Download presentation
Presentation is loading. Please wait.

1
La Dialisis Peritoneal como puente a la Hemodialisis
José Divino MD, PhD VP Medical Affairs Baxter Renal Division Latin America Congreso de la Sociedad Española de Nefrologia Cadiz 29 Septiembre 2007

2
The incidence of infection associated with
PD is no greater than that associated with HD. Data from the USRDS demonstrate that modality-related infections (i.e., peritonitis and vascular access infection) are lower in PD than in HD patients
 are lower in PD than in HD patients.")
3
What infections do dialysis patients get?
Infections directly related to the therapy: Hemodialysis Vascular access (catheters, grafts, fistulas) Peritoneal Dialysis Peritonitis, exit site infections Other infections Pneumonia Skin infections (esp with poor circulation) Dental, ENT (ear, nose, throat)
 Peritoneal Dialysis. Peritonitis, exit site infections. Other infections. Pneumonia. Skin infections (esp with poor circulation) Dental, ENT (ear, nose, throat)")
4
Bacteremia/Septicemia
Bacteremia is when a bacterial infection is found in the blood. This is documented by a blood culture growing out the organism. Patients may be mild to severely ill. Septicemia is when a patient has bacteremia and is clinically ill. In the USRDS, it means the patient is admitted to hospital. Local infections, e.g. skin infection, can cause bacteremia/septicemia, but not usually unless the local infection is severe.

5
Mortality from Infection: PD & HD
USRDS 2003 Annual Report

6
Reason for Admission: PD & HD
USRDS 2003 Annual Report

7
Bacteremia associated with PD is significantly less common
than with HD, and bacteremia associated with peritonitis is rare

8
Overall first-year hospital admission rates for septicemia, by modality: adjusted rates
Figure 6.38 Incident dialysis patients with 90-day rule; adjusted rates adjusted for age, gender, race, & primary diagnosis. Patients with Medicare as a secondary payor or enrolled in an HMO on day 90 are excluded, as are patients with septicemia claims overlapping the start date of the followup period.

9
Organisms in Sepsis: HD &PD
USRDS 2003 Annual Report

10
Foley et al JASN 2004;15:

11
Foley et al JASN 2004;15:

12
Mortality after first bacteremia/septicemia event: adjusted mortality rates
Figure 6.39 Incident dialysis patients, 1996–2000, with 90-day rule & with Medicare as primary payor; adjusted rates adjusted for age, gender, race, primary diagnosis, & vintage. Patients without sepsis in the first year + 90 days after initiation are used as the reference cohort.

13
Fig. 1. Cumulative incidence of bacteremia or septicemia over time in
the Wave 2 population.

14
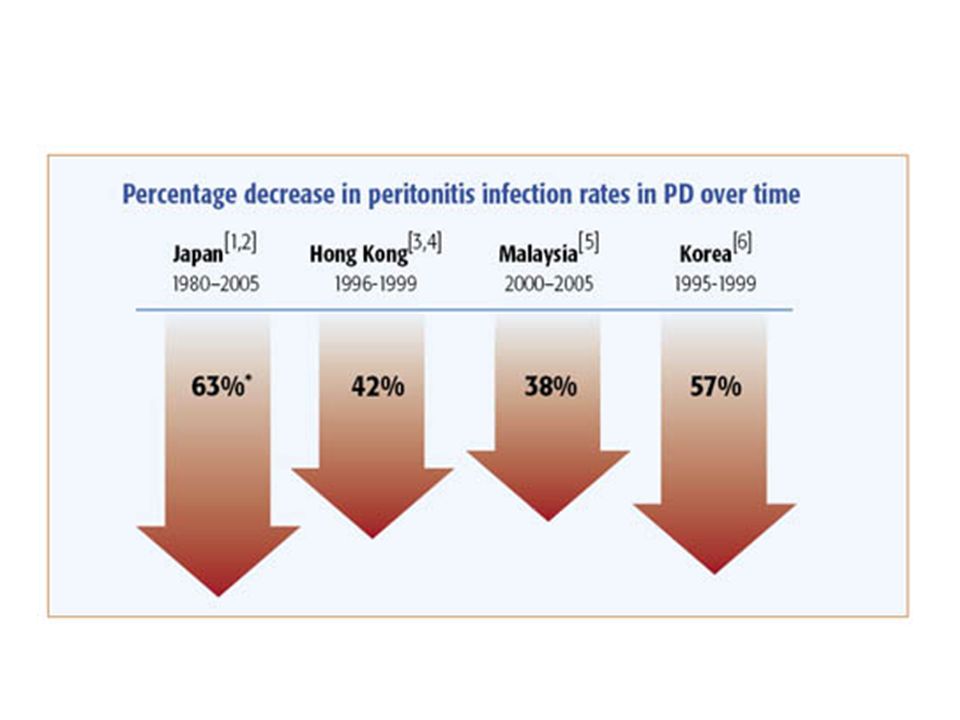
dramatically decreased over the last decade
The incidence of peritonitis associated with PD has dramatically decreased over the last decade

