Download presentation
Presentation is loading. Please wait.

2
STRABISMUS: IS IT ‘STRABISMIC’ ? …. NEUROLOGICAL? OR BOTH?
LIONEL KOWAL DIRECTOR, OCULAR MOTILITY CLINIC, RVEEH SENIOR CLINICAL FELLOW, DEPT OPHTHALMOLOGY, UNIVERSITY OF MELBOURNE FIRST VICE PRESIDENT, INTERNATIONAL STRABISMOLOGICAL ASSOCIATION,

3
OVERVIEW…. OF THE CAUSES, ASSOCIATIONS AND TYPES OF STRABISMUS
IDENTIFYING SOME COMMON / UNDER- RECOGNISED ASSOCIATIONS

4
STRABISMUS Any ocular misalignment INCLUDES:
Abnormalities of development of acuity Abnormalities of development of binocularity The variants of congenital nystagmus

5
CHILDHOOD STRABISMUS 1. Derive largely from refractive disorders
2. Pure neurological 3. Derive largely from abnormal early visual devpt 4. Special types

6
STRABISMUS: END RESULT OF A COMPLEX JIGSAW PUZZLE
Abnormalities in one / more of… Sensory development Refraction Orbital anatomy EOM anatomy / physiology Cortical / supranuclear Accommodation / convergence either cause or are caused by strabismus

7
COMPLEX JIGSAW PUZZLE Abnormal Sensory development
Amblyopia Suppression Abnormal retinal correspondence

8
COMPLEX JIGSAW PUZZLE Abnormal Refraction
Hyperopia or ‘plus’ error * Causes esotropia Any asymmetric refractive error Causes amblyopia, esotropia if + *so-called ‘long sighted’ - NOT the mirror image of short sighted. The patient can see clearly by generating focusing effort = accommodation

9
COMPLEX JIGSAW PUZZLE Abnormal orbital anatomy1
Orbital pulley heterotopy Changes muscle actions Globe size distorting muscle cone Causes pseudo- 6th Shallow / deep orbit Shallow: more prone to exotropia

10
COMPLEX JIGSAW PUZZLE Abnormal orbital anatomy 2
Intorted / extorted orbit More prone to alphabet patterns Plagiocephaly More prone to oblique dysfunction

11
COMPLEX JIGSAW PUZZLE Abnormal EOM anatomy / physiology
Oblique muscle dysfunction Abnormal elevation / depression in AB- or AD- duction Globe torsion Abnormal innervation [Duane's, CFEOM] Strange incomitant strabismus

12
COMPLEX JIGSAW PUZZLE Abnormal cortical / supranuclear substrate 1
motor fusion oculomotor ‘shock absorber’ / ‘glue’ that tries to keep eyes straight sensory fusion stereopsis Abnormal binocular columns

13
COMPLEX JIGSAW PUZZLE Abnormal cortical / supranuclear substrate 2
Abnormal interneurons Latent Manifest Latent Nystagmus = LMLN = Fixation Maldevelopment N Just about any cause / association of devptl delay Chiari PVL

14
COMPLEX JIGSAW PUZZLE Abnormal Accom - Conv relationship
Accom too much convergence Conv too much accommodation *too little is rarely a problem

15
1. Derives from refractive disorders
TYPES OF STRABISMUS 1. Derives from refractive disorders 2. Pure neurological 3. Derives from abn early visual devpt 4. Special types

16
NORMAL ACCOMMODATION Accommodation and convergence = Focus and Aim
are very tightly linked

17
ACCOMMODATIVE / ‘OPTOMETRIC’ ESOTROPIA
+4 : Abn degree of accommodation required to see clearly Abn amount of accomm convergence is generated competes against motor fusion [oculomotor shock absorber]

18
WHAT DOES +4 MEAN? For distance, generates same accommodation that ‘perfect’ person generates when looking 1/4 m away. For distance fixation, eyes will tend to a point 25cm away When an object 25cm away, eyes will a point 12 cm away

19
ACCOMMODATIVE / ‘OPTOMETRIC’ ESOTROPIA
Exactly the same can happen with low + and abnormal accomm - convergence relationship* Many of these bifocals *many synonyms - convergence Xs, high AC/A ratio

20
Developing an esotropia…
Prolonged accommodation tendency to inappropriate convergence and increased tone in medial recti Increased tone will eventually exceed motor fusional reserve and esotropia! Initially reversible with glasses Eventually the medial rectus shortens so much that only botox or surgery will work Glasses still required to prevent recurrence [and, when older, for clear vision]

