Download presentation
Presentation is loading. Please wait.

1
the inservice exam Feb 25, 2009 Short term $$$ (moonlighting, Mets)
Long term $$$$$$ (licensure, career in EM) But also: intro to EM practice Similar questions to ABEM Last year: 207 questions counted Physician’s Evaluation and Educational Review VII Las Vegas Board Review Course MP3s (2003?) EMEDS Review sinaiem.org/files/articles/BR-emeds/ … jar files
 But also: intro to EM practice. Similar questions to ABEM. Last year: 207 questions counted. Physician’s Evaluation and Educational Review VII. Las Vegas Board Review Course MP3s (2003 ) EMEDS Review sinaiem.org/files/articles/BR-emeds/ … jar files.")
2
This lecture series Board review: Five months, 20 lectures…
Different than Dr. Cherkas sessions This year: More engagement than More questions, buzzwords than last year More repetition More candy

3
OB+GYN+GU About 19 questions in PEER VII (out of 410)
Some overlap in ID, S+S, Procedures + Skills Last year’s inservice: it was 8+7 out of 207 CV, GI, Pulm, Trauma each ~20 Likely emphasis: details that make or break ED diagnosis or management

4
OB+GYN+GU Today: Pregnancy, UTI, PID
Select Male Concerns: scrotal and penile No renal / stones / HD / PD complications You already got some STDs from Jim Hinchey

5
Warning: Graphic Photos of our Holiday Parties

8
Question 1 A 32 year old man presents with a painful erection that has lasted for more than 10 hours. Which of the following medications is the most likely cause of this condition? Olanzapine Not the psych drug (Zyprexa) you should be thinking of… Pseudoephedrine No – this is a therapy (only if given early) Terbutaline No – this is a therapy (0.25 mg subQ q30 min … in the deltoid) Trazodone Most causes of priapism are iatrogenic, from anti-HTN or psych meds Venlafaxine Also linked to priapism but much less common than trazodone
 you should be thinking of… Pseudoephedrine. No – this is a therapy (only if given early) Terbutaline. No – this is a therapy (0.25 mg subQ q30 min … in the deltoid) Trazodone. Most causes of priapism are iatrogenic, from anti-HTN or psych meds. Venlafaxine. Also linked to priapism but much less common than trazodone.")
9
Priapism Low flow (90%, ischemia), venous obstruction Meds (psychotropics, antihistamines, anti-HTN, viagra, cocaine) Hematologic (sickle cell, leukemia, thalassemia) Intra-cavernosal injections (pre-1998) Spinal cord injuries Painful 12+ hours to thrombosis and ischemia impotence High flow (10%), arterial source Secondary to groin or straddle injury Arterial cavernosal shunt Less pain, no fibrosis Treat with embolization
 Intra-cavernosal injections (pre-1998) Spinal cord injuries. Painful. 12+ hours to thrombosis and ischemia impotence. High flow (10%), arterial source. Secondary to groin or straddle injury. Arterial cavernosal shunt. Less pain, no fibrosis. Treat with embolization.")
10
Priapism Rx General Treatment: Sickle cell: PRBCs, hyperbaric oxygen
Focus on pain control, urinary obstruction, hydration, O2 (sicklers) Alpha-adrenergic antagonists: terbutaline IM, intracorporal phenylephrine Corporal aspiration Shunt surgery Sickle cell: PRBCs, hyperbaric oxygen Iatrogenic (due to penile injections for impotence) Leukemia: terbutaline, chemo Non-reversible causes: idiopathic, high spinal cord injury, meds
 Alpha-adrenergic antagonists: terbutaline IM, intracorporal phenylephrine. Corporal aspiration. Shunt surgery. Sickle cell: PRBCs, hyperbaric oxygen. Iatrogenic (due to penile injections for impotence) Leukemia: terbutaline, chemo. Non-reversible causes: idiopathic, high spinal cord injury, meds.")
11
Question 2 A 47 year old uncircumcised, obese man presents with painful “tip of the penis.” Exam shows a swollen and tender glans and foreskin. On retraction, the foreskin appears excoriated and has a foul-smelling, purulent discharge. No other findings are present. What is the diagnosis? Balanoposthitis Balanitis (glans) + foreskin! Usually skin flora. Treat with sitz, cleaning, keflex. If it’s cheesy, it’s candida. May be the presenting sign for diabetes – check a FSBS! Fournier’s gangrene Patient not immunocompromised, no systemic signs or spreading beyond tip. Herpes simplex Vesicles… not discharge. Paraphimosis Can’t extend. Vicious cycle; true emergency. Give ice, sugar, puncture… slit? Phimosis Can’t retract. Can lead to pain, UTI. Dilate, plus 4-6 weeks of steroid cream.
 + foreskin! Usually skin flora. Treat with sitz, cleaning, keflex. If it’s cheesy, it’s candida. May be the presenting sign for diabetes – check a FSBS! Fournier’s gangrene. Patient not immunocompromised, no systemic signs or spreading beyond tip. Herpes simplex. Vesicles… not discharge. Paraphimosis. Can’t extend. Vicious cycle; true emergency. Give ice, sugar, puncture… slit Phimosis. Can’t retract. Can lead to pain, UTI. Dilate, plus 4-6 weeks of steroid cream.")
12
Balanoposthitis Balanitis = inflammation of the glans penis
Posthitis = inflammation of the foreskin Cause: Usually Staph/Strep, can be fungal Poor hygiene, undiagnosed DM, seborrheic dermatitis Rx: Local measures: soap, drying Antifungal cream, possible broad spectrum antibiotics (cephalosporin)
")
13
Phimosis / Paraphimosis
Phimosis = inability to retract foreskin Uncommon cause of urinary retention Congenitial or bc of chronic balanoposthitis Paraphimosis = retracted skin that cannot be reduced A true urologic emergency Can lead to gangrene of glans bc of arterial compromise Leave foley in place if present Rx: If unable to reduce manually Use Local anesthetic at constricting band, make superficial vertical incision to decompress

14
Question 3 A 13 year old boy is brought in for sudden onset of groin pain. On exam, the patient’s right testis is swollen, tender, and slightly elevated in the scrotum. Which of the following statements regarding this condition is correct? CT is the imaging study of choice CT gives great anatomy… but who wants IV, radiation on a kid’s nads? Duplex ultrasonography provides little data about testicular anatomy US is 100% specific for torsion, good anatomy. Manual detorsion shouldn’t wait. Positive cremasteric reflex confirms the diagnosis Reflex should be absent in torsion Relief of pain with elevation reliably differentiates this condition from epididymitis Relief of pain with elevation (Prehn’s sign) suggests epididymitis… not reliable… The “bell-clapper” deformity predisposes patients to this condition Tunica vaginalis (a fold of peritoneum) should just cover superior pole of testis and attach to posterior scrotum. If it covers entire testicle and attaches to spermatic cord, testis can rotate more freely.
 suggests epididymitis… not reliable… The bell-clapper deformity predisposes patients to this condition. Tunica vaginalis (a fold of peritoneum) should just cover superior pole of testis and attach to posterior scrotum. If it covers entire testicle and attaches to spermatic cord, testis can rotate more freely.")
15
Testicular Torsion Cause: twisting of the spermatic cord
Maldeveloped testes (at baseline tend to lie more horizontal than vertical = bell clapper deformity) Findings: Young male with abdominal pain Peak incidence in puberty but can occur at any age Sudden onset of pain, not changed by scrotal elevation Absence of cremasteric reflex (normal: stroking proximal medial thigh causes testicle to elevate) Tests: Ultrasound Doppler, Nuclear Scan Rx: Emergent urology consult for surgical repair May try Manual Derotation while waiting (rotate testicle in lateral direction, “open book.” Relief of pain indicates success.)
 Findings: Young male with abdominal pain. Peak incidence in puberty but can occur at any age. Sudden onset of pain, not changed by scrotal elevation. Absence of cremasteric reflex (normal: stroking proximal medial thigh causes testicle to elevate) Tests: Ultrasound Doppler, Nuclear Scan. Rx: Emergent urology consult for surgical repair. May try Manual Derotation while waiting. (rotate testicle in lateral direction, open book. Relief of pain indicates success.)")
16
Testicular Appendage Torsion
Cause: twisting of pedunculated structures on the epididymis or testis More common than testicular torsion in prepubertal boys Findings: “Blue Dot Sign:” pathognomonic, represents hemorrhage of appendage visualized through thin scrotal skin. Tests: Doppler ultrasound Rx: Possible surgery. May not be necessary if doppler of testicle is normal.