15
Why has peritonitis improved?
Advances in the systems “Flush before fill” Fewer connections Better appreciation of surgical issues Immobilization Not related to catheter type ISPD guidelines target 1 episode in every 18 patient months, but many programs do better and we should aim for better.

16
“Flush before fill”

17
Simplifying the Therapy UltraBag™ Integrated Disconnect System
Unique product design: Asymmetrical Y-junction with straight drain path Clinically validated for: Reduced potential of re-circulation1 Reduced potential of re-infusion of bacteria into peritoneum1 Easy for patients to use Reduced training time An optimal PD Delivery System needs to incorporate both contamination protection AND flush efficiency UltraBag distinguishes itself in the market due to it’s asymmetric Y. This design allows contaminents to flow directly away from the patient rather than re-circulate in the Y junction for possible re-infusion. Kubey,W., Straka, P., Holmes, C.J. (1998, January 27,) Importance of Product Design on Effective Bacterial Removal by Fluid Convection in Y Set and Tiwnbag Systems. Blood Purification, 16,
 Importance of Product Design on Effective Bacterial Removal by Fluid Convection in Y Set and Tiwnbag Systems. Blood Purification, 16,")
19
Remón et al. Nefrología 26 Nº1: 45-55, 2006

20
Technique success with PD has shown continuing improvement over time

21
Improved PD Reduced infection rates and easier to use systems have improved technique success with PD Drop rates remain high, ranging from 10-50% per year in different parts of the world Programs with greater experience have better outcomes

22
Mortality from Infection: PD & HD
USRDS 2003 Annual Report

23
Conclusions There are advantages of PD in managing common clinical issues seen in dialysis patients, and improvements are being made in managing clinical issues specifically related to PD

24
Why Start on PD ? Better preservation of RRF.
Initial survival advantage relative to HD. Better results after renal transplantation. Preservation of vascular access

25
Access outcome 3.8 - 9.7 bacteremias per 1000 catheter days
Incidence of bacteremia from temporary CVC’s Internal Jugular 5.4% after 3 weeks Femoral 10.7% after 1 week bacteremias per 1000 catheter days Oliver et al: KI 2000; 58: 2543

26
Hospitalization in the first year of RRT for ESRD
Prospective study of 526 incident patients starting RRT. 1 year follow up. Univariate analysis: The most common single reason for admission was creation of & complications to vascular access for HD. The use of temporary vascular access for HD were associated with prolonged hospitalization & repeated admissions. Patients initially treated with HD rather than PD spent longer time in hospital & were more likely to be admitted. Metcalfe et al. Q J Med 2003; 96: 899

