletes with a history suggestive of lung bleeding alters blood-gas barrier function resulting in higher concentrations of red cells and protein in BAL fluid. The lack of activation of proinflammatory pathways (except LTB4) in the airspaces supports the hypothesis that the mechanism for altered blood- gas barrier function is mechanical stress. 45.")
46
Circular break of the epithelium
Full break of the blood-gas barrier Costello et al., 1992 Red cell moving out of the capillary lumen (c) into an alveolus (a) West et al., 1995 46
 into an alveolus (a) West et al.,")
47
WHY DOES HAPE OCCUR ? Hypothesis 3. Perturbation of alveolar fluid clearance Role of fluid in extravascular space depends on: Its accumulation Efficiency of its rate of clearance Hypoxia Na,K-ATPase activity (Dada et al., 2003) Twenty years ago, pioneering studies by Matthay et al. (3) revealed that alveolar fluid resorption in adult animals was not affected by manipulating Starling forces but via active transport of sodium (Na+) from the alveolar airspaces, across the alveolar epithelium, and into the pulmonary circulation. This creates an osmotic gradient that is responsible for the clearance of lung edema from the alveolar spaces (4–6). As depicted in Figure 1, Na+ uptake occurs on the apical surface of alveolar epithelial cells (AECs), predominantly through amiloride- sensitive Na+ channels (6, 7). (Amiloride is a specific Na+ channel inhibitor.) Subsequently, Na+ is actively extruded from the basolateral surface into the lung interstitium by the sodium potassium-adenosine triphosphatase (Na,K-ATPase); water follows because of the osmotic gradient (2, 8, 9). Experiments in human lungs, in situ animal models, and isolated rat lungs have demonstrated that lung liquid clearance is prevented by hypothermia—probably by inhibition of active metabolic processes for solute transport (10)—and inhibited by both amiloride and ouabain, a Na,K-ATPase inhibitor (8, 11, 12). The Na,K-ATPase is a plasma membrane enzyme that maintains electrochemical Na+ and K+ gradients across the plasma membrane by pumping Na+ out of the cell and K+ into the cell against their respective concentration gradients in an adenosine 5'-triphosphate-dependent process. 47
 Twenty years ago, pioneering studies by Matthay et al. (3) revealed that alveolar fluid resorption in adult animals was not affected by manipulating Starling forces but via active transport of sodium (Na+) from the alveolar airspaces, across the alveolar epithelium, and into the pulmonary circulation. This creates an osmotic gradient that is responsible for the clearance of lung edema from the alveolar spaces (4–6). As depicted in Figure 1, Na+ uptake occurs on the apical surface of alveolar epithelial cells (AECs), predominantly through amiloride- sensitive Na+ channels (6, 7). (Amiloride is a specific Na+ channel inhibitor.) Subsequently, Na+ is actively extruded from the basolateral surface into the lung interstitium by the sodium potassium-adenosine triphosphatase (Na,K-ATPase); water follows because of the osmotic gradient (2, 8, 9). Experiments in human lungs, in situ animal models, and isolated rat lungs have demonstrated that lung liquid clearance is prevented by hypothermia—probably by inhibition of active metabolic processes for solute transport (10)—and inhibited by both amiloride and ouabain, a Na,K-ATPase inhibitor (8, 11, 12). The Na,K-ATPase is a plasma membrane enzyme that maintains electrochemical Na+ and K+ gradients across the plasma membrane by pumping Na+ out of the cell and K+ into the cell against their respective concentration gradients in an adenosine 5 -triphosphate-dependent process. 47.")
48
PREVENTION OF HAPE Don't climb at high altitude!!!!
Undergo hypoxic ventilation test to determine natural fitness for high altitude If not fit, undergo training, and plan for slow ascent (At altitudes above 3000 m individuals should climb no more than 300 m per day with a rest day every third day) Avoid strenuous physical exertion Anyone suffering symptoms of acute mountain sickness should stop, and if symptoms do not resolve within 24 hours descend at least 500 m.
 Avoid strenuous physical exertion. Anyone suffering symptoms of acute mountain sickness should stop, and if symptoms do not resolve within 24 hours descend at least 500 m.")
49
TREATMENT OF HAPE Get the patient down in lower altitude as fast and as low as possible Give O2 or hyperbaria Apply expiratory positive airways pressure With a respiratory valve device Or by pursed lips breathing Treat like any other case of pulmonary edema; in some cases, antibiotics may be needed 49

50
SPECIFIC TREATMENT OF HAPE
Acetazolamide, oral mg 2x/day Dexamethasone, oral. I.M. or I.V. 2 mg q 6hrs or 4 mg q 12 hrs. Nifedipine, oral mg long-acting, q 12 hrs. Tadalafil oral 50 mg. 2x/day Sildenafil 50 mg q 8 hrs Salmeterol inhaled 125mg 2x/day

