Download presentation
Presentation is loading. Please wait.

1
Tata Memorial Hospital
Childhood Acute Lymphoblastic Leukemia: Risk Stratification in Developing Countries Shripad Banavali MD(Med;Bom), BC(Ped;USA), BE(Hem-Onc;USA) Tata Memorial Hospital
, BC(Ped;USA), BE(Hem-Onc;USA) Tata Memorial Hospital.")
2
Acute Lymphoblastic Leukemia
Most common form of childhood cancer. Treatment of ALL is true success story of modern oncology.

4
Key Components of Successful Therapy
Clinical trials; Co-operative groups Empiric multi-agent CNS therapy Pre-symptomatic CNS therapy Post-induction intensification Anti-metabolite therapy Re-induction/re-consolidation Risk adapted therapy

5
ALL: L1, L2, L3, PAS

9
Multiplex RT-PCR in B lineage ALL

12
MORPHOLOGICAL REMISSION (98%)
Morphology cannot discriminate between patients with HR or LR of relapse. More sensitive techniques needed to detect small numbers of malignant cells during and after treatment. Detection of MRD (IP and RT-PCR). MOLECULAR REMISSION (?%)
. MOLECULAR REMISSION ( %)")
13
What is detection of MRD

14
What is detection of MRD
It is nothing but detection of the clones of cells resistant to the chemotherapy given.

15
MRD: Study of Resistance in ALL
Resistance can also be studied by:- (1) MTT in-vitro Assay Pred + Asp + VCR Drug resistance profile 3 yr DFS 100% Most sensitive profile (20% pts) 84% Inter. sensitive profile (40% pts) 43% Least sensitive profile (40% pts)
 MTT in-vitro Assay. Pred + Asp + VCR Drug resistance profile. 3 yr DFS 100% Most sensitive profile (20% pts) 84% Inter. sensitive profile (40% pts) 43% Least sensitive profile (40% pts)")
16
MRD: Study of Resistance in ALL
Resistance can also be studied in-vivo by:- (2) D7 blast count post exposure to Pred + 1 dose of IT-MTX (3) D 15 BM blast %
 D7 blast count post exposure to. Pred + 1 dose of IT-MTX. (3) D 15 BM blast %")
18
Estimation of MRD Flow cytometry : (2) RT-PCR:
 RT-PCR:")
22
Treatment of Childhood ALL
TOP PRIORITY PREVENTION OF RELAPSE

23
ALL-Challenges For Developed Countries Clinical trials
Despite success, 25% of children relapse. Intensify therapy for those who need or will benefit from it. Many of those who are cured are over-treated Minimize side effects Little progress has been made in the treatment of certain very high risk groups (Ph+, infants and relapse) Develop new treatment options
 Develop new treatment options.")
26
PEDIATRIC ONCOLOGY : FACTS
India U.S.A. New cases / yr , ,400 Rx, curative intent <25% % Cure rate, adequ. Rxed % % Overall cure rate % % Rxed on Co-op Groups % %

27
Hematological cancers in India Average Annual Age standardized incidence rate per 100,000 persons ( ) Region Lymphoid leukemia Myeloid leukemia M F M F Delhi Mumbai Bangalore Chennai Bhopal Barshi Medical Oncology, vol. 19, , 2002

28
Rx of ALL: THE TMH EXPERIENCE
V+P % V+P+Doxo or L-Asp % VACP % 1. Advani et al: Am J Hematol 15:35,1983 2. Advani et al: Ind J Cancer 26:180,1989 3. Advani et al: Am J Hematol 39:242, 1992 4. Advani et al: Ann Onc 10:167,1999

30
Advani et al. Ann Oncol 1999

31
Advani et al. Ann Oncol 1999

32
Clinical characteristics in relationship to event free survival by participating center. Results of multi-variate analysis. Characteristic DELHI P-Value CHENNAII MUMBAI Number accrued 228 168 652 Age 0.20 0.033 0.74 WBC count 0.0005 0.080 0.002 Platelet count 0.025 0.059 0.011 Hemoglobin 0.94 0.38 0.79 LDH -- 0.47 0.39 Immunophenotype 0.99 0.13 0.17 Lymphadenopathy 0.66 0.83 0.49 Hepatosplenomegaly 0.58 0.92 Mediastinal mass 0.32 0.10