27
The more than 10-fold increase in mortality in ESRD patients is mainly due to CVD and infections USRDS analysis stratified by gender, race, and age CVD Sepsis 0,001 0,01 0,1 1 10 100 25-34 35-44 45-54 55-64 65-74 75-84 85+ Age (years) Annual mortality (%) 0.0001 0.001 0.01 0.1 10 100 25-34 35-44 45-54 55-64 65-74 75-84 85+ Age (years) Annual mortality (%) ESRD ESRD GP GP Foley et al. Am J Kidney Dis 1998,32:S112-S119 Sarnak et al. Kidney Int 2000 Oct;58(4): Pecoits-Filho & Lindholm 2003
 Annual mortality (%) Age (years) Annual mortality (%) ESRD. ESRD. GP. GP. Foley et al. Am J Kidney Dis 1998,32:S112-S119. Sarnak et al. Kidney Int 2000 Oct;58(4): Pecoits-Filho & Lindholm")
28
Central venous catheter (CVC) and its risks
They are exposed to risks of venous dialysis catheter insertion, and catheter-related infection and thrombosis. Development of (long-term) access-failure is correlated with both use of central venous catheter, and premature puncture of access system at start of dialysis. ( Vanholder 2001)
 access-failure is correlated with both use of central venous catheter, and premature puncture of access system at start of dialysis. ( Vanholder 2001)")
29
Complications of catheter usage
Limited ability to provide adequate dialysis Related to size of CVC: - Diameter - Length Recirculation Placement problems Complications Tip location Thrombosis Extrinsic Intrinsic Infection Exit site Tunnel Catheter related bacteremia

30
Peritoneal Dialysis as a bridge in chronic hemodialysis patients
Juan Fernández Cean

31
Three treatment options for
End Stage Renal Disease: HD PD RT

32
Vascular access in chronic HD patients :
Arteriovenous fistulae (AVF) Arteriovenous grafts (AVG)
 Arteriovenous grafts (AVG)")
33
Vascular access in chronic HD patients :
Arteriovenous fistulae (AVF) Arteriovenous grafts (AVG) Venous Catheter (VC) is used as a bridge in CHD patients
 Arteriovenous grafts (AVG) Venous Catheter (VC) is used as a bridge in CHD patients.")
34
The outcome of HD patients depends on the vascular access:
Arteriovenous fistulae (AVF) Arteriovenous grafts (AVG) Venous Catheter (VC)
 Arteriovenous grafts (AVG) Venous Catheter (VC)")
35
Septicemia, access and cardiovascular disease in dialysis patients: The USRDS Wave 2 Study.
Ishani A, Collins A, Herzog C and Foley R. Kidney International (2005) 68, Risk of bacterimia
 68, Risk of bacterimia.")
36
Septicemia, access and cardiovascular disease in dialysis patients: The USRDS Wave 2 Study. Ishani A, Collins A, Herzog C and Foley R. Kidney International (2005) 68, Risk of bacterimia

