Download presentation
Presentation is loading. Please wait.

1
A Regional Public Health System in NH
What Do We Have Now? Why Regionalize? How Do We Make a Case for Regional Public Health in a State Like NH? What Would Change?

2
What Does Public Health Look Like in NH Today?
Each of New Hampshire’s 234 cities and towns are required by law to have a health officer Only five New Hampshire communities maintain public health departments of various size ; no county health departments At the State level, DHHS is the lead public health agency. The Department of Environmental Services, Department of Education, and Department of Safety also play key roles In almost all New Hampshire communities, non-governmental organizations provide a significant sub-set of public health services

3
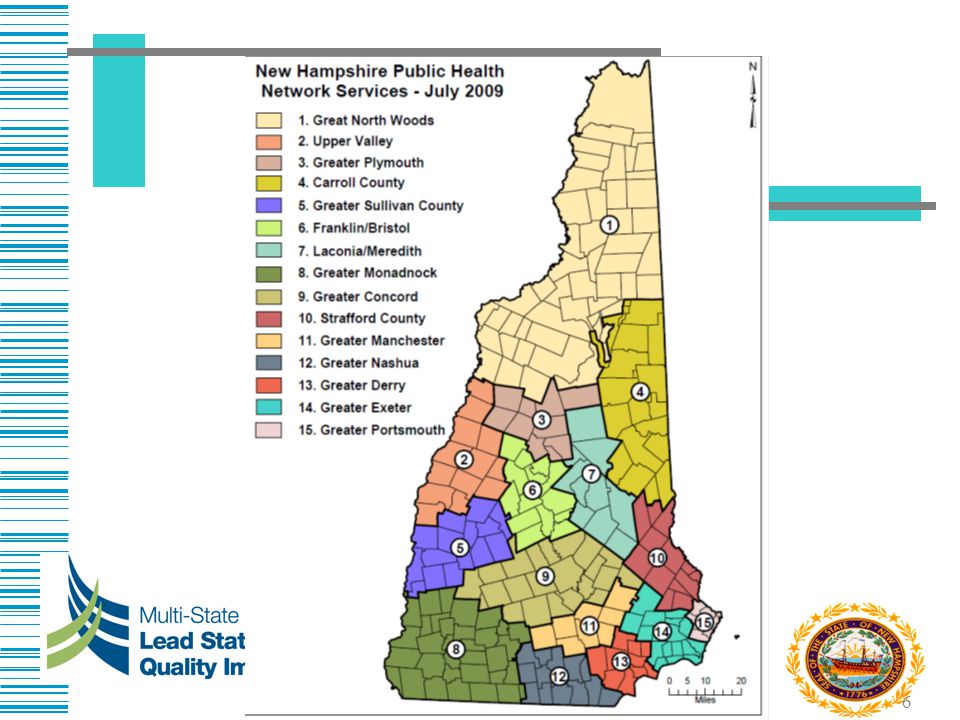
2004 New Hampshire Public Health Network
“Assuring the health and safety of all NH residents” 14 Coalitions 118 Towns 50% of NH towns 70% of the NH population covered 5-11 communities per coalition

4
All Health Hazard Regions
Organized to plan for and respond to public health emergencies 19 Regions

5
And more maps for other services
Community health centers Tobacco coalitions WIC services HIV prevention Etc, etc, etc.

7
Why Regionalization?

8
Potential Benefits of Regionalization
Study in the AJPH, March 2006 examined performance of public health agencies, size and resources It noted that small public health agencies may benefit by combining resources and operations But gains may diminish with size – too big is not good (but NH is small in both geography and population) Mays, G, McHugh, M et al. AJPH, March 2006 Vol. 96, No. 3
 Mays, G, McHugh, M et al. AJPH, March 2006 Vol. 96, No. 3.")
9
Regionalization Goal Overall Goal – A performance-based public health delivery system, which provides all 10 essential public health services throughout New Hampshire Provide high quality public health based on national standards

10
Why do we need regional public health in one of the healthiest states?
What is killing us and making us sick today are chronic illnesses (heart disease, cancer, respiratory disease, injuries) Many of the contributing factors to these are preventable – tobacco, diet, physical activity, alcohol consumption Well-run community based public health programs can prevent these problems Money can be saved
 Many of the contributing factors to these are preventable – tobacco, diet, physical activity, alcohol consumption. Well-run community based public health programs can prevent these problems. Money can be saved.")
11
What is Public Health ? The study and practice of managing threats to the health of a community or population The public health approach is applied to populations ranging from a handful of people to the whole human population Priorities are to prevent (rather than treat) a disease or injury through the study of cases; promoting healthy behaviors; preventing the spread of disease; and addressing policy issues.
 a disease or injury through the study of cases; promoting healthy behaviors; preventing the spread of disease; and addressing policy issues.")
12
Individual vs. Populations
How does public health differ from health care? . Individual vs. Populations