33
CALLA + ACUTE LYMPHOBLASTIC LEUKEMIA CHANGING INCIDENCE OVER 3 DECADES

34
T- ACUTE LYMPHOBLASTIC LEUKEMIA CHANGING INCIDENCE OVER 3 DECADES

35
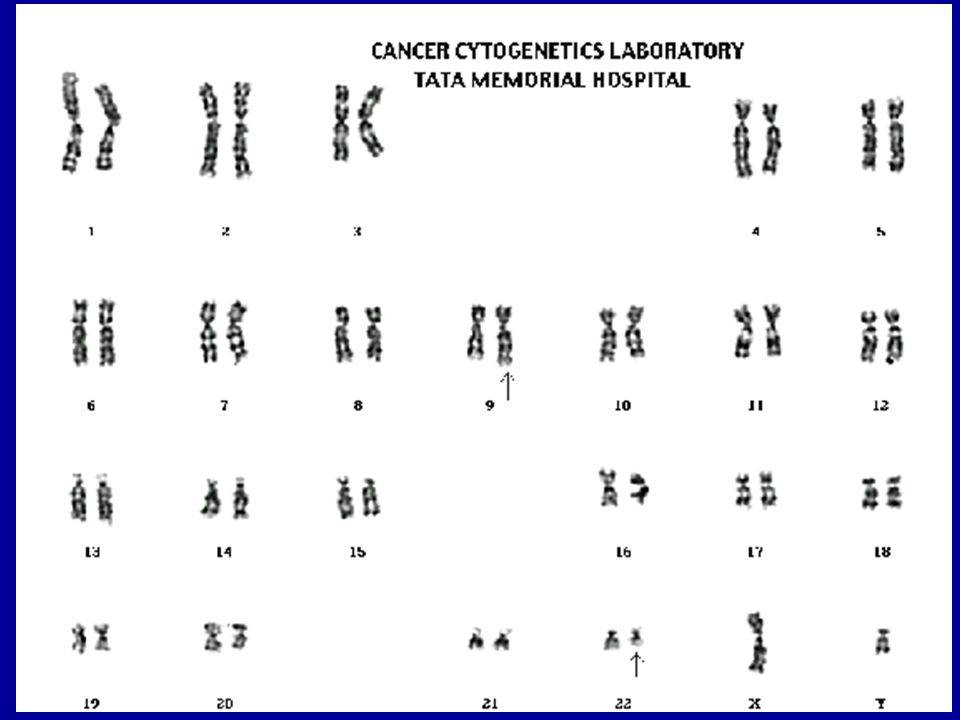
Frequencies of the major subgroups of Precursor B cell ALL in Indian children differ from the rest. Siraj AK, et al. Leukemia 2003; 17: n= 259 India (%) USA (%) Europe (%) TEL-AML mBCR-ABL* ELA-PBX MLL-AF *Guiterrez MI, et al. J Mol Diagnostics 2005; 7:40-47
 USA (%) Europe (%) TEL-AML mBCR-ABL* ELA-PBX MLL-AF *Guiterrez MI, et al. J Mol Diagnostics 2005; 7:")
36
x MUMBAI DELHI CHENNAI

37
Childhood Acute Lymphoblastic Leukemia Results of MCP-841 in other Centres
Bangalore Trivandrum Jaipur Total number 127 66 49 CR (%) 96 83 90 TRM(%) 2.4 24.2 16.3 Relapse(%) - 21.8 22.4 CCR(%) 53 57 F Up(months) 36 38
 TRM(%) Relapse(%) CCR(%) F Up(months)")
38
ALL : FUTURE PLANS CLINICAL
New ALL protocol Collaboration with INCTR Salient features More Continuous CT More Chemo in 1st year Both Inj. & oral CT during Maintenance Less RT (1260 cGy)
")
39
THE PROBLEM Limited Resources Lack of Appropriate
(Financial and Human Capital) Research High Low capacity to treat Poor Access to therapy Mortality Rate Late Presentation & Late Detection
 Research. High. Low capacity to treat Poor Access to therapy Mortality Rate. Late Presentation. & Late Detection.")
40
THE SOLUTION Limited Resources Appropriate
(Financial and Human Capital) Research Best Low capacity to treat Rx Pts. ĉ Best Prognosis Value for Money Low Intensity Rx
 Research. Best. Low capacity to treat Rx Pts. ĉ Best Prognosis Value for Money. Low Intensity Rx.")
41
Appropriate Rx ALL Rx Outcome Pharmacogenetics Pharmakokinetics
SEED Biology of Leukemic cells ALL Rx Outcome Pharmacogenetics Pharmakokinetics SOIL Genotype Nutrition Supportive care Compliance Drug quality

42
What is detection of MRD
It is nothing but detection of the clones of cells resistant to the chemotherapy given. “Functional Assay”

43
Appropriate Rx ALL Rx Outcome Pharmacogenetics Pharmakokinetics
SEED Biology of Leukemic cells ALL Rx Outcome Pharmacogenetics Pharmakokinetics SOIL Genotype Nutrition Supportive care Compliance Drug quality

44
Estimation of MRD Flow cytometry : 2-3 laser Flow-cytometer many antibodies time consuming expensive (2) RT-PCR: by TCR receptor; Ig gene rearrangements; known translocations. Individual primers. Expertise not available at all centres.
 RT-PCR: by TCR receptor; Ig gene rearrangements; known translocations. Individual primers. Expertise not available at all centres.")
46
Can there be a simple way to estimate MRD?