37
Annual mortality rate according to the vascular access
Type of vascular access and survival among incident HD patients: the Choices for healthy outcomes in caring for ESRD (CHOICE) study. Astor B et al. JASN, March 2005 Annual Mortality rate (%)
 study. Astor B et al. JASN, March Annual Mortality rate (%)")
38
Type of vascular access and survival among incident HD patients: the Choices for healthy outcomes in caring for ESRD (CHOICE) study. Astor B et al. JASN, March 2005 Mortality (%) PD
 PD.")
39
Type of vascular access and survival among incident HD patients: the Choices for healthy outcomes in caring for ESRD (CHOICE) study. Astor B et al. JASN, March 2005 Mortality (%) PD
 PD.")
40
Haemodialysis vascular access problems in Canada: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS II) David C. Mendelssohn1, Jean Ethier2, Stacey J. Elder3, Rajiv Saran4,5, Friedrich K. Port3 and Ronald L. Pisoni3 NDT- March 2006; 21: 46 % 66 % 70 % Fig. 2. Vascular access use among new ESRD (incident) patients in Canada, Europe and the USA in DOPPS II, 2002–2004 (n = 2025). Analysis included incident patients who entered DOPPS within 5 days of their first ever chronic HD treatment.
 patients in Canada, Europe and the USA in DOPPS II, 2002–2004 (n = 2025). Analysis included incident patients who entered DOPPS within 5 days of their first ever chronic HD treatment.")
41
Haemodialysis vascular access problems in Canada: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS II) David C. Mendelssohn1, Jean Ethier2, Stacey J. Elder3, Rajiv Saran4,5, Friedrich K. Port3 and Ronald L. Pisoni3 NDT- March 2006; 21: 18 % 25 % 33 % Fig. 1. Vascular access use among prevalent HD patients in Canada, Europe and the USA in DOPPS II, 2002–2003 (n = 6460). From data collected on a prevalent cross-section of HD patients at 252 dialysis units participating in DOPPS during 2002–2003 from Canada, Europe (France, Germany, Italy, Spain, Sweden and the UK) and the USA. Sample weights were employed to account for the differing proportions of patients sampled in each facility.
. From data collected on a prevalent cross-section of HD patients at 252 dialysis units participating in DOPPS during 2002–2003 from Canada, Europe (France, Germany, Italy, Spain, Sweden and the UK) and the USA. Sample weights were employed to account for the differing proportions of patients sampled in each facility.")
42
Colonia de bacterias dentro de la capa de biofilm, sobre la superficie de un catéter vascular
Raad I. Intravascular catheter related infections. Lancet 1998; 351:

43
Venous catheters are a necessary bridge to perform HD when there is an AVF-AVG complication or at the initiation of HD Venous Catheter AVF or AVG AVF or AVG Thromboses, infection Venous Catheter AVF or AVG Initiation of HD

44
Three treatment options for
End Stage Renal Disease: HD PD RT

45
End Stage Renal Disease:
Three or four ? treatment options for End Stage Renal Disease: HDcat PD HDavf RT

46
Patients with venous catheter at the initiation of HD
% % % ESRD patients arriving in an emergency situation for the first dialysis treatment Juan Fernández-Cean ASN 37th Annual Meeting.2004

47
LA DIALYSIS OVERVIEW: ESRD AND PD Patients

48
Nephrol Dial Transplant (2002) 17: 2226-2230
Infective endocarditis in chronic haemodialysis: two treatment strategies Juan Fernández-Cean, Asunción Alvarez, Sergio Burguez, Graciela Baldovinos, Patricia Larre-Borges and Mercedes Cha Nephrol Dial Transplant (2002) 17:
 17:")
49
Infective Endocarditis, incidence in general population and in chronic dialysis (1996)
Incidence per person- years 0.65 39 48 11 Abbott K et al. Hospitalization for Bacterial Endocarditis after initiation of Chronic Dialysis in the United States. Nephron 2002;91:

50
Infective Endocarditis in chronic HD In-hospital mortality
Country Year Mortality HD General population Francia % % Hanslik NDT, 12:1301-2,1997 USA % Robinson, AJKD 30:521-4, 1997 Uruguay % Fernández, NDT 17: , 2002