17
Epididymitis Cause: Inflammatory process (gradual)
Can be infectious or due to reflux of sterile urine Young boys: think of congenital abnormalities Gram neg. Secondary to structural, neurologic, functional abnormalities of lower tract Sexually active: usually STD-related If Gram neg, give erythromcin Elderly: think of obstruction (prostate, stricture) Usually E.coli and Klebsiella 5-25% of testicular cancers are initially misdiagnosed as epididymitis S/Sxs: gradual onset of pain Prehn’s sign = relief of pain with elevation of scrotum Rx: Abx as indicated by age, NSAIDs, bed rest, scrotal support, intermittent ice packs
 Usually E.coli and Klebsiella. 5-25% of testicular cancers are initially misdiagnosed as epididymitis. S/Sxs: gradual onset of pain. Prehn’s sign = relief of pain with elevation of scrotum. Rx: Abx as indicated by age, NSAIDs, bed rest, scrotal support, intermittent ice packs.")
20
Acute Prostatitis Cause: S/Sxs: Prostate massage is contraindicated
Sexually Active: consider STD (GC) Elderly: consider E.coli S/Sxs: Perineal pain, dysuria, frequency, fever/chills, urinary retention “Boggy” enlarged, tender prostate Prostate massage is contraindicated May lead to bacteremia
 Elderly: consider E.coli. S/Sxs: Perineal pain, dysuria, frequency, fever/chills, urinary retention. Boggy enlarged, tender prostate. Prostate massage is contraindicated. May lead to bacteremia.")
21
Question 4 A 56 year old man with DM II presents with 3-4 days of fever and groin pain. There is no hx of recent illness, but glucose levels have been difficult to control for over a week. His exam is in the next figure. What is the most appropriate initial treatment? Can we do this, Cherkas-style? High-dose intravenous penicillin Hyperbaric oxygen therapy Intravenous piperacillin/tazobactam Suprapubic catheterization Surgical debridement

23
Question 4, continued A 56 year old man with DM II presents with 3-4 days of fever and groin pain. There is no hx of recent illness, but glucose levels have been difficult to control for over a week. His exam is in the next figure. What is the most appropriate initial treatment? High-dose intravenous penicillin Not enough coverage (most common Cx is E. coli, Bacteroides, and staph…) Hyperbaric oxygen therapy An adjunct, and a controversial one. Certainly not initial therapy. Intravenous piperacillin / tazobactam Could go for pen (for G+ and C. perfringes) plus aminoglycoside or 3g cephalo for gram negs, plus anaerobe coverage with metronidazole or clinda. Suprapubic catheterization May become necessary, depending on extent. But not initial therapy for this pt. Surgical debridement Almost certainly necessary, but not the initial treatment.
 Hyperbaric oxygen therapy. An adjunct, and a controversial one. Certainly not initial therapy. Intravenous piperacillin / tazobactam. Could go for pen (for G+ and C. perfringes) plus aminoglycoside or 3g cephalo for gram negs, plus anaerobe coverage with metronidazole or clinda. Suprapubic catheterization. May become necessary, depending on extent. But not initial therapy for this pt. Surgical debridement. Almost certainly necessary, but not the initial treatment.")
24
Scrotal Abscess Must differentiate between abscess of the skin (hair follicle carbuncle/furuncle) vs. Abscess of scrotal contents Skin abscess Rx: I&D, no abx Intra-scrotal abscess can be a complication of epididymitis Ultrasound can help to distinguish Must differentiate from Fournier’s Low threshhold for Urologic Consultation

25
Fournier’s Gangrene Surgical Emergency Cause: Findings:
Extensive tissue loss and increased mortality with delayed diagnosis Cause: Polymicrobial infxn of subcutaneous tissue that originates either in the skin, urethra, rectum Immunocompromised at risk (DM,EtOH, IVDA, chronic steroids) Findings: Can start as a benign infection or abscess Quickly becomes “virulent” with crepitus Always consider this in any pt with scrotal, rectal or genital pain or tachycardia out of proportion to clinical findings
 Findings: Can start as a benign infection or abscess. Quickly becomes virulent with crepitus. Always consider this in any pt with scrotal, rectal or genital pain or tachycardia out of proportion to clinical findings.")
26
Question 5 In the treatment of a 3 year-old boy with UTI, which of the following additional signs is the strongest indication for hospital admission? Localized myalgias whatever Maculopapular rash not really associated with UTI at any age Marked fever no – this is often the presenting symptom Mucoid diarrhea may help distinguish UTI from AGE at this age, shouldn’t affect dispo Persistent vomiting Vomicking unable to take ABx, mandates IV therapy and admission

28
Question 6 A 24 year old woman complains of dysuria, urgency, and frequency. She denies f/c, no n/v, no back pain. She has no known drug allergies and a urine pregnancy test is negative. Bedside urine dip shows 3+ blood, 1+ nitrites, and 1+ leukocyte esterase. What is the most appropriate course? Order a urine culture and treat with an appropriate ABx for 3 days Rosen’s and Tintinalli say no culture is necessary, only 10-20% will fail empiric tx Order a urine culture and treat with an appropriate ABx for 7 days Not pregnant, not a male, not elderly, not diabetic, no hx of prior UTI’s… Treat with an appropriate ABx for 3 days Empiric therapy without UCx is appropriate if no risk factors for complications Treat with an appropriate ABx for 7 days 3d is enough. Use local abiogram to guide ABx choice. Wait for microscopic analysis of the urine before deciding whether to order a urine culture. Wait for FEW ORG SEEN ??? A UTI patient should be your fastest dispo of the day.

29
Urinary Tract Infection
Cause: E.coli (90%), Klebsiella, Proteus, Enterobacter (5-20% combined) Males usually secondary to urologic disease Dx: Sxs CFUs of single pathogen Relapse = same organism & serotype, < 1 month since initial infection Reinfection = recurrence of sxs 1-6 months after initial infection, usually different organism
, Klebsiella, Proteus, Enterobacter (5-20% combined) Males usually secondary to urologic disease. Dx: Sxs CFUs of single pathogen. Relapse = same organism & serotype, < 1 month since initial infection. Reinfection = recurrence of sxs 1-6 months after initial infection, usually different organism.")
30
UTIs: Deeper Thoughts Complicated UTIs Asymptomatic bacteriuria:
Underlying urologic pathology, pregnancy, immunocompromised, usually not E.coli Asymptomatic bacteriuria: Can progress to symptomatic infection, especially in pregnancy Acute Urethral Syndrome +Dysuria, but with low (or no) bacterial count in urine cultures. UA often positive. Generally indicates infection & should be treated Dysuria Ddx: chlamydia, herpes, GC, vaginitis
 bacterial count in urine cultures. UA often positive. Generally indicates infection & should be treated. Dysuria Ddx: chlamydia, herpes, GC, vaginitis.")
31
UTIs: Lab Tests Nitrite: specific (90%) but not sensitive (50%)
Based on bacteria-induced change of nitrate to nitrite (varies by bug, urine incubation) Leukocyte Esterase: similar (80% sp, 48% sn) Based on presence of WBCs in urine Pyuria = 2-5 WBC in females, 1-2 WBC in males Bacteriuria = any bacteria in an uncentrifuged gram stain smear, or > 15/HPF in centrifuged specimen Chlamydia infection can be associated with low WBC and low bacterial counts
 Leukocyte Esterase: similar (80% sp, 48% sn) Based on presence of WBCs in urine. Pyuria = 2-5 WBC in females, 1-2 WBC in males. Bacteriuria = any bacteria in an uncentrifuged gram stain smear, or > 15/HPF in centrifuged specimen. Chlamydia infection can be associated with low WBC and low bacterial counts.")
32
UTIs: When to Culture? Pyelonephritis, recent hx pyelonephritis
Underlying urologic pathology Children, Males Diabetics, Immunocompromised Recent Instrumentation, Indwelling catheter Prolonged Sxs prior to Rx 3 or more UTIs in the past year DO NOT need to culture young, healthy women with uncomplicated UTIs DO need to r/o other sources of pyuria/dysuria: STDs, prostatitis, pyelonephritis, epididymitis

