Download presentation
Presentation is loading. Please wait.

1
END-OF-LIFE CARE HEART FAILURE and COPD Dr Sally Reeder Specialty Doctor in Palliative Medicine

2
LIFE-LIMITING ILLNESS
Symptoms Patient and carer needs Psychological support Spiritual needs Social isolation Carer support Quality of Life

3
PARALLEL SYMPTOMS Lethargy Decreased mobility Pain Dyspnoea Anorexia
Nausea Depression Anxiety Decreased QOL

4
DIFFERENCES Predicting mortality Terminal phase
Understanding of diagnosis and prognosis Discussions about prognosis End-of-Life discussions Contact with health and social services Financial support Availability of specialist services in community

5
NON-CANCER PATIENTS Unpredictable illness trajectory
Acute events – hospital admissions Patient attitude to diagnosis Timing of death uncertain ?opportunities for End-of-Life discussions Patient choice Palliative specialist involvement limited

6
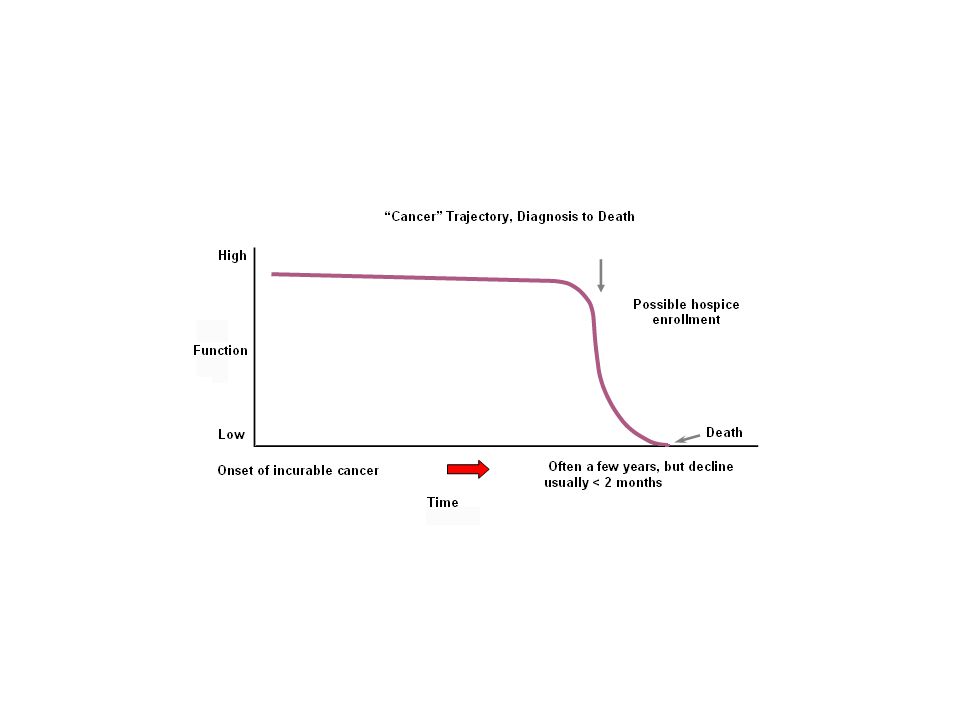
ILLNESS TRAJECTORIES 3 typical illness trajectories
-Steady progression eg: cancer -Gradual decline eg: HF / COPD -Prolonged gradual decline eg: dementia / old age

9
WHO DEFINITION of PALLIATIVE CARE
An approach that improves quality of life. Life-threatening illness Prevention and relief of suffering Early identification Impeccable assessment Treatment – physical, psychological, spiritual.

10
LIFE-LIMITING ILLNESSES
PALLIATIVE MEDICINE LIFE-LIMITING ILLNESSES

11
WHO SHOULD DELIVER THIS PALLIATIVE CARE? General Practitioners?
Cardiologists? Specialist clinic staff? WHEN AND WHERE SHOULD IT BE DELIVERED? At diagnosis? Clinic appointments? Hospital admissions? GP appointments?