51
Infective Endocarditis and vascular access
HD Removal of the infected vascular access IE HD with a new venous catheter (as a bridge) AVF, AVG or Venous catheter PD (as a bridge)
 AVF, AVG or Venous catheter. PD (as a bridge)")
52
Infective endocarditis in chronic haemodialysis: two treatment strategies
Juan Fernández-Cean, Asunción Alvarez, Sergio Burguez, Graciela Baldovinos, Patricia Larre-Borges and Mercedes Cha Nephrol Dial Transplant (2002) 17: Period: HD (n: 21) IE HD (n: 9) Vascular access removal PD (n: 12)
 17: Period: HD (n: 21) IE. HD (n: 9) Vascular access removal. PD (n: 12)")
53
Characteristics of patients
HD (9) PD (12) P All Age 58 +16 NS SEX m/f 4/5 7/5 11/10 Diabetes 2 Cancer 1 3 Valv. disease 4 8 Prosthetic valve Time in HD (months)
 PD (12) P. All. Age NS SEX m/f. 4/5. 7/5. 11/10. Diabetes. 2. Cancer Valv. disease Prosthetic valve. Time in HD (months)")
54
Patients Number Mortality of deaths
Two treatment strategies in infective Endocarditis in HDC (n= 21) - Mortality Patients Number Mortality of deaths All % HD % P: 0.03 PD % Nephrol Dial Transplant (2002) 17:
 - Mortality. Patients Number Mortality of deaths. All % HD % P: PD % Nephrol Dial Transplant (2002) 17:")
55
Infective endocarditis in chronic haemodialysis: two treatment strategies
Juan Fernández-Cean, Asunción Alvarez, Sergio Burguez, Graciela Baldovinos, Patricia Larre-Borges and Mercedes Cha Nephrol Dial Transplant (2002) 17: 5 HD (9) 4 HD (21) 1 EI PD (12) 3 8
 17: HD (9) 4. HD (21) 1. EI. PD (12)")
56
PD could also be used as a bridge when there is an AVF complication or at the initiation of HD
Venous Catheter AVF or AVG AVF or AVG PD Thromboses, infection Venous Catheter AVF or AVG Initiation of HD PD

57
These results suggest that if PD is utilized as a bridge to HD, the hospitalization and mortality associated with infectious endocarditis in chronic HD patients may be significantly reduced. In those case where the use of a central venous catheter is being considered, PD can be applied as a safer transitory solution, “a bridge”, while the patient receives an AV fistula and it matures

58
Considerar el uso de DP como un “puente” La colocación del catéter peritoneal asocia menos complicaciones DP puede iniciarse inmediatamente luego de colocado el catéter La frecuencia de complicaciones infecciosas es menor durante su utilización Se puede planificar un acceso vascular definitivo para HD

59
Perspectives in renal medicine
Hemodialysis access failure: a call to action. R Hakim and J Himmelfarb. Kidney Int, Vol 54 (1998), pp Se debe considerar el uso de DP como un “puente” en los pacientes que presentan uremia avanzada y no son candidatos ideales para tratamiento prolongado con DP. El inicio de tratamiento sustitutivo con DP, en tanto permite que madure la FAV o prótesis, puede mejorar la sobrevida de los accesos vasculares y del paciente.
, pp Se debe considerar el uso de DP como un puente en los pacientes que presentan uremia avanzada y no son candidatos ideales para tratamiento prolongado con DP. El inicio de tratamiento sustitutivo con DP, en tanto permite que madure la FAV o prótesis, puede mejorar la sobrevida de los accesos vasculares y del paciente.")
60
Fernandez-Cean J et al, WCN 2007
Access related morbidity in hemodialysis and peritoneal dialysis patients J. Fernández-Cean*1, G. Baldovinos1, A. Stein2, A. Varela1, V. Matonte3, N. Orihuela4, M. Garau1, I. Olaizola1, C. González1, R. López1, M. Mautone5, M. Pereyra1, Z. Lydia1, A. Petraglia1, R. Lombardi2, S. Orihuela4, T. Gómez4, A. Altuna1, C. Tenca1, E. Carbonell2 1HD, SARI, 2HD, INU, Montevideo, 3HD, CAMEDUR, Durazno, 4PD, Uruguayana, 5PD, Americano, Montevideo, Uruguay Fernandez-Cean J et al, WCN 2007