33
Adult UTI Treatment Female, lower tract, nonrecurrent, simple
TMP/SMZ BID x 3d Quinolone x 3d Female, lower tract, complicated / or Male, upper tract TMP/SMZ x 10d Macrobid x 10d Cefadroxil x 10d Amox/Augmentin x 10d Quinolone x 10d Female, lower tract, suspected STD Doxycycline x 10d TMP/SMZ x 10d Erythromycin x 10d (E.coli not covered) culture for chlamydia, GC Think Pseudomonas in high-risk patients Cover with broad spectrum Abx
 culture for chlamydia, GC. Think Pseudomonas in high-risk patients. Cover with broad spectrum Abx.")
34
High-Risk Pyelonephritis
Pregnancy: Incidence of pyelonephritis increases in the 3rd trimester and may precipitate preeclampsia, sepsis & miscarriage DM, Sickle Cell Anemia Renal Calculi / obstruction Elderly / Debilitated Carcinoma, Chemotherapy Recent hospitalization Recent instrumentation of UT Pyelonephritis = leading cause of perinephric abscess

35
Question 7 A 17 year old woman complains of dysuria x3 days. She denies f/c, no n/v/d, no abd pain. Pelvic exam reveals a homogenous white discharge that coats the vaginal walls. Pregnancy test is negative. Wet mount shows clue cells. The best treatment is: azithromycin this is not chlamydial urethritis or PID! (chlamydia is #1 reported STI) ceftriaxone this is not gonococcal urethritis or PID! fluconazole if it were fungal, they would have said cottage cheese.. levofloxacin this is not a UTI! and levaquin has poor anaerobe coverage… metronidazole therapy of choice in both pregnant and nonpregnant patients. A seven-day course of clinda cream or pills is also acceptable. Metronidazole also works on trichomonas, which can present similarly to vaginosis (but is described with dyspareunia, dysuria, and a wet mount that shows flagellates).
 ceftriaxone. this is not gonococcal urethritis or PID! fluconazole. if it were fungal, they would have said cottage cheese.. levofloxacin. this is not a UTI! and levaquin has poor anaerobe coverage… metronidazole. therapy of choice in both pregnant and nonpregnant patients. A seven-day course of clinda cream or pills is also acceptable. Metronidazole also works on trichomonas, which can present similarly to vaginosis (but is described with dyspareunia, dysuria, and a wet mount that shows flagellates).")
36
Gardnerella (BV) New term: Anerobic Vaginosis
Gram negative rod, faculatative anaerobe “fishy” order, rather than maldorous Clue cells: anaerobes sticking to squamous epithelial cells. Looks like a fried egg with salt and pepper under microscope. Rx: Flagyl. Truly, flagyl in first trimester is controversial.

38
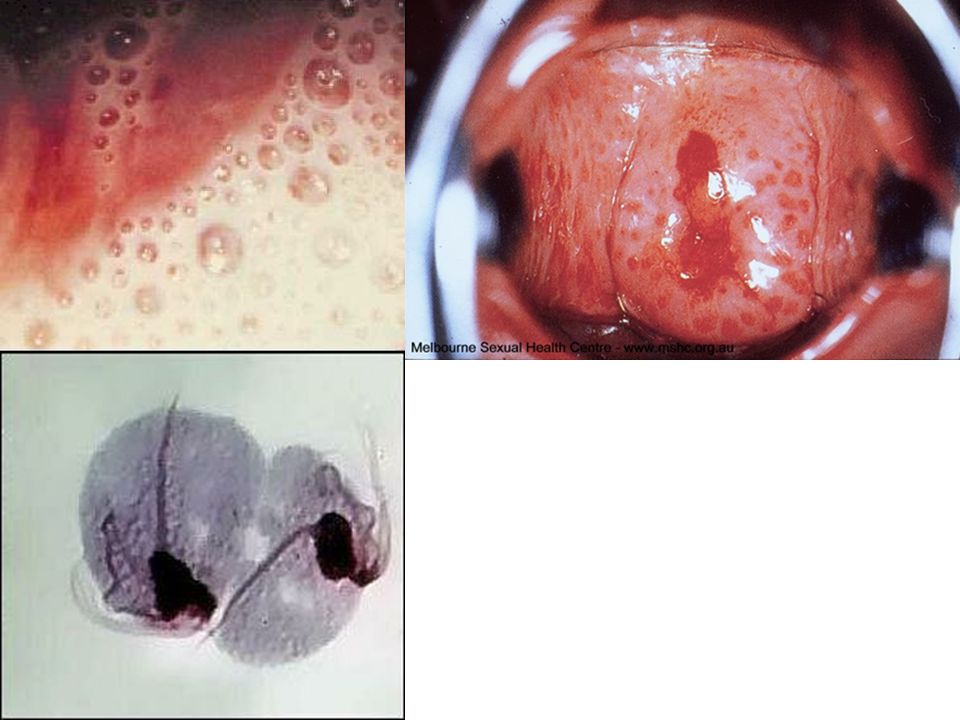
Trichomonas Women: Frothy, grey, malodorous
Men: asymptomatic, urethritis Drop it on slide: see swimming things Word STRAWBERRY: GOES WITH TRICH Other strawberries: tongue A protozoan. Rx: Flagyl (not intuitive) Think Flagyl if you have no idea what to use! (giardia, anaerboes, ameobas, other parasites) What else should you be doing after you treat the patient: treat partner Single dose therapy In Pictures: look like fat sperm
 Think Flagyl if you have no idea what to use! (giardia, anaerboes, ameobas, other parasites) What else should you be doing after you treat the patient: treat partner. Single dose therapy. In Pictures: look like fat sperm.")
40
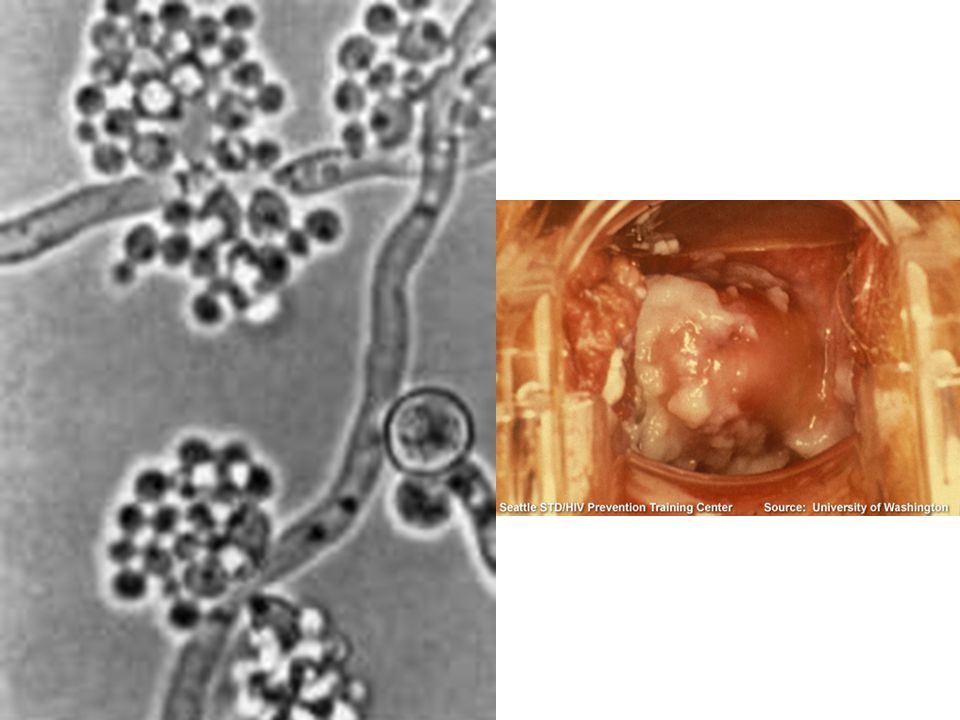
Candida Yeast Risk factors: Cottage cheese, no smell
diabetes (common presentation of new onset DM) contraception antibiotics Cottage cheese, no smell Drop on slide: KOH dissolves other elements, leaves behind hyphae (spaghetti) and spores (meatballs) RX: single treatment of fluconazole, or lotrimin suppository
 contraception. antibiotics. Cottage cheese, no smell. Drop on slide: KOH dissolves other elements, leaves behind hyphae (spaghetti) and spores (meatballs) RX: single treatment of fluconazole, or lotrimin suppository.")
43
Question 8 A 23 year old woman presents complaining of lower abdominal pain. Pelvic exam reveals yellow vaginal discharge, as well as moderate CMT. Adnexa are tender, but no masses are present. Outpatient management may be considered if the patient has: A physician who can provide followup care It’s hard to discharge PID: Poor followup, adolescence, HIV, N/V, ambiguity… Pelvic abscess Um, no. This would be a reason for IV ABx, admission Positive urine pregnancy test No. Pregnancy should actually protect against PID – this presentation is ominous. Already taken antibiotics for similar complaints So they’ve failed outpatient therapy and need IV ABx and admission Temperature greater than 38.8C Fever is not uncommon but I guess the PEER folks found this concerning

