Download presentation
Presentation is loading. Please wait.

1
IV FLUIDS

2
Basic Principles

3
BASIC PRINCIPLES Osmolality/Osmolarity Tonicity Sodium & Water balance

4
What is Osmolality?

6
OSMOLALITY Measurement of concentration of particles in a solution
(Total concentration of penetrating & nonpenetrating solutes) i.e. Concentration of electrolytes, drugs, glucose in a solution such as serum or urine
 i.e. Concentration of electrolytes, drugs, glucose in a solution such as serum or urine.")
7
OSMOLALITY Normal = 285-295 mOsm/kg
The ICF and ECF are in osmotic equilibrium

8
OSMOLALITY OSMOLALITY = mOsm/kg of solvent
OSMOLARITY = mOsm/liter of a solution

9
What is Tonicity?

10
TONICITY measure of the ability of a solution to cause a change in the volume or tone of a cell by promoting osmotic flow of water (Total concentration of penetrating solutes only)
")
11
TONICITY

12
Who regulates osmolality?

13
Water

14
WATER BALANCE Important in the regulation of osmolality
Modification of water intake and exretion

15
60% ICF TOTAL BODY WATER ECF Interstitial Fluid Plasma

16
FORCES THAT MOVE WATER Osmolality Tonicity Na/K ATPase pump Hydrostatic pressure Oncotic pressure

17
SODIUM BALANCE The main regulator of intravascular volume status

18
Electrolyte composition
EXTRACELLULAR FLUID INTRACELLULAR FLUID

19
WHAT IS THE BODY’S GOAL? PHYSIOLOGIC HOMEOSTASIS EUVOLEMIA
ISOTONIC ENVIRONMENT

20
What mechanisms in the body makes sure that the balance of sodium and water is normal? What hormones play a big role in the maintenance of physiologic homeostasis?

21
There are upper & lower limits to the amount needed to achieve ideal physiologic homeostasis

22
WATER REPLACEMENT 1.5 to 2 liters / day

23
SODIUM REQUIREMENT DIET: RDA = < 2400mg/day (1 teaspoon/day)
or < 104 meq/day PLASMA : Normal levels = meq/L FOR Na CORRECTION: Maintenance of 2-4 meq/kg/day

24
Intravenous Fluids

25
INTRAVENOUS FLUIDS chemically prepared solutions
Achieve and maintain a euvolemic and isotonic environment within the body They are tailored to the body’s needs and used to replace lost fluid and/or aid in the delivery of IV medications

26
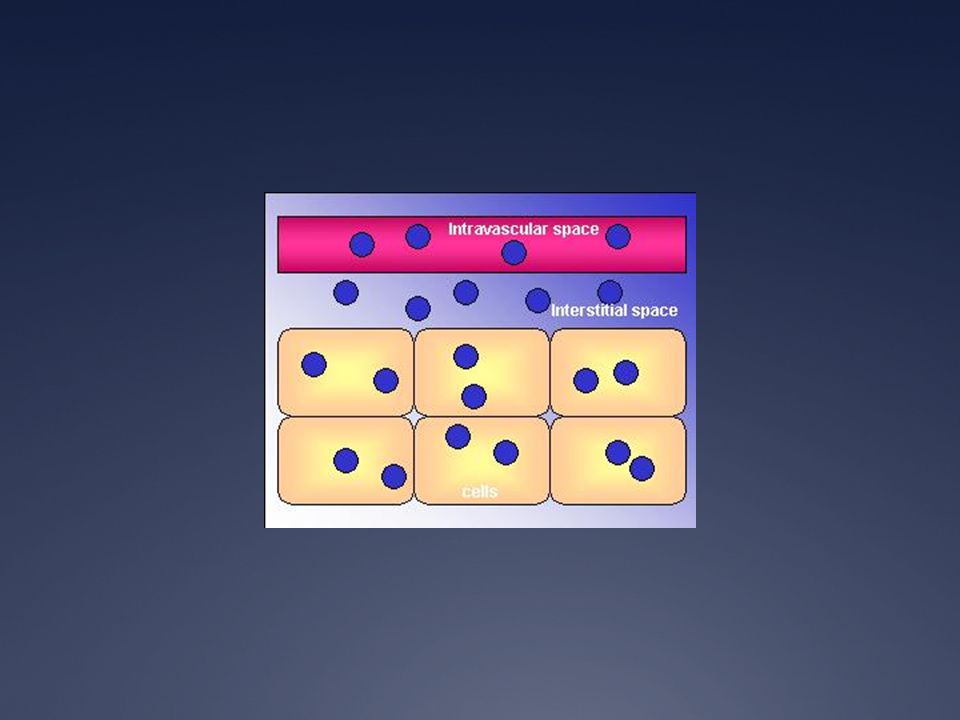
ISOTONIC IV FLUIDS created to distribute evenly between the intravascular, interstitial, and cellular spaces.