47
TDT expression by all ALL blasts Not expressed normally in PB
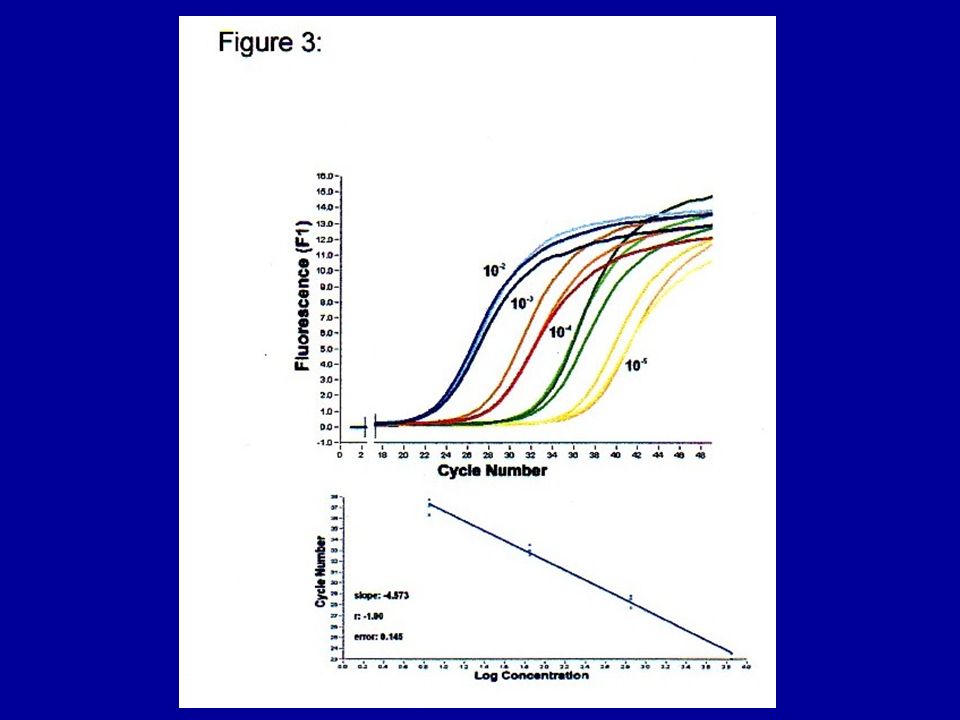
Real Time Analysis of Terminal Deoxy Transferase Gene Expression: A convenient marker for Minimal Residual Leukemia Bu R, Belgaumi A, Timson G, Banavali S, Al Mahir, Bhatia K, Gutierrez MI. TDT expression by all ALL blasts Not expressed normally in PB Estimation of TDT in PB by Real time PCR

50
ALL: “Core Biology” Lab Assessment Of Components Of Cure In Developing Countries
Real time reference laboratory system for risk based classification. MRD studies : using single parameter, e.g. TDT Using PB At diagnosis ; At week 4 & 6 (8)
")
51
ALL: “Core Biology” Lab Assessment Of Components Of Cure In Developing Countries
All samples to be sent to a central lab by courier. MRD studies based on single parameter, e.g. TDT. 5-7 day turnaround time. Results sent by . Remaining sample to be stored for future studies.

54
What Is The Best Way To Risk Stratify Children With ALL In Developing Countries?
One parameter (Not multiple like clinical, IP, DI, Cytogen, Mol, MRD) MRD Estimation Simplest version using single parameter Functional assay
 MRD Estimation. Simplest version using single parameter. Functional assay.")
55
Management of Childhood ALL
Common Standard Rem. Ind Protocol Estimation of MRD at D29/D43 > 1 % < 0.01 % < 0.1 % ? Less intensive Rx ? Shorter duration D. D. I Allo. BMT Investigational Therapies

56
CURABLE Childhood Cancers are PROVIDED THEY ARE…. diagnosed early
diagnosed properly treated appropriately

57
ALL TEAM Clinical Lab Studies INCTR Collaboration
Dr. S.D.Banavali Dr.C.N.Nair Dr. Ian Magrath Dr. P.A.Kurkure Dr. Ashok Kumar Ms. Melissa Adde Dr. B.Arora Mr. Sashikant Dr. Kishore Bhatia Dr. S.K.Pai Dr. A.Chougule Dr. Marina Gutierrez Dr. P.M.Parikh Dr. P.M. Parikh Dr. R.Bhagwat Dr.S. Barbhaya MSW Dept. Dr. A.Vora Dr.S.Kamath Mr.M.A. Patil Sister Asha Dr.P. Kadam Amre Ms. Neelima Dalvi Ms. A. Paes Dr. S.Chiplunkar Data Managers Radiotherapy Dr.J.Khode Ms. B.Kolhatkar Dr.M.A.Muckaden Ms.M.Patkar Ms.R.Hawaldar Dr.S.Lashkar Ms. B.Tambe Dr. N.Nair Mr.R.Kadam Surgery Dr. S.Goswami Dr. R.Mistry Dr.N.Merchant

Similar presentations





















 Department of Pediatrics Princess Marina Hospital.>")