44
PID/Salpyngitis Causes: Neisseria gonorrhoeae, chlamydia trachomatis (#1), Gardnerella vaginalis, anerobes Ascending disease: starts in cervix, goes through tubes Risk Factors: anything that mucks up the tubes. Previous PID, IUD, adolescent w/multiple partners

45
PID, continued Can’t be ruled on physical exam. FORGET CMT
CMT, adnexal tenderness, elevated temperature, discharge DON’T NEED TO ADMIT ALL PATIENTS Consider for: Pregnancy—this is very uncommon Immunosuppressed IUD Clinically ill Outpatient compliance issues Fertility issues TOA peritonitis

46
More on PID Cervical culture not correlates with actually causative organism. Treatment always empiric Complicatons: Chronic pain/dyspareunia TOA infertility (most common cause of infertility) Fitz-Hugh-Curtis: RUQ pain w/o biliary disease Watch out in RUQ pain questions on boards. What is the next thing you do? answer is pelvic exam F-H-C catch phrase: violin strings (adhesions between capsule of liver and abdominal wall)
 Fitz-Hugh-Curtis: RUQ pain w/o biliary disease. Watch out in RUQ pain questions on boards. What is the next thing you do answer is pelvic exam. F-H-C catch phrase: violin strings (adhesions between capsule of liver and abdominal wall)")
48
If recurrent/chronic/fails treatment, think anaerobes. FLAGYL
PID Rx: treat Gonorrhea and chlamydia. Gonococci: ceftriaxone/cefuroxime or quinolone (single dose) Chlamydia/anaerobes: doxy 10 days (slower turnover rate) If recurrent/chronic/fails treatment, think anaerobes. FLAGYL
 Chlamydia/anaerobes: doxy 10 days (slower turnover rate) If recurrent/chronic/fails treatment, think anaerobes. FLAGYL.")
50
Question 9 The side effects of emergency contraception meds can be reduced by: Avoiding their use in smokers Risk of VTE goes up with OCP use and age over 35, obesity, and smoking Peri- or post-ovulatory administration Actually there’s theoretical risk of ectopic here – the P might cause ciliary dysfxn. Taking the pill before a meal Symptoms of n/v, headache, fatigue are benign. Abd pain must get ectopic w/u Using a progestin-only regimen WHO ‘98 says P dosing within 72 hours is more effective than Yuzpe, fewer AE Using combination pills with both estrogen and progestin Yuzpe ‘74 method is two E+P doses, twelve hours apart, within 72 hours of sex.

51
Miscarriages (definitions old fashioned)
Threatened: if pain and bleeding but os is closed. Both internal and external have to be closed Instructions: don’t put anything in your vagina Inevitable: same thing, but os open Incomplete: passed some, not all tissue (at the os) Missed: baby dies, don’t have abortion. Not common.
 Missed: baby dies, don’t have abortion. Not common.")
52
Abortions, cont. Board question: if missed situation described & pt has fever: septic abortion. Worry about DIC in these cases polymicrobial Septic abortion: most common is polymicrobial (“polymicrobial” also associated with diabetic foot ulcer questions)
")
53
Question 10 A 26 year old woman who is 6 weeks pregnant presents with RLQ pain opf 10 hours’ duration. The pain began periumbilically and migrated to the RLQ. She has nausea which she attributes to pregnancy. She has a fever of 38C and elevated WBC with left shift. UA is normal. Sono shows IUP, but the appendix was not visualized. What is the next appropriate management step? Admit for observation Lots of overlap between appendicitis (nausea, WBC, pain) and pregnancy. Discharge with instructions to return in 12 hours for repeat exam This is a high-risk patient who should not leave. CT of abdomen and pelvis Risk to fetus is low, but specialists’ input is preferable. Consult surgery and OB She’s febrile and pregnant with abd pain. They’re going to need to get involved. Start IV fluid hydration and observe in the ED for six hours Delaying the diagnosis of appy can lead to increased M+M, fetal loss (up to 20%)
 and pregnancy. Discharge with instructions to return in 12 hours for repeat exam. This is a high-risk patient who should not leave. CT of abdomen and pelvis. Risk to fetus is low, but specialists’ input is preferable. Consult surgery and OB. She’s febrile and pregnant with abd pain. They’re going to need to get involved. Start IV fluid hydration and observe in the ED for six hours. Delaying the diagnosis of appy can lead to increased M+M, fetal loss (up to 20%)")
54
Safe imaging in pregnancy
Diagnostic Radiology in pregnancy: If it’s indicated, do it. D-dimer has no defined norms, just rises. Helpful if negative… Rad Threshold is 50 mSv. ?Others say fetus = 10. CXR = 0.02 mSv. CTAngio = 5-30… if it’s indicated, do it. Weeks 2-8: Organogenesis. Rads teratogen Weeks 8-15: Neuro development at risk Weeks 15+ … much less risk