28
HYPOTONIC IV FLUIDS What IV fluids are specifically designed so the fluid leaves the intravascular space and enters the interstitial and intracellular spaces?

30
HYPERTONIC IV FLUIDS What IV fluids are designed to stay in the intravascular space (intra, within; vascular, blood vessels) to increase the intravascular volume, or volume of circulating blood?
 to increase the intravascular volume, or volume of circulating blood")
32
ISOTONIC SOLUTIONS = 285-295 mOsm/L
Na = meq/L HYPERTONIC SOLUTIONS = > 300 mOsm/L Na = > 150meq/L HYPOTONIC SOLUTIONS = < 260 mOsm/L Na < 130meq/L

33
CRYSTALLOIDS contain electrolytes (e.g., sodium, potassium, calcium, chloride) but lack the large proteins and molecules found in colloids. classified according to their “tonicity.” describes the concentration of electrolytes (solutes) dissolved in the water, as compared with that of body plasma (fluid surrounding the cells).
 dissolved in the water, as compared with that of body plasma (fluid surrounding the cells).")
34
COMPOSITION OF IV FLUIDS
OSMOLARITY (mosm/L) Na+ (mmol/L) K+ Cl- Base PNSS 308 154 ? PLR 273 130 D5LR 525 4 109 28 D5NR 552 140 98 50 D50.3NaCl 355 51 D5IMB 350 25 20 22 23 D5NM 368 40 3 16 D5W 255
 Na+ (mmol/L) K+ Cl- Base. PNSS PLR D5LR D5NR D50.3NaCl D5IMB D5NM D5W")
35
COLLOIDS contain solutes in the form of large proteins or other similarly sized molecules. Remain in the blood vessels for long periods of time and can significantly increase the intravascular volume (volume of blood).
.")
36
COLLOIDS/PLASMA EXPANDERS
Albumin = 1-2 kg/dose infused in 2 hours Haes-teryl = 20-40ml/kg Voluven = 20-40ml/kg Gelofuschin = 20-40ml/kg Fresh frozen plasma = 10-15ml/kg x 4 hours Dextran 40 or 60

37
BLOOD AND BLOOD PRODUCTS
are the most desirable fluids for replacement but are not the first choice for immediate volume expansion in children with shock Not only is the intravascular volume increased, but the fluid administered can also transport oxygen to the cells.

38
BLOOD AND BLOOD PRODUCTS
COMPUTATION pRBC 10 ml/kg to run for 4 hours Fresh whole blood 10-20 ml/kg in 4-6 hours Platelet Concentrate 15-20 ml/kg as fast drip Cryoprecipitate 1 unit/6kg/dose

39
Computation

40
OVERALL GOALS 1)ESTIMATE LOSSES Fluid & Electrolyte deficit
Maintenance requirements Ongoing losses 2)SELECT IV FLUID Initial replacement – always with ISOTONIC FLUID Maintenance requirement & ongoing losses
SELECT IV FLUID. Initial replacement – always with ISOTONIC FLUID. Maintenance requirement & ongoing losses.")
41
STEP ONE: Estimate Losses
SEVERITY OF DEHYDRATION INFANT (ml/kg) ADOLESCENT (ml/kg) CLINICAL SIGNS MILD 5% (50) 3% (30) Dry mucous membranes Oliguria MODERATE 10% (100) 6% (60) Poor skin turgor Sunken fontanel Marked oliguria Tachycardia Quiet tachypnea SEVERE 15% (150) 9% (90) Marked tachycardia Weak to absent distal pulses Narrow pulse pressure Hypotension and altered mental status
 ADOLESCENT (ml/kg) CLINICAL SIGNS. MILD. 5% (50) 3% (30) Dry mucous membranes. Oliguria. MODERATE. 10% (100) 6% (60) Poor skin turgor. Sunken fontanel. Marked oliguria. Tachycardia. Quiet tachypnea. SEVERE. 15% (150) 9% (90) Marked tachycardia. Weak to absent distal pulses. Narrow pulse pressure. Hypotension and altered mental status.")
42
STEP TWO: In shock?