13
Example- Smoking Health care response Public Health Response
Treat an individual for smoking related health problems – asthma, pneumonia, heart disease, cancer, etc. Counsel to quit smoking Provide nicotine replacement therapy Public Health Response Study the effects of tobacco – Surgeon General’s report Labeling of cigarettes Public information campaigns Promote policies such as non-smoking workplaces Enforcement of laws such as limiting tobacco sales to minors

14
Public Health Goes to You
Unlike personal health care services, in many cases the public does not have to travel to receive public health services Public health staff go out to do investigations Public health staff analyze diseases by populations Public health education campaigns are delivered where people go or access information (radio,TV, billboards, schools, workplaces, etc.) So public health regions do not need to align exactly with hospitals or doctors offices service areas
 So public health regions do not need to align exactly with hospitals or doctors offices service areas.")
15
Public Health Saves Money
$10 per person per year in proven community-based disease prevention (improvements in physical activity, nutrition and preventing smoking) could yield saving of $2.8 billion in health care costs in 2 years That’s $2 in return for every $1 invested in the first 1-2 years Prevention for a Healthier America:Investments in Disease Prevention Yield Significant Savings, Stronger Communities. Trust for America’s Health July
 could yield saving of $2.8 billion in health care costs in 2 years. That’s $2 in return for every $1 invested in the first 1-2 years. Prevention for a Healthier America:Investments in Disease Prevention Yield Significant Savings, Stronger Communities. Trust for America’s Health July")
16
Obesity for example 23.6 % population is obese, 61.8% are overweight or obese – significant increase from NH ranks 35th in the nation, despite having the lowest poverty rate Worst in New England ¹ For the first time in 2 centuries our children’s life expectancy is potentially less than ours (2-5 years) due to obesity and related factors (diabetes, heart disease, kidney failure, cancer) F as in Fat: How Obesity Policies are Failing in America 2008, Trust for America’s Health, August NEJM March 2005
 due to obesity and related factors (diabetes, heart disease, kidney failure, cancer) F as in Fat: How Obesity Policies are Failing in America 2008, Trust for America’s Health, August NEJM March")
17
Example - Obesity Health Care Response
Treatment for conditions such as heart disease, high blood pressure, diabetes, cholesterol Nutritional counseling Bariatric surgery Public Health Response Working with schools to provide healthy lunch menus Working with community coalitions to develop walkable communities Assist in developing policies for physical activities in schools

18
The 10 Essential Public Health Services

19
The Proposed Approach The DPHS and Regionalization Initiative workgroup envision one lead public health agency per region. It must be linked a governmental entity that is responsible to coordinate or directly provide the 10 essential services. The lead agency may subcontract or create memoranda of understanding for some essential services Regions based on existing ones (many are quite similar) and take into account geographic features, existing public health services and population size Two levels of public health (primary and comprehensive) that acknowledge existing resources and capacity to carry out public health services. Comprehensive = Manchester and Nashua Primary = everywhere else
 and take into account geographic features, existing public health services and population size. Two levels of public health (primary and comprehensive) that acknowledge existing resources and capacity to carry out public health services. Comprehensive = Manchester and Nashua. Primary = everywhere else.")
20
Approach Will be based on national standards for what a public health agency should look like and how it should perform Will be an evolutionary process – some may not meet all components of a primary agency from the beginning but will move there in time. Will require changes to state law.

21
The Role of Government in Public Health
Assessment – Takes into account all relevant factors to the extent possible, based on objective factors, without self-interest Policy Development – Takes place as a result of interactions among public and private organizations Assurance – Assures that necessary services are provided to reach agreed upon goals by encouraging the private sector, requiring it, or providing services directly