12
SHOULD THE PALLIATIVE CARE TEAM BECOME INVOLVED,
AND WHEN? Hospital-based Palliative Specialists Hospice out-patient clinics Day Hospice attendance Hospice admission

13
BARRIERS to ACCESSING SPECIALIST PALLIATIVE CARE SERVICES

14
From Cardiology Palliative care only for dying patients
Need to continue active intervention Concerns medications will be stopped Lack of understanding what SPC can offer

15
From Specialist Palliative care
Floodgates will open / patient load Stretch charitable funding ? Skills to manage these patients Chronically ill - ? Exacerbation ? Block beds

16
From Patients I don’t have cancer I’m not dying Distressing
Lack of understanding – their disease palliative care

17
COST

18
HEART FAILURE / COPD ?

19
AN EQUITABLE SERVICE All life-limiting illnesses under SPC umbrella
Early introduction to the service Patient and carer education End-of-Life discussions PPC documents Day hospice

20
END-STAGE HEART FAILURE
Optimal treatment but still symptomatic Principles of Symptom control Assessment and investigation Intervention to reversible factors Palliation of irreversible factors Rationalisation of medication Renal dysfunction / Hypotension

21
MEDICATIONS Statins – stop Aspirin / Clopidogrel – stop
ACE Inhibitors – reduce if renal dysfunction Loop diuretics Spironolactone B Blockers Digoxin – stop, unless in AF

22
BREATHLESSNESS Common Assess for treatable causes
Infection ; Effusion: PE; underlying Ca; pulmonary oedema asthma; COPD; anxiety Oxygen - ?benefit Opioids – careful monitoring Anxiolytics Non –pharmacological measures breathing techniques; fan:pacing;

23
PAIN in HEART FAILURE Angina; - ct anti-anginal medication as long as possible musculoskeletal; arthritis; Gout WHO analgesic ladder Avoid NSAIDs Amitriptyline

24
NAUSEA Consider cause Medication – opioids; digoxin toxicity; spironolactone constipation; renal failure anxiety Avoid Cyclizine – strong anticholinergic effects Metoclopramide Levomepromazine Haloperidol Syringe driver

25
OTHER SYMPTOMS Fatigue
Over-diuresis; hypokalaemia; poor sleep; anaemia; depression; PND; periodic respiration; sleep apnoea Depression Avoid tricyclics Itch Good skin care of oedematous legs; SSRI Constipation Avoid bulking agents eg: fybogel

26
TERMINAL STAGE Not tolerating oral medication Syringe driver
Analgesics Antiemetics Anxiolytics Diuretic Liverpool Care Pathway LCP

27
End-Stage COPD Difficult to diagnose
Persistent breathlessness despite optimum treatment Severe airflow obstruction FEV1 <30% Housebound An increased frequency of hospital admissions Fear / anxiety

28
STUDY of COPD PATIENTS NEEDS
Diagnosis and disease process Treatment options Prognosis What dying might be like Advance care planning ie: identical to needs of cancer patients!

29
End – Stage COPD Respiratory and non-respiratory symptoms
BREATHLESSNESS Decreased mobility Wheeze Depression Cough Social isolation Fatigue Pain Poor sleep Worse standard of daily life than Lung Ca

30
MANAGEMENT Bronchodilators Anticholinergics Oxygen Anxiolytics Opioids
Coping strategies purse-lip breathing; slow expiration; lean forward Pyschological support – end-of–life planning

31
GOING FOR GOLD Equitable end-of-life care
ALL appropriate patients on palliative register Avoid un-necessary hospital admissions Advanced care planning Patient choice

32
Domiciliary Visits Primary care team + Hospice Dr
Aim - to recognise end-stage - respect patients choices - control symptoms - prevent hospital admissions - strive for a “good death”

33
COPD PILOT Looking at providing an equitable service
Recognising the different illness trajectories Meeting patients needs Introduction to the Hospice Acknowledging what's already available

34
COPD PILOT Joint clinic at St Johns Hospice RLI Respiratory team
SJH Doctor / Day hospice nurse Physio / OT / CT COPD patients chosen by respiratory team FEV1 < 30 > 3 admissions 6 week programme

Similar presentations




>")







 Noreen Baxter Respiratory Nurse Specialist May 2005.>")