58
Question 11 Which of the following conditions is most likely to be associated with a hydatiform mole? Abdominal pain It’s not more common than pain with normal pregnancy Abnormally low beta-hCG Not an ectopic! beta-hCG will actually be much higher than dates suggest Hyperemesis Most likely to be associated with the Mole. Hypothyroidism The Mole will make its own thyroid hormones, may trigger pre-eclampsia Vaginal discharge May present with bleeding, sure. Also see large uterus, large ovaries, may be passing grape clusters (hydropic villi).
.")
59
Molar pregnancy Associated with Asians, first pregnancies, teens or 40’s 1st and 2nd trimester bleeding The only possible cause of first-trimester pre-eclampsia Chorionic villi tumor, not actually a fetus 46XX is complete, more likely to be malignant. Path needed to tell complete from incomplete (69XXXY, more benign) No fetal heart, uterus bigger than normal. Hcg very high (100,000s) “Snowstorm” appearance on ultrasound
 No fetal heart, uterus bigger than normal. Hcg very high (100,000s) Snowstorm appearance on ultrasound.")
61
Normal pregnancy Morning sickness: associated with good overall outcomes 12 wks: pelvic brim 20 wks: umbilicus Highest at 36th week, then fundus descends Increased CO 20-30% Most women get a hydronephrosis of pregnancy Chadwick’s sign: soft, blue cervix (venous, ok) Rabbit done died?
 Rabbit done died")
62
Human Chorionic Gonadotropin
Doubles every hours Becomes positive after implantation, about a week (8-9 days) after intercourse After first missed period, you will be positive Miscarriage: works in reverse. Gets cut in half every 2-3 days.
 after intercourse. After first missed period, you will be positive. Miscarriage: works in reverse. Gets cut in half every 2-3 days.")
63
Pregnancy Complications
Appendicitis: most common surgical condition in pregnancy (same incidence as in age-matched nonpregnant patients). Difficult to diagnose: already have increased wbc, appy in RUQ UTI in preg: consider as upper tract infections. Longer course (10 day), send culture If pyelonephritis, admission +/- if sick
. Difficult to diagnose: already have increased wbc, appy in RUQ. UTI in preg: consider as upper tract infections. Longer course (10 day), send culture. If pyelonephritis, admission +/- if sick.")
65
Question 12 Which of the following is a characteristic of the HELLP syndrome? Increased LDH Why not HELLDHLP? Hemolytic anemia implies elevated LDH Neurologic symptoms May help distinguish HELLP from TTP (but bad HELLP can cause seizures) Normal antithrombin III Helps distinguish HELLP (low) from TTP, HUS (normal) Occurs early in pregnancy Occurs late, and 30% postpartum (TTP occurrence is even throughout preg) Renal symptoms Helps distinguish HELLP from TTP (but bad HELLP can cause ARF)
 Normal antithrombin III. Helps distinguish HELLP (low) from TTP, HUS (normal) Occurs early in pregnancy. Occurs late, and 30% postpartum (TTP occurrence is even throughout preg) Renal symptoms. Helps distinguish HELLP from TTP (but bad HELLP can cause ARF)")
66
Preeclampsia Proteinuria > 300 mg in 24 hours +/- edema
Hypertension (140/90 or 30/15 over baseline) Presents as headache, blurry vision, CNS changes, or just HTN After 20 weeks, unless molar pregnancy Risk Factors: Primagravids and grand-multiparous DM Age Obesity
 Presents as headache, blurry vision, CNS changes, or just HTN. After 20 weeks, unless molar pregnancy. Risk Factors: Primagravids and grand-multiparous. DM. Age. Obesity.")
67
HELLP Syndrome Hemolysis, Elevated Liver enzymes, Low Platelets
Variant of pre-eclampsia May present as epigastric/RUQ pain Hemolysis: schistocytes on peripheral smear Abnormal coagulation profile

68
Eclampsia Pre-eclampsia + seizure: eclampsia
Headache, CNS, visual changes, hyperreflexia Worse w/poor prenatal care, DM, obesity Rx: magnesium sulfate, hydralazine Definitive treatment is DELIVERY Not the same as primary hypertension: more like withdrawl htn, pheo. Don’t use typical drugs! Beta-blocker contraindicated: “unopposed alpha stimulation”

69
Ectopic Pregnancy Leading cause of first trimester maternal death
2nd in $$ for claims against EM docs Risk factors: Anything that mucks up your tubes PID previous ectopic IUD tubal surgery Infertility treatment ?Unilateral, ?intermittent pain (95%) bleeding (80%, not constant) 5-8 wks after LMP
 bleeding (80%, not constant) 5-8 wks after LMP.")
70
Ectopic Pregnancy Region: distal ampulla of fallopian tube (90%)
Need positive hcg Then do ultrasound

71
Ectopic workup Indicators of IUP, all should be visible on TV by 5-6 weeks: yolk sac fetal heart fetal pole Heterotopics: 1:30,000 (but 5x higher if on fertility treatment) If not IUP Too early Ectopic Abnormal IUP Get quant hcg. If above discrim zone ( , depending on ref), call gyn. If lower, may be too early. You don’t know what you have. Call gyn, will likely go home to f/u in 2 days for serial HCG.
 If not IUP. Too early. Ectopic. Abnormal IUP. Get quant hcg. If above discrim zone ( , depending on ref), call gyn. If lower, may be too early. You don’t know what you have. Call gyn, will likely go home to f/u in 2 days for serial HCG.")
72
Ectopic, cont. Happen at around 4-5 wks
Culdocentesis: rarely used. The positive is NON CLOTTING BLOOD Indication for methotrexate: in stable ectopics/no fluid in belly. If they’ve started to leak, don’t use MTX. Failure rate 5-10% Our job is mostly stabilization, coordination.

74
RhoGAM If they’re Rh Negative, give it
Passive antibody if mother RH negative and any mixing of blood between circulations (vag bleeding, trauma) 50 mcg if <12wks, 300mcg if >12 weeks Test for mixing: Kleinhauer Betke: look for nucleated RBC (of fetus) in maternal blood
 50 mcg if <12wks, 300mcg if >12 weeks. Test for mixing: Kleinhauer Betke: look for nucleated RBC (of fetus) in maternal blood.")
75
Third trimester bleeding
Placental abruption: normal placenta (in fundus, near head), painful bleeding. Takes a while to ooze out: painful, darker color. Ultrasound CAN’T always diagnosis this Risk factors: HTN, older, multitip, smoke, cocaine Previa: painless, bright red. Ultrasound always helpful Don’t do pelvic exam in this situation Admit, stabilize, RhoGAM if Rh-Neg, C-section if remains unstable
, painful bleeding. Takes a while to ooze out: painful, darker color. Ultrasound CAN’T always diagnosis this. Risk factors: HTN, older, multitip, smoke, cocaine. Previa: painless, bright red. Ultrasound always helpful. Don’t do pelvic exam in this situation. Admit, stabilize, RhoGAM if Rh-Neg, C-section if remains unstable.")
77
Question 13 A 30 year old woman presents complaining of a ‘typical’ migraine. She is 4 weeks post-partum and currently breastfeeding. Which of the following medications is contraindicated? Thank goodness this isn’t a question on HELLP, IIH/pseudotumor, SAH, where they’d be asking about optimal imaging… Acetaminophen Safe in pregnancy (B) and breastfeeding (“Safe”) Caffeine Safe in pregnancy (C?) and breastfeeding (“N/A”) Ergotamine Passes through milk, causes v/d and seizures in infants. Morphine Passes through milk at 1% of maternal dose, no adverse affects reported Promethazine Phenergan is C: Safe in pregnancy, “potentially unsafe” in breastfeeding
 and breastfeeding ( Safe ) Caffeine. Safe in pregnancy (C ) and breastfeeding ( N/A ) Ergotamine. Passes through milk, causes v/d and seizures in infants. Morphine. Passes through milk at 1% of maternal dose, no adverse affects reported. Promethazine. Phenergan is C: Safe in pregnancy, potentially unsafe in breastfeeding.")
78
Safe drugs in pregnancy
FDA ranked A,B,C,D,X (low risk→high risk) Most asthma meds (steroids, albuterol, etc.) HTN: beta blockers, calcium channel blockers Heparin (not warfarin) Killed vaccines (tetanus) Antibiotics: PCN, cephalosporins, clinda, INH, ethambutol
 Most asthma meds (steroids, albuterol, etc.) HTN: beta blockers, calcium channel blockers. Heparin (not warfarin) Killed vaccines (tetanus) Antibiotics: PCN, cephalosporins, clinda, INH, ethambutol.")
79
Safe drugs in pregnancy
Meds in pregnancy: Almost nothing is category A (RCT shows no risk) Localize, topicalize if you can. Congestion meds: all C Antipyretics: Mostly B at first, D for third term Antiemetics: Doxylamine is A, ‘trons are B, all else C Antibiotics: Pen, Cephalos, Azithro, Vanc: B Analgesics: Oxycodone, Hydrocodone = B. Codeine C.
 Localize, topicalize if you can. Congestion meds: all C. Antipyretics: Mostly B at first, D for third term. Antiemetics: Doxylamine is A, ‘trons are B, all else C. Antibiotics: Pen, Cephalos, Azithro, Vanc: B. Analgesics: Oxycodone, Hydrocodone = B. Codeine C.")
81
Question 14 A 20 year old woman presents by ambulance. EMS reports she just had a seizure. She is 7 months pregnant and has not had any prenatal care – her mother called 911 because she “wasn’t acting right.” On arrival, vital signs are 171/90, HR 90, RR 13, sat 99% on O2. She is unarousable. Management should include: Lorazepam 1 mg IV Class D and not indicated for eclampsia (if pt had SE with hx of szs, sure…) Magnesium 6g IV over 20 minutes IV beats IM. Keep levels between 4-7 mg/dL. Drip at 2g/hr. Check reflexes. Nifedipine 10 mg PO Magnesium won’t control BP, but an oral agent has no role here. Phenobarbital 1g IV Class B but not the solution here. Phenytoin 1g IV over 25 minutes Class D and not indicated for eclampsia.
 Magnesium 6g IV over 20 minutes. IV beats IM. Keep levels between 4-7 mg/dL. Drip at 2g/hr. Check reflexes. Nifedipine 10 mg PO. Magnesium won’t control BP, but an oral agent has no role here. Phenobarbital 1g IV. Class B but not the solution here. Phenytoin 1g IV over 25 minutes. Class D and not indicated for eclampsia.")
82
Safe drugs in pregnancy
Midazolam, Diazepam are D Haldol, Droperidol are D Pentobarb, Ketamine are B Lidocaine, Propofol are B. ACE-I, ARBS are X or D. Hydralazine is only C, fenoldepam, esmolol are B. Ethanol, Phenytoin, Valproate, Tetracycline all D. Quinolones C.