43
MACRODRIP SETS = 10 – 15 drops (gtts)/ml
MICRODRIP SETS= 60 microdrops (ugtts)/ml)
/ml)")
44
(Volume in mL) x (drip set) gtts
= (Time in minutes) min
 min.")
45
CONVERSION FACTORS 1 ml = 15 drops (gtts) = 60 microdrops (ugtts) 1 drop (gtt) = 4 microdrops (ugtts) 1 microdrop (ugtts)/min = 1 ml/hour
 = 60 microdrops (ugtts) 1 drop (gtt) = 4 microdrops (ugtts) 1 microdrop (ugtts)/min = 1 ml/hour")
46
FLUID DEFICITS Ludan’s Method
WEIGHT MILD DEHYDRATION ml/kg/8 hours MODERATE DEHYDRATION SEVERE DEHYDRATION <15 kg 50 100 150 >15 kg 30 60 90 Give ¼ in 1 hr Give ¾ in 7 hr Give 1/3 in 1 hr Give 2/3 in 7hr PLAIN LR/PLAIN NSS D5LR PLAIN LR/ PLAIN NSS

47
FLUID DEFICITS – WHO *Use Ringer’s Lactate
SOME DEHYDRATION 75ml/kg in 4 hours SEVERE DEHYDRATION AGE FIRST GIVE 30ml/kg in: THEN GIVE 70ml/kg in: Infants under 12 months 1 hour 5 hours Older 30 minutes 2 ½ hours

48
SODIUM CORRECTION DEFICIT CORRECTION: desired-actual x weight x * Desired Na+ is meq MAINTENANCE COMPUTATION: maintenance x weight *Maintenance is 2-4meq/kg COMPUTE FOR ACTUAL Na+ Needed to be incorporated in your IV FLUID = Maintence + Deficit *Give the First ½ in 8 hours then ¼ in each succeeding 8 hour shifts to complete your 24 hour correction

49
POTASSIUM CORRECTION COMPUTE FOR THE K+ REQUIREMENT = 2-4meq/kg/day
DETERMINE how much KCL you will be incorporating in your IV fluid to complete a 24 hour correction Check IV fluid rate *Maximum 40meq/Liter of KCL incorporation in IV Fluid CHECK POTASSIUM INFUSION RATE (KIR) = meq of KCL x IV rate (ml/hour) x weight (maximum of 0.2meq/kg/hour)
 = meq of KCL x IV rate (ml/hour) x weight. (maximum of 0.2meq/kg/hour)")
50
MAINTENANCE REQUIREMENTS Holliday-Segar Method
BODY WEIGHT WATER (ml/kg/day) First 10 kg 100 ml/kg Second 10 kg (<20kg) 50ml/kg for each kg > 10kg ml Each additional kg (>20kg) 20ml/kg for each kg > 20kg ml
 First 10 kg. 100 ml/kg. Second 10 kg (<20kg) 50ml/kg for each kg > 10kg ml. Each additional kg (>20kg) 20ml/kg for each kg > 20kg ml.")
51
MAINTENANCE REQUIREMENTS Ludan Method
BODY WEIGHT (kg) TOTAL FLUID REQUIREMENT (TFR) at ml/kg/day > 3-10 kg 100ml/kg/day > kg 75ml/kg/day > kg 50-60ml/kg/day >30-60 kg 40-50ml/kg/day
 TOTAL FLUID REQUIREMENT (TFR) at ml/kg/day. > 3-10 kg. 100ml/kg/day. > kg. 75ml/kg/day. > kg ml/kg/day. >30-60 kg ml/kg/day.")
52
IV FLUID SELECTION INITIAL REPLACEMENT (GOAL: Restore Intravascular volume & Tissue Perfusion)– always with an ISOTONIC SOLUTION PNSS , PLR, PNR FOLLOW UP HYDRATION (For Ongoing Losses) – Isotonic/Hypertonic, can be Glucose containing D5LR, D5NR MAINTENANCE – Usually Hypotonic D5IMB , D5NM
 – Isotonic/Hypertonic, can be Glucose containing. D5LR, D5NR. MAINTENANCE – Usually Hypotonic. D5IMB , D5NM.")
53
FLUIDS NOT WORKING? Review medications: Dopamine Dobutamine
Norepinephrine Epinephrine Milrinone Vasopressin Nitroprusside