21
Accommodative esotropia
Usually 2-5 yrs old Usually high + [thick magnifying lenses] Sometimes low / normal + with abnormal relation b/w accomm and convergence Background of normal visual devpt in first 6mo of life

22
Developing an esotropia…
Happens more readily * if motor fusion is impaired: chromosomal defect / devptl delay Amblyopia Orbital anomaly LMLN * younger, lower +

23
‘Breakdown of pre- existing phoria…’
Only acceptable as a presumptive label if: Wears thick magnifying lenses ± amblyopia Accomm disturbed e.g. Ditropan

24
2. Pure neurological TYPES OF STRABISMUS
1. Derives from refractive disorders 2. Pure neurological 3. Derives from abn early visual devpt 4. Special types

25
‘Pure’ neurological strabismus
True cong sup obl palsy 6th CFEOM [hypoplasia sup div 3rd; KIF mutation] ..have 2ary effects that are dependent on age of onset and associated factors such as refraction

26
R SOP HEAD TILT TO LEFT

27
R IO OA R SO UA TIGHT RSR RIR ‘UA’

28
True sup obl palsy LSO OK RSO ?absent

29
REAL CONG R SOP & CONG ET FIXING WITH PARETIC R EYE

30
R SO atrophic

31
Fake SOP Conditions that simulate SOP False +ve diagnostic rate ?50%
Abnormal cyclovertical anatomy Craniofacial anomalies Posteroplaced trochlea [Bagolini] Fink : 20% of SO and IO have > 30 degrees asymmetry in course Demer: orbital pulley displacements Abnormal physiology Brodsky’s wild pitch

32
3. Derives from abnormal early visual development
TYPES OF STRABISMUS 1. Derives from refractive disorders 2. Pure neurological 3. Derives from abnormal early visual development 4. Special types

33
1. Abnormal symmetric acuity devpt ‘Congenital Nystagmus’ * = CN
Bilateral bad refractive error Albinism : optic n dysplasia, foveal hypoplasia Bil optic n hypoplasia Bil cataracts CN degrades vision further * aka Idiopathic Infantile N, Cong motor N, Cong Sensory N,…

34
‘Congenital Nystagmus’ = CN
Pendular / jerk Greater on lateral gaze UNIQUE : CONVERGENCE NULL Face turns Pathognomonic waveform

35
CN: face turn null & convergence null
Null zone on R gaze drives face turn / tilt to L N to L when L of null N to R when R of null

36
Convergence null : unique to CN

37
Abnormal binocularity devpt Latent Manifest Latent N *
Caused by… Any strabismus Asymmetric refraction Monocular vision reducing pathology - cataract, optic n hypo,…. * aka Fixation Maldevelopment N

38
Abnormal binocularity devpt Latent Manifest Latent N
Jerk Greater on ABduction UNIQUE : Fast phase to fixing eye Face turns : RF R face turn, LF L face turn Head tilts : RF R tilt, LF L tilt

39
LMLN VIDEO OF POST OP LMLN; NOW ‘PURE’ LN
Esophoria after Exotropia surgery N to fixing eye

40
LMLN : N fixing eye Fast phase to fixing eye

41
LMLN COMMONLY CONGENITAL ESOTROPIA but can cause / be associated with other strabismus Also CAUSES DISSOCIATED H & V DEVIATIONS