61
Fernandez-Cean J et al, WCN 2007
Introduction: Venous catheters (VC) are used as an unavoidable bridge in ESRD patients in HD, at the initiation or when there are complications of the arteriovenous access (AVA). Many publications stress that morbidity and mortality are higher in HD patients treated with VC. Fernandez-Cean J et al, WCN 2007
 are used as an unavoidable bridge in ESRD patients in HD, at the initiation or when there are complications of the arteriovenous access (AVA). Many publications stress that morbidity and mortality are higher in HD patients treated with VC. Fernandez-Cean J et al, WCN")
62
Fernandez-Cean J et al, WCN 2007
Introduction: Venous catheters (VC) are used as an unavoidable bridge in ESRD patients in HD, at the initiation or when there are complications of the arteriovenous access (AVA). Many publications stress that morbidity and mortality are higher in HD patients treated with VC. In this study we analyze the different vascular access (VA) used in a population of chronic HD patients and the related morbidity. The results are compared with those of PD patients. Fernandez-Cean J et al, WCN 2007
 are used as an unavoidable bridge in ESRD patients in HD, at the initiation or when there are complications of the arteriovenous access (AVA). Many publications stress that morbidity and mortality are higher in HD patients treated with VC. In this study we analyze the different vascular access (VA) used in a population of chronic HD patients and the related morbidity. The results are compared with those of PD patients. Fernandez-Cean J et al, WCN")
63
Introduction: Venous catheters (VC) are used as an unavoidable bridge in ESRD patients in HD, at the initiation or when there are complications of the arteriovenous access (AVA). Many publications stress that morbidity and mortality are higher in HD patients treated with VC In this study we analyze the different vascular access (VA) used in a population of chronic HD patients and the related morbidity. The results are compared with those of PD patients. Our hypothesis is that PD could be safer than VC as a bridge in patients without a usable AVA.
 are used as an unavoidable bridge in ESRD patients in HD, at the initiation or when there are complications of the arteriovenous access (AVA). Many publications stress that morbidity and mortality are higher in HD patients treated with VC. In this study we analyze the different vascular access (VA) used in a population of chronic HD patients and the related morbidity. The results are compared with those of PD patients. Our hypothesis is that PD could be safer than VC as a bridge in patients without a usable AVA.")
64
Fernandez-Cean J et al, WCN 2007
Patients and Methods: All HD and PD patients treated in 5 dialysis centers (3 HD centers and 2 PD Centers) from January 1, 2004 to November 30, 2006 were included Variables recorded in the observation period Demographics: age, sex, diabetes HD or PD access: type (AVA, VC, PD catheter) date of creation and date of last use Hospitalization days (Hosp-s) Date of death, Transplantation or lost of follow-up. Fernandez-Cean J et al, WCN 2007
 from January 1, 2004 to November 30, 2006 were included. Variables recorded in the observation period. Demographics: age, sex, diabetes. HD or PD access: type (AVA, VC, PD catheter) date of creation and date of last use. Hospitalization days (Hosp-s) Date of death, Transplantation or lost of follow-up. Fernandez-Cean J et al, WCN")
65
Access related morbidity in hemodialysis
and peritoneal dialysis patients 319 patients HD PD ALL Patients Diabetic (%) Older than 65 (%)
 Older than 65 (%)")
66
Access related morbidity in hemodialysis
and peritoneal dialysis patients 319 patients HD PD ALL Patients Diabetic (%) Older than 65 (%) Access changes (changes per person-year) (0.50) (0.07) (0.38)
 Older than 65 (%) Access changes (changes per person-year) (0.50) (0.07) (0.38)")
67
Access related morbidity in hemodialysis
and peritoneal dialysis patients 319 patients HD PD ALL Patients Diabetic (%) Older than 65 (%) Access changes (changes per person-year) (0.50) (0.07) (0.38) AVA VC Hosp-days per 1000 person-month
 Older than 65 (%) Access changes (changes per person-year) (0.50) (0.07) (0.38) AVA. VC. Hosp-days per person-month.")
68
Fernandez-Cean J et al, WCN 2007
Conclusion: These HD patients had a higher rate of change in dialysis access than the PD patients. In this investigation, morbidity, measured by Hosp-d, is lower in PD than in HD patients with a venous catheter and the difference is statistically significant. This result fits with our hypothesis and could be a reason to consider PD as a bridge in HD patients without a usable AVA. Fernandez-Cean J et al, WCN 2007