54
STEP THREE: Frequent Reassessment
Pulse quality Heart Rate Capillary Refill Time Urine Output Temperature Blood Pressure Neurologic Function Oxygen saturation Breath sounds and respiratory rate

55
STEP FOUR: Ancillary studies & Pharmacologic interventions
TREATMENT Shock etiology & severity Organ dysfunction Metabolic derangements Response to therapeutic interventions Medications Correct metabolic derangements Manage pain and anxiety Subspecialty consult

56
ADDITIONAL READING CASES
HYPOVOLEMIC SHOCK DISTRIBUTIVE SHOCK OBSTRUCTIVE SHOCK CARDIOGENIC SHOCK NEUROGENIC SHOCK OTHERS Diarrhea Sepsis Pericardial tamponade Brain tumor Poisonings DKA Tension pneumothorax Brain trauma Nephrotic/Nephritic syndrome Burns Ductal dependent heart lesions Fluids for newborns Dengue Massive pulmonary embolism Anaphylactic shock Trauma Surgical cases

57
BURNS Parkland Formula
Crystalloid at 4ml/kg x % BSA burned + Maintenance requirement Give ½ over the first 8 hours Then ½ over the next 16 hours *See Burn Assesment Chart for %BSA burned

58
DENGUE PPS 2010 Recommendations
NOT in Shock With MILD Dehydration D5LR/ D5NSS/ D50.9NaCl Maintenance rate using Holliday Segar/Ludan Correct in 24 hours D5LR/ D5NSS/ D50.9NaCl Maintenance rate (Ludan) + Mild Dehydration (Ludan) Give ½ in the first 8 hours Give the rest in the remaining 16 hours
 + Mild Dehydration (Ludan) Give ½ in the first 8 hours Give the rest in the remaining 16 hours")
59
END NELSON’S TEXTBOOK OF PEDIATRICS HARRIET LANE
PPS DENGUE 2010 GUIDELINES

60
CASE 1 year old MALE was brought to the ER by his hysterical mother due to sudden generalized tonic clonic convulsions and upward rolling of the eyeballs which occurred five minutes prior to consult. This is reported to be his first attack. On further investigation, you noted a 3 day history of vomiting followed by diarrhea. The vomiting occurs 2x/day, postprandial, amounting to ½ cup per episode.

61
The frequency of the diarrhea was 6-8 stools/day amounting to 1 cup/episode, watery, blood streaked; This was accompanied by fever (tmax 39) and intermittent episodes of abdominal pain; No known unusual food intake but the child plays with the neighborhood kids a lot and comes home very dirty. (+) decrease in appetite; Noted progressive decrease in activity
 decrease in appetite; Noted progressive decrease in activity .")
62
Last urine output noted 9 hours prior to consult; (+) Family history of BFC – paternal relatives The rest of the history was unremarkable
 Family history of BFC – paternal relatives The rest of the history was unremarkable")
63
PHYSICAL EXAMINATION Temperature 39; Heart rate 140/ minute; Respiratory rate 42/min; Blood pressure 90/60 Asleep, arousable; Not in respiratory distress; Good skin turgor; Pink, dry lips, no tpc, dry oral mucosa, sunken eyeballs, no clad; Equal chest expansion, clear breath sounds, no retractions;

64
Heart with regular rhythm, no murmurs; Abdomen tympanitic, soft, hyperactive bowel sounds Full and equal pulses

Similar presentations