83
Trauma in Pregnancy Initial trauma care same as non-pregnant
Causes of fetal death: #1 maternal death, #2 abruption Remember RhoGAM No radiologic test should be withheld for appropriate maternal evaluation

84
Trauma in Pregnancy Fetal monitoring >20 weeks
Minimum of four hours Signs of fetal distress > 8 contractions/hour suggest abruption Kleihauer-Betke test (fetal-maternal hemorrhage) For hypotension—turn pt to left side (to displace uterus off IVC), fluid bolus Maternal stabilization is the most important factor in determining fetal survival
 For hypotension—turn pt to left side (to displace uterus off IVC), fluid bolus. Maternal stabilization is the most important factor in determining fetal survival.")
85
Safe imaging in pregnancy
Diagnostic Radiology in pregnancy: If it’s indicated, do it. D-dimer has no defined norms, just rises. Helpful if negative… Rad Threshold is 50 mSv. ?Others say fetus = 10. CXR = 0.02 mSv. CTAngio = 5-30… if it’s indicated, do it. Weeks 2-8: Organogenesis. Rads teratogen Weeks 8-15: Neuro development at risk Weeks 15+ … much less risk

86
Pre-term Labor Labor at 20-35 weeks Sterile speculum
Risk factors: multiple births, DES, cocaine, PIH, abruptio, alcohol, smoking Admit, IV Fluids, bed rest, tocolytics (mag, terbutaline … you won’t be giving…)
")
87
Premature Rupture of Membranes (PROM)
Rupture >20 weeks and prior to labor Nitrazine test: blue (positive) Sterile speculum exam: ferning (due to high quantity of salts in amniotic fluid) Avoid bimanual Risks: Infection, premature labor, prolapsed cord Admit them, they’re not going. Start monitoring in the ED, consider tocolytics.
 Sterile speculum exam: ferning (due to high quantity of salts in amniotic fluid) Avoid bimanual. Risks: Infection, premature labor, prolapsed cord. Admit them, they’re not going. Start monitoring in the ED, consider tocolytics.")
88
Umbilical Cord Prolapse
Seen in up to 8%, but perinatal mortality: 50% Pulsating cord on exam Put patient in knee to chest position Emergent c-section Stop the delivery, elevate the presenting part, Trendelenburg can help, but call GYN

90
Amniotic Fluid Embolism
2nd/3rd Trimester Immune response to amniotic fluid in circulation First described in More like anaphylaxis? Shock, bleeding, dyspnea, hypoxia, coagulopathy Mortality = 50% at 1 hour, 80% at 4-5 hours All we can really do is pressors, FFP, maybe HD, emergency C-section

91
Fetal Distress Fetal hypoxia and/or acidosis
Late decels (early decels expected with contractions) Severe variable decels are concerning Decreased variation is concerning Treatment: left lateral position, oxygen, IV fluids, consider delivery (emergency C-section)
 Severe variable decels are concerning. Decreased variation is concerning. Treatment: left lateral position, oxygen, IV fluids, consider delivery (emergency C-section)")
92
Late Decelerations

93
Delivery Ask yourself: What is GA? (betamethasone if < 34 weeks)
How many feti? Meconium + resp depression ET intubation History of maternal drug use? Consider narcan 8 stages: Head out by stage 3-4, then anterior shoulder, then posterior shoulder Wait 30 min for placenta, pull gently, check it

94
Dystocia Difficult labor Abnormal fetal presention
Cephalopevlic disproportion Gestational diabetes Treatment: Fetal manipulation (could cause brachial plexopathy) Suprapubic pressure Generous episiotomy
 Suprapubic pressure. Generous episiotomy.")
95
APGAR Score Indicator of neonatal depression Measured at 1 and 5 min
Appearance (color), Pulse, Grimace (reflex), Activity (tone), Respiration Score 0-2 each
, Pulse, Grimace (reflex), Activity (tone), Respiration. Score 0-2 each.")
96
Emergency C-section Maternal cardiopulmonary arrest
Indicators of fetal survival Cause of maternal death Quality of CPR Gestational Age (>23 weeks) Arrest to delivery time (after 20 minutes, survival is unlikely) Vertical abdominal and uterine incision
 Arrest to delivery time (after 20 minutes, survival is unlikely) Vertical abdominal and uterine incision.")
98
Question 15 Which of the following is the least likely risk factor for postpartum endometritis? Cesarean delivery C-section is actually the biggest risk factor. Chorioamnionitis Really, any opportunity for bacteria to get into the uterus is a risk factor Many vaginal exams during labor So this is also a risk factor Time since rupture of membranes And this is, too. Urinary tract infection UTI is on the differential, naturally, but no obvious way for bacteria to go from here to uterus… thus, not a risk factor

99
Endometritis Diagnosed by H+P, fever, uterine tenderness
WBC, Cx, sono/CT may support diagnosis Polymicrobial, foul smelling, fever High rate in c-section patients Risks PROM Prolonged labor Chorioamnionitis Multiple exams Internal monitoring devices Treat outpatient with doxy or clinda, with low threshold for admission and IV cephalosporins

100
Mastitis Pain, erythema, swelling Staph infection.
Nurse with other breast, express milk, anti staph treatment (cephalosporin, erythromycin)
")
101
Question 16 A 22 year old woman who is 1 week postpartum and breastfeeding presents complaining of vaginal bleeding more than expected, that started 2 days prior. She says the previous lochia had not been malodorous and had been light red in color. She denies fever or vomit. Vital signs are normal, save for a mild tachycardia. She has minimal abdominal pain. Pelvic shows normal vagina and cervix, no CMT. She is bleeding from the OS. Uterus feels firm and globular. The most likely diagnosis is: Lower genital tract laceration You would see this on exam, and there’d be no bleeding FROM os… Normal menses Not 1 week out, not in a breastfeeder… Retained placenta Many causes of postpartum hemorrhage, this one fits best. Visibile on sono. D+C indicated. Uterine atony Would be boggy or doughy. Most common cause of immediate postpartum hem (ie, 24 hr) Uterine rupture This would present as continued bleeding despite firm tone. More pain and irritation.
 Uterine rupture. This would present as continued bleeding despite firm tone. More pain and irritation.")
102
Postpartum Hemorrhage
Uterine atony Most common cause in first 24 hrs Risks: overdistended uterus, prolonged/precipitous labor, high parity Treatment: fundal massage, oxytocin, IV fluids Ruptured uterus Seen with Previous c-section, excessive pressure, trauma Tachycardia, hypotension, bleeding, absent heart tones Fluid resuscitation, immediate c-section Consider hysterectomy