22
A Primary Regional Public Health Agency
Staff, funding, and legal recognition to assure a fundamental public health presence Performs some level of the 10 essential services Collaborates extensively with system partners in the region to coordinate more comprehensive services The NH DPHS continues to provide some core services (i.e.. lab, disease investigations) to these regions Coordinates with local health officers or move towards shared health officer among municipalities
 to these regions. Coordinates with local health officers or move towards shared health officer among municipalities.")
23
Proposed Staffing Every region would have: Shared across regions:
Administrator Health educator/marketing staff Nurse (?) Environmental health specialist Support staff Shared across regions: Epidemiologist Emergency preparedness coordinator Medical consultant (Shared or in-kind) Financial manager IT support
 Environmental health specialist. Support staff. Shared across regions: Epidemiologist. Emergency preparedness coordinator. Medical consultant. (Shared or in-kind) Financial manager. IT support.")
24
How is this Different than the Public Health Networks?
Proposal that there be a legally-recognized regional public health council which… Designates a lead public health entity that… Is responsible to the council and regional public health system partners for… Implementing a coordinated approach to provide public health services to the public

25
Next Steps-What Do We Have?
Assessments to Help Us Determine, Resources, Costs, Needs and Approach June February 2010 Financial analysis of all state/local/private public health funding with consideration of efficiencies from regionalization – Patrick Bernet, FAU Assessment of local/regional public health system capacity to deliver the 10 essential services- with a gaps analysis – Lea Lafave, CHI Assessment of what the link to government could look like - Jennifer Wierwille Norton

26
Financial Assessment To gain an understanding of current public health expenditures in each region and for the state as a whole Will capture state, municipal and private-sector funding To try to understand the potential financial implications of regionalizing select public health services

27
Lead organization : Regional Partners : State
Capacity Assessment Purpose To identify assess and gaps in the region and these that may lend themselves to regionalization. Process: Framework of the National Association of City and County Health Officials Essential Service Standard Indicator Revised Tool Lead organization : Regional Partners : State Each region in the state (7 to start) You are first!! So, the purpose of the assessment is….and this is part of a greater effort of public health regionalization that is underway in NH. It is part of an effort to build the public health infrastructure, and so, we are assessing the assets and gaps of each region as they relate to deviverying the 10 essential public health services. Now, if you have any questions about the 10 essential services or whether you deliver any of them, you will hopefully have a very clear understanding before too long, and by the end of the day. And, as I mentioned, as our first regional assessment. Until today it has been all very conceptual. We are truly assessing the process of the assessment, and looking for how it can be improved. Until today it has been all very conceptual.
 You are first!! So, the purpose of the assessment is….and this is part of a greater effort of public health regionalization that is underway in NH. It is part of an effort to build the public health infrastructure, and so, we are assessing the assets and gaps of each region as they relate to deviverying the 10 essential public health services. Now, if you have any questions about the 10 essential services or whether you deliver any of them, you will hopefully have a very clear understanding before too long, and by the end of the day. And, as I mentioned, as our first regional assessment. Until today it has been all very conceptual. We are truly assessing the process of the assessment, and looking for how it can be improved. Until today it has been all very conceptual.")
28
What is the Governance Assessment?
Focuses on figuring out who’s responsible or held accountable; not doing the work but overseeing it; Who’s overseeing performance of the public health entities who are partners. Who’s assessing the degree to which the partners in the region have the necessary authority, resources and policies to provide essential public health services. Assures that the infrastructure exists to protect and promote health in the community.

29
Governance Assessment in Two Parts
Part I: Examining Readiness to Serve in a Governance Function: The first part of the assessment provides a tool to measure the region’s readiness to serve as governing body or Public Health Council to oversee the delivery of services and programs. Part II: Examining Types of Lead Public Health Entities Participants will use part II of the tool to hold a facilitated discussion about the different options available for the region’s Public Health Council to choose as a lead public health entity (type of entity).
.")
30
What Will Change? Statewide, regional and more formalized recognized system, in law that provides a more even level of each essential service Coordinates the current fragmented system that delivers very different levels of service More efficient use/better coordination of existing resources Based on national standards -PHAB

31
What Won’t Change? Municipalities retain legal authority for enforcing state laws and local ordinances DPHS provides some core services such as lab and disease control Local agencies will still receive funds directly from DPHS but will need to be part of the regional system

32
And the benefits will be…
Higher quality services at the best possible cost Ability to measure ourselves against national standards Better positioning for increasingly competitive federal funds

33
Questions? Joan Ascheim
NH Dept of HHS, Division of Public Health Services ext. 4110 Lea Lafave Community Health Institute/JSI

Similar presentations
>")










![The Role of Governance in Public Health Accreditation [Insert your name and title] [Insert LHD]](/2/732128/big_thumb.jpg "The Role of Governance in Public Health Accreditation [Insert your name and title] [Insert LHD]>")




 Changes Iowa Medicaid Enterprise October 14, 2008.>")
 In Kuwait>")