42
CONGENITAL ESOTROPIA

43
ASSOCIATIONS OF LMLN & Congenital ET
Down’s 30% Severe neonatal course IVH /HC near 100% PVL

44
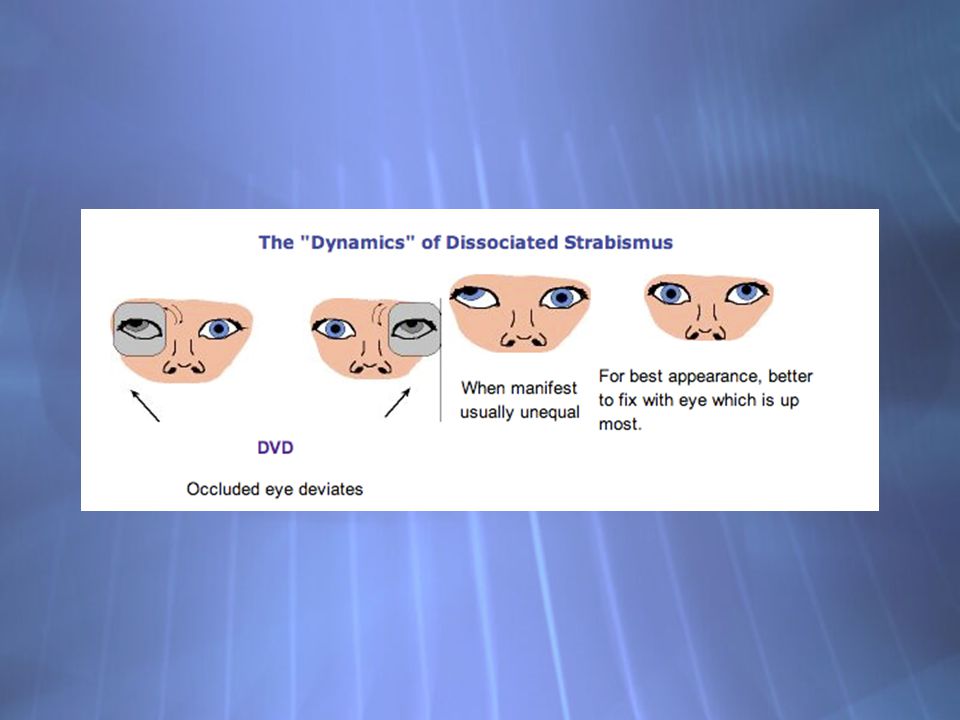
VERTICALS IN CONG STRAB : DVD Dissociated Vertical Deviation
Common pattern: Right fixation: L L fixation: R Contralateral DVD is the end result of ‘braking’ the torsional component of LMLN in the fixing eye to try and improve acuity

45
VERTICALS IN CET : DVD RE fixing LE

47
CONGENITAL STRABISMUS
Head turns / face tilts are common Caused by attempts to minimise blur effect of the LMLN

48
Alternating Face Turn L Fixation : L Face Turn
R Fixation : R Face Turn Ciancia’s syndrome: preference for fixation in adduction because recruiting medial rectus ‘brakes’ horizontal component of LMLN improved vision Alternating face turn has 2 causes. One is the H version of ciancia’s syndrome -If the L wants to see more clearly, then the H component of LMLN has to be lessened and this is done by recruiting the LMR, and the best way to do this is to adopt a L face turn,

49
Special case: Head tilt to fixing eye
LF drives HT to L RF : no HT Caused by Torsional LMLN Here we have L tilt driven by L fixation. With RE fixation, there is no tilt. The Usual cause of this situation is a type of congenital nystagmus with the awkward name of LMLN. This is usually H, but may have a T component as well. This is described well in the ISA Vancouver meeting proceedings.

50
LF drives HT to L Torsional LMLN
LMLN is the cong nystag seen with disorders of binocular development [?always] Seen in cong ET = Fixation Maldevelopment N. Usually has H component, sometimes T as well Fine torsional N on slit lamp N degrades vision - vision improves when N blocked This type of N [like any type of N] degrades vision. Vision improves when the N is blocked. You can often see this N on the slit lamp. LMLN is seen in all cases of cong ET, tho’ not all cases of cong ET have the torsional type.

51
Special case: Alternating Head Tilt
LF drives L tilt RF drives R tilt = Ciancia’s syndrome If LF drives head tilt to L and RF drives head tilt to the R, this is the same mechanism - a need to see more clearly generates a need to suppress the T component of the N. A head tilt recruits SO which acts as a brake on the N and allows clearer vision.

52
Recap…Abnormal binocularity devpt Latent Manifest Latent N
Features of this type of strab recognised by the accompaniments. LMLN, + one/ more of… Head tilt / face turn to fixing eye DVDs Large angle esotropia

53
‘Ophthalmic’ PVL Optic n hypoplasia uni-/bi-
Cognitive visual problems - normal acuity Reduced acuity LMLN CN

54
THINGS THAT LOOK LIKE ‘STRABISMIC’ STRABISMUS
CHIARI – later onset ‘deterioration of old latent strabismus ‘ – there always has to be a credible background / predisposition. And a reason for breakdown

55
THINGS THAT LOOK LIKE ‘STRABISMIC’ STRABISMUS
Autoimmune neuropathies Myesthenia

56
Strabismus syndromes Duane’s Brown’s

57
Brown’s Tight superior oblique tendon Restricted elevation in aDuction

58
Duane’s Retraction on adduction
Retraction R on L gaze Restricted aDduction R Restricted aBduction L Co-firing Lateral rectus on aDuction

59
Duane’s Retraction L on R gaze Restricted aDduction L
Co-firing lateral rectus on aDuction

60
THANK YOU

Similar presentations









 Journal of American Association for Peadiatric Ophthalmology and strabismus 2008.>")
 may turn in, out, up, or down can be present in one or both eyes cross-eyed, squint. Vergence Duction.>")