69
Limitations: Restrospective

70
Limitations: Restrospective Prevalent and incident patients

71
Limitations: Restrospective Prevalent and incident patients Mortality was not analyzed

72
VASCULAR ACCESS SITE RELATED INFECTION IN DIALYSIS (V.A.R.I.):
a multicenter, prospective, Italian study. The A.St.R.I.D. project A.St.R.I.D. Rio de Janeiro, 23 April 2007

73
Aim of the study To assess the V.A.R.I. rates To identify variables associated with them

74
Participating centres
11 dialysis units: 10-50 technical beds

75
Patients: 940 - age: 65±15 years
Study population Patients: age: 65±15 years - male 57 % # vascular accesses: Total follow-up: pt-months Median patient f.u.: months Total access f.u.: 334,306 days # dialysis sessions: 142,883 treatments

76
Patient characteristics
# of patients % Housing: alone ,6 nursing home ,1 family ,2 Malnourished: ,7 Diabetics: ,1 HBsAg positive: ,4 HCVAb positive: ,6 HIV positive: ,4 Karnofsky (median): 86 (IQR: 60-90)
: 86 (IQR: 60-90)")
77
Reported events 883 events, requiring hospitalization or antibiotic therapy V.A.R.I. 18% Not infectious event 41% Infection not access related 41%

78
Distribution of pathogens
% S. aureus 41 26.1% S. epidermidis 29 18.5% Other Coagulase negative Staphylococci 39 24.8% E. coli 25 15.9% Klebsiella 1 0.6% Enterobacter spp. 3 1.9% P. aeruginosa 5 3.2% S. malthophilia Candida albicans Other 8 5.1% 69.4

79
Factors associated to VARI-1*
Variable Category HR p Sex F vs M Type of vascular access (vs AVF) Graft 6.43 <0.001 p CVC <0.001 t CVC <0.001 HCV yes vs no 1.34 NS HBV yes vs no 1.65 NS HIV yes vs no 1.49 NS * Univariate Cox regression analysis
 Graft 6.43 < p CVC < t CVC < HCV yes vs no 1.34 NS. HBV yes vs no 1.65 NS. HIV yes vs no 1.49 NS. * Univariate Cox regression analysis.")
80
Factors associated to VARI-2*
Variable Category HR p Number of dialysis session per week NS Housing (vs. nursing home) living with family living alone 0.89 NS Karnofsky per 10 points increase 0.82 <0.001 Diabetes yes vs no 1.27 NS Malnutrition yes vs no 1.38 NS Impaired immune syst. drug related disease related * Univariate Cox regression analysis
 living with family living alone 0.89 NS. Karnofsky per 10 points increase 0.82 < Diabetes yes vs no 1.27 NS. Malnutrition yes vs no 1.38 NS. Impaired immune syst. drug related disease related * Univariate Cox regression analysis.")
81
Multivariate analysis
Only the type of access retained statistical significance

82
Infection rates Infection risk per patient: 1.19 per 100 patient-month Infection risk per access: 0.38 per 1000 access-days 0.26 per 1000 dialysis sessions

83
Infection-free survival
AVF Graft pCVC tCVC 365 730 Kaplan Meier analysis

84
Conclusion The incidence of VARI is elevated in dialysis population
The pathogen responsible of infection is mainly Staph Aureus CVC, either permanent or temporary, have a very high incidence of VARI AVF remains the “preferred” vascular access and any effort for reducing the use of CVC must be done

Similar presentations










 patients Policy.>")