103
Postpartum Hemorrhage
Retained placenta Early or delayed post-partum hemorrhage Sudden, brisk, painless bleeding Boggy, enlarged uterus Oxytocin, D&C, fluid resuscitation Uterine inversion Excessive traction on umbilical cord OB emergency- IV, 02, tocolytic drugs Do not separate placenta Manual reimplantation or emergent laparatomy Lower genital tract laceration Coagulopathy (von Willebrand)
")
107
Lymphogranuloma Venereum
Organism: Chlamydia trachomatis S/Sxs primary infection: Uncommon in U.S. Primary lesion followed by inguinal buboes Buboes grow and rupture or form firm inguinal masses Rx: Doxycycline

108
Lymphogranuloma Venereum (LGV)
Caused by certain serotypes of Chlamydia 1-3 week incubation (vs days with herpes) BUBOES=painful inguinal nodes Usual scenario: Swollen gland in groin, a little bit sick with it—fevers, chills, myalgias
 BUBOES=painful inguinal nodes. Usual scenario: Swollen gland in groin, a little bit sick with it—fevers, chills, myalgias.")
109
BUBOES

110
LGV No high fevers/non-toxic
Catchphrase: obligate intracellular organism, similar to virus. Doesn’t turn over quickly. Subacute disease process Use doxy or macrolide Since it turns over slowly, should do extended course (21 days) Complications: urethral scarring
 Complications: urethral scarring.")
111
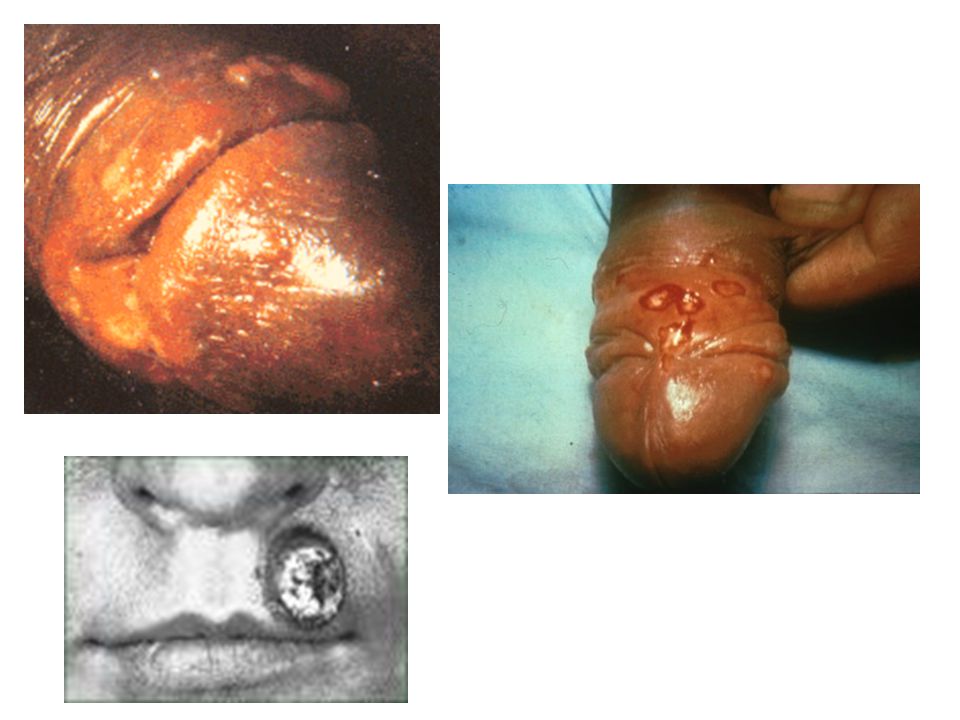
Chancroid Organism: Haemophilus ducreyi S/Sxs primary infection:
Tender painful papule followed by ulceration Multiple lesions may be present, and coalesce Painful inguinal adenopathy in 50% May evolve to buboes and rupture Culture Lesion Rx: azithromycin, ceftriaxone (single dose of both)
")
112
Chancroid Gram negative bacillus: Haemophilus ducreyi
Seen in developing countries Incubates over 2-5 days Vesiculo-pustulo, develops into ulcer

114
+ = CHANCROID

115
Chancroid, continued Painful (Painless: primary syphillis)
Penis picture: must have pain clue! Treatment: macrolide usually not wrong Azithromycin, erythromycin, ceftriaxone

116
Gonococcal Urethritis
Organisms: N. gonorrhea, associated with chlamydial infection (30-50%) S/Sxs: Copious yellow pus Virtually always symptomatic (dysuria) Tests: Gram-neg intracellular diplococci, send GC Consider testing for syphilis Test both partners Rx: Treat for G & C IM Ceftriaxone, or fluoroquinolone, or one-dose cefixime + azithro
 S/Sxs: Copious yellow pus. Virtually always symptomatic (dysuria) Tests: Gram-neg intracellular diplococci, send GC. Consider testing for syphilis. Test both partners. Rx: Treat for G & C. IM Ceftriaxone, or fluoroquinolone, or. one-dose cefixime + azithro.")
117
Non-gonococcal urethritis
Organism: usually Chlamydia (the most common STD) Less commonly Ureaplasma, herpes, trichomonas, candida S/Sxs: Watery discharge, or no discharge No leuks on smear (in 30%) Often asymptomatic Tests: PCR or enzyme immunoassay Rx: 1gm azithromycin once or doxy 100mg BID x 10d
 Less commonly Ureaplasma, herpes, trichomonas, candida. S/Sxs: Watery discharge, or no discharge. No leuks on smear (in 30%) Often asymptomatic. Tests: PCR or enzyme immunoassay. Rx: 1gm azithromycin once or doxy 100mg BID x 10d.")
118
Chlamydia #1 sexually transmitted disease
Major cause of female infertility Symptoms of local disease: Discharge Dysuria Women: cervicitis, urethritis, PID Men: epididymitis, urethritis, proctitis Vag bleeding Asymptomatic 3-20% Rx: azithromycin, doxycycline

120
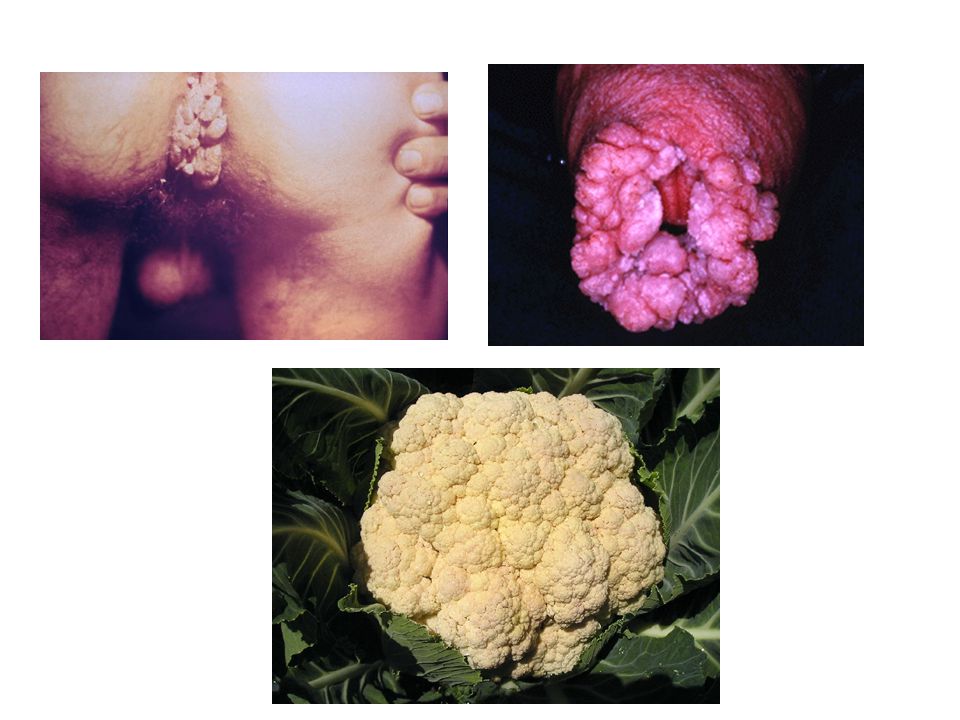
Condyloma Acuminatum (venereal warts)
Human Papilloma Virus 1-3 month incubation Related to cervical carcinoma Soft, vegetative clusters: Think cauliflower/broccoli Transmitted through direct contact