51
Hepatic Insufficiency
Medication Renal Insufficiency Hepatic Insufficiency Pregnancy Other Issues Acetazolamide Avoid if GFR <10 mL/min, metab acidosis, hypoK, hypercalcemia, & hyperphosphatemia Contraindicated Category C Avoid if w/ concurrent long-term aspirin; cuation with sulfa allergy; avoid concurrent K-wasting diuretics and ophthalmjic CAI Dexamethasone No C.I.; No dose adjustments May increase FBS in diabetics; avoid in PUD or GO-bleed risk patients Nifedipine Best to avoid; if use necessary, 10 mg B.I.D. Caution PUD or GO-bleed risk or gastroesoph varices patients Tadalafil 5mg if GFR mL/min. Max 10 mg; <5 if GFR < 30mL/min. Child's Class A & B = 10mg/dL; Child's class C= don't use Category B Incr. Risk of GERD; caution with other meds affecting cP450; avoid concurrent nitrates and B-blockers Sildenafil Same dose adj as Tadalafil Decrease dose; start with 25 mg; avoid use if with g-e varices Salmeterol Insufficient data; best to avoid Potential for adverse reaction in pts w/ CAD prone to arrhythmia; avoid concurrent beta-blockers, monoamine oxidase inhibitors, or tricyclic antidepressants Luks and Swenson, Chest, 2008; 133:

52
Medication Malaria Traveler's Diarrhea
Acetazolamide No known interactions with prophylaxis med, but could increase serum quinine concentration No interactions with fluroquinolones or macrolides; Dexamethasone No known interactions with prophylaxis or treatment meds Potential increased risk of tendon injury Nifedipine No reported interactions with prophylaxis or treatment med, except mefloquine Avoid clarithromycin; safe to use azithromycin and fluroquinolones Tadalafil Sildenafil Salmeterol Avoid chloroquine due to increased risk of QT- interval prolongation and ventricular arrhythmia. Other agents safe to use Luks and Swenson, Chest, 2008; 133:

53
KEY POINTS High altitude = stressful environment for the lungs
At extreme altitudes : lung = primary and essential organ for human function and survival HAPE = potentially lethal form of AMS Extravasation of fluid from the intra- to extravascular space in the lung Main mechanism involved: pulmonary hypoxic vasoconstriction Capillary stress failure Exercise-induced hypoxemia at sea level shows a similar pattern 53

54
Summary Respiration is directly tied to metabolism, and physical and physiologic principles High Pressure and Altitude pose problems for Respiration, which reach the limits of normal physiology Different animals, including man, respond to high altitude through adaptation and/or acclimatization; Gene regulation of Hemoglobin evolves more quickly than structural changes Acute ascent to high altitude poses clinical problems that could lead to various forms of acute mountain sickness (AMS) which, like HAPE, may be fatal Prevention and early recognition of symptoms of HAPE important, for prompt treatment
 which, like HAPE, may be fatal. Prevention and early recognition of symptoms of HAPE important, for prompt treatment.")
55
Summary Best treatment is prevention
Specific treatment modalities helpful, but not always successful Best treatment is descent from high altitude. Other supportive treatment similar to any capillary leak pulmonary edema is often necessary

56
RECOMMENDED REFERENCES
BOOK Ward et al. High altitude medicine and physiology. 3rd edition. Arnold. 2000 ARTICLES Hopkins et al. Intense exercise impairs the integrity of the pulmonary blood-gas barrier in elite athletes. Am J Respir Crit Care Med. 1997;155(3): West JB et al. Pathogenesis of high-altitude pulmonary oedema: direct evidence of stress failure of pulmonary capillaries. Eur Respir J. 1995;8(4):523-9. Schoene. Unraveling the mechanism of high altitude pulmonary edema. High Alt Med Biol. 2004;5(2): West, JB. The Physiologic Basis of High Altitude Diseases. Annals Intern Med, 2004, 141: Luks and Swenson, Chest, 2008; 133: Martin, et al. Variattion in human performance in the hypoxi mountain environment. Exp Physiol, 2010; 953: 56
: West JB et al. Pathogenesis of high-altitude pulmonary oedema: direct evidence of stress failure of pulmonary capillaries. Eur Respir J. 1995;8(4): Schoene. Unraveling the mechanism of high altitude pulmonary edema. High Alt Med Biol. 2004;5(2): West, JB. The Physiologic Basis of High Altitude Diseases. Annals Intern Med, 2004, 141: Luks and Swenson, Chest, 2008; 133: Martin, et al. Variattion in human performance in the hypoxi mountain environment. Exp Physiol, 2010; 953:")
Similar presentations

>")











 –Dec max O2 consumption Extreme altitude 6000m(20000ft) –Progressive deterioration - death Fig.>")