122
Condyloma Acuminatum Don’t get confused with Condyloma lata (syphilis)
Potential question: Patient presents with C.A. what is the next thing to do? (answer: look for other VDs) Treatment: Condylox (podofilox topical) Aldara (imiquimod topical) Cryotherapy
 Treatment: Condylox (podofilox topical) Aldara (imiquimod topical) Cryotherapy.")
123
Herpes Organism: Herpes Simplex (HSV-1 or 2)
S/Sxs of primary infection: Painful pustular or ulcerative lesions Constitutional sxs common (headache, fever, myalgias) Lymphadenopathy (80%) Rx: Acyclovir 200mg 5x/day for 10d
 Lymphadenopathy (80%) Rx: Acyclovir 200mg 5x/day for 10d.")
124
Genital Herpes Type 1: above waist, type 2 below waist
This is not always true, but 60-80% of genital lesions are type 2 All primary infections present like a generalized infection: they have fever/flu/adenopathy Lesions develop at 2-8 days: shallow, painful vesicles

126
HSV, continued Differential dx: mono, primary HIV
Primary infection is worst, infection gets better, then it breaks out from nerves. Relapses associated with stress Tzacnk smears: scraped from BASE of vesicle in epithelial cells. Multinucleate giant cell the key phrase

127
HSV Active at time of birth: need GYN consult
Rx: -cyclovir. Indicated for primary symptoms, immunosuppressed. Also decreases relapse Complications: a good question, not obvious. Young person, febrile, jaundice…not hep virus but herpes! Hepatits, meninigitis, encephalitis, cervical CA, Erythema multiforma also a known rash Urinary retention: invasion of virus into sacral root ganglia. Not from pain. In young women with urinary retention, think herpes!

128
Inclusion body= Chlamydia
HSV The classic picture of herpes lesion: Clustered vesicles on erythemetous base (Hand: herpetic whitlow) Tzank smear confusion: Inclusion body= Chlamydia
 Tzank smear confusion: Inclusion body= Chlamydia.")
129
Gonorrhea… “The clap” Localized disease symptoms:
Discharge pain with urination Cervicitis, urethritis, proctitis, PID Vag bleeding Abdominal/pelvic pain Asymptomatic Rx: single dose therapy Cefixime, ceftriaxone, quinolone

130
Gonorrhea Complications of untreated disease
PID Epidiymitis/orchitis, prostatitis Eye infection Disseminated gonococcal disease Skin lesion: tender pustule on erythemetous base Arthritis/tenosynovitis Endocarditis meningitis

131
Syphillis Organism: Treponema pallidum S/Sxs of Primary Syphilis:
Painless chancre Indurated borders No constitutional sxs Minimal adenopathy Dx: by darkfield microscopy, VDRL, FTA-ABS (to confirm) Rx: 2.4MU benzathine PCN G IM Secondary Syphilis
 Rx: 2.4MU benzathine PCN G IM. Secondary Syphilis.")
132
Syphilis Treponema pallidum (spirochete) 3 different stages Primary
PAINLESS ULCER on penis (chancre) RPR, FTA, VDRL negative in 1st stage Look for the positive dark field Resolves spontaneously Rx: PCN
 RPR, FTA, VDRL negative in 1st stage. Look for the positive dark field. Resolves spontaneously. Rx: PCN.")
133
Secondary syphilis Rash in young health person, not very sick: also think mycoplasma, pittyriasis rosea Low grade fever, not too itchy Palms and soles: others: gonnococcus (pustules), EM, RMSF, allergic reactions/contact dermatitis Condyloma latum Some fever, some painless adenopathy
, EM, RMSF, allergic reactions/contact dermatitis. Condyloma latum. Some fever, some painless adenopathy.")
134
Secondary Syphilis

135
Tertiary syphilis Bites you when you’re an old man, 25 years after primary infection CNS Tabes dorsalis Neuropathy Meningitis Cardiovascular syphilis aortic aneurysm Skin lesions: gummas Benzathine penicillin drug of choice (Long acting penacillin: “LA” by nurses). Strep pharyngitis the only other indication for LA. Second line: docy, erythro, ceftriaxone. Not as good
. Strep pharyngitis the only other indication for LA. Second line: docy, erythro, ceftriaxone. Not as good.")
137
Syphilis Chancre- painless papule- hallmark of primary syphilis
2ndary syphilis 4-10 weeks- macular rash- trunk extremities- palms + soles oral lesions grey painless ulcers Tertiary syphilis-untreated for years- 2 types-neurosyphilis after 10 yrs-meningovascualar vasculitis of vertebral or spinal vessels or tabetic syphilis-demylination and ataxia Cardiovascular only after yrs usually thoracic aorta- aortiv valve insufficiency

138
STI’s Condyloma lata-secondary syphilis- typically-large painless flat topped lesions-typically in anogenital region Condyloma acuminata- genital warts – HPV – pink to grey keritanized with papilliform growths Gonococcal proctitis- tenismus, anal itching and yellow discharge Granuloma inguinale- bacterial infection with Calymmatobacterium granulomatis-painless papules beefy red ulcers with rolled edges Chancroid- Heomophilus Ducreyi- painful genital ulcer-

139
Ovarian cysts Get terminology straight!
Follicular cyst (before egg released), about 3 cm Corpus luteum cyst (after egg released, or pregnant) Nothing bad happens, unless >3 cm…can have torsion, rupture and bleeding!
, about 3 cm. Corpus luteum cyst (after egg released, or pregnant) Nothing bad happens, unless >3 cm…can have torsion, rupture and bleeding!")
140
Ovarinan/Adnexal Torsion
Twists around pedicle Must be tumor or large cyst to do this Dermoid cyst most common Severe unilateral pain, nausea, vomiting Sometimes bleeding, but not impressive Unilateral tenderness Diagnosis: ultrasound, laparoscopy Differential: ectopic, IUP, appendicitis, PID

141
Ovarian tumor Post menopausal Usually advanced stage when diagnosed
2nd most common gyn malignancy Mass on ultrasound Refer

142
Endometriosis Endometrium outside of the uterus
Abdominal pain, cyclical in nature Most commonly on ovary, but can occur anywhere in abdomen, even in lung! Get cyclical pneumothorax Treatment: hormonal therapy

143
Uterine cancer Most common GYN cancer
The case: Old lady with vag bleeding Risk factors Continuous estrogen Obesity Diabetes Hypertension, nulliparity Late menopause Pap smears don’t work for this Refer to gyn

144
Uterine prolapse Herniation into vagina
Post menopausal, multiparous women Think they have alien in their vagina ED Rx: reduce it! f/u gyn for possible surgery

145
Dysfunctional Uterine Bleeding
Think of anovulatory cycles due to hormonal imbalances. Most with starting periods (menarche), stopping (menopause) Consider cancer Cycle with hormones, D&C
, stopping (menopause) Consider cancer. Cycle with hormones, D&C.")
146
Sexual assault/ Post-exposure prophylaxis
You have to consider it in every case, but not necessarily do it in every case Plan B (levonorgestrel): give 1 dose now, then another in 12hrs Not 100% effective, gets less effective with more time from assault Works up to 3 days after sexual activity Nausea and vomiting common Consider in SA
: give 1 dose now, then another in 12hrs. Not 100% effective, gets less effective with more time from assault. Works up to 3 days after sexual activity. Nausea and vomiting common. Consider in SA.")
147
SA considerations Check for preg: underlying pregnancy
HIV test: same as above Syphilis serology 3 ways to tell if there was intercourse with ejaculation: Acid phosphatase (in seminal fluid) P30 (seminal marker) Looking for motile sperm
 P30 (seminal marker) Looking for motile sperm.")
Similar presentations







































>")