Download presentation
Presentation is loading. Please wait.

1
Introduction to EVIDENCE-BASED MEDICINE
DEPARTMENT OF FAMILY & COMMUNITY MEDICINE UP-Philippine General Hospital

2
WHAT IS EVIDENCE BASED MEDICINE?
The conscientious, explicit, judicious use of current best evidence in making decisions about the care of individual patient. It means integrating individual clinical expertise with the best available external clinical evidence from systematic research. Thus Evidence based medicine evolved. According to Dr. David Sackett in 1996… Dr. David Sackett, 1996

4
EVIDENCE-BASED MEDICINE

5
STEPS IN EBM PROCESS The patient
1. Start with the patient – a clinical problem or question arises out of the care of the patient The question 2. Construct a well built clincial question from the case The resource 3. Select the appropriate resource(s) and conduct the search The evaluation 4. Appraise the evidence for its validity and applicability 5. Return to the patient – intergrate the evidence with the clinical expertise, patient preference and apply it to practice Self evaluation 6. Evaluate your performance with this patient
 and conduct the search. The evaluation. 4. Appraise the evidence for its validity and applicability. 5. Return to the patient – intergrate the evidence with the clinical expertise, patient preference and apply it to practice. Self evaluation. 6. Evaluate your performance with this patient.")
6
STEP 1: CLINICAL SCENARIO
Maria, a 67 year old History of congestive heart failure brought on by several myocardial infarctions. Hospitalized 2x in the last 6 months for worsening of heart failure Remember: EBM always start and ends with the patient Duke University Medical Center and Health Sciences Library, 2006

7
STEP 1: CLINICAL SCENARIO
Presently in normal sinus rhythm She is extremely compliant about taking her medications (enalapril, aspirin and simvastatin) She desperately wants to stay out of the hospital You think she should also be taking digoxin, but you are not certain if this will help keep her out of the hospital. You decide to research this question before her next visit. Duke University Medical Center and Health Sciences Library, 2006
 She desperately wants to stay out of the hospital. You think she should also be taking digoxin, but you are not certain if this will help keep her out of the hospital. You decide to research this question before her next visit. Duke University Medical Center and Health Sciences Library,")
8
STEP 2. CONSTRUCT A WELL BUILT CLINICAL QUESTION
ANATOMY OF A CLINICAL QUESTION POPULATION primary problem, disease, or co-existing conditions sex, age or race of a patient INTERVENTION OR TREATMENT main intervention, prognostic factor, or exposure prescribe a drug, Order a test? Order surgery? COMPARISON OR CONTROL main alternative to compare with the intervention Another drug? Another test? Placebo? Your clinical question does not always need a specific comparison OUTCOME What do you hope to accomplish/measure/improve/affect? What are you trying to do for the patient? Symptoms? Number of adverse events? Functionality? Test scores? METHODOLOGY Type of Evidence/Study Anatomy of a good clinical question 1. Patient or problem How would you describe a group of patients similar to yours? What are the most important characteristics of the patient? This may include the primary problem, disease, or co-existing conditions. Sometimes the sex, age or race of a patient might be relevant to the diagnosis or treatment of a disease. 2. Intervention, prognostic factor, or exposure Which main intervention, prognostic factor, or exposure are you considering? What do you want to do for the patient? Prescribe a drug? Order a test? Order surgery? What factor may influence the prognosis of the patient? Age? Co-existing problems? What was the patient exposed to? Asbestos? Cigarette smoke? 3. Comparison What is the main alternative to compare with the intervention? Are you trying to decide between two drugs, a drug and no medication or placebo, or two diagnostic tests? Your clinical question does not always need a specific comparison. 4. Outcomes What can you hope to accomplish, measure, improve or affect? What are you trying to do for the patient? Relieve or eliminate the symptoms? Reduce the number of adverse events? Improve function or test scores?

9
GOING BACK TO MARIA Patient / Problem
Elderly with congestive heart failure Intervention Digoxin Comparison Placebo Outcome Primary: reduce number of hospitalizations Secondary: reduce mortality Methodology Randomized Controlled Trial A placebo looks and taste exactly the same as drug in question but without the active ingredient.

10
Meta-analysis This pyramid shows the strength of evidences.

11
TYPE OF QUESTION: WHAT TYPE OF STUDY?
Suggested best type of Study Therapy RCT>cohort > case control > case series Diagnosis Cross sectional>prospective, blind comparison to a gold standard Etiology/Harm RCT > cohort > case control > case series Prognosis cohort study > case control > case series Prevention RCT>cohort study > case control > case series Cost economic analysis What type of study is best suited for Maria’s case?

12
STEP 3: SELECT THE APPROPRIATE RESOURCE AND CONDUCT THE SEARCH
SEARCH STRATEGIES Identify the concepts: KEY TERMS Phrase search: “quotation marks” Boolean Principle: OR, AND MeSH Truncation and Wild Card Limits Related Articles Clinical Queries A well-built clinical question can lead directly to a well-built search strategy. Key Terms: prioritize Phrase Search Boolean Principle: Use of OR to broaden your search Use of AND to limit your search MeSH: Medical Subject Heading: limit your search Truncation and Wild Card: broaden your search Limits Related Articles Clinical Queries

13
BOOLEAN PRINCIPLE By using OR & AND… How do we get A? B? C? D? A D B C
Congestive Heart Failure Digoxin By using OR & AND… How do we get A? B? C? D? A Hosptialization D B C

14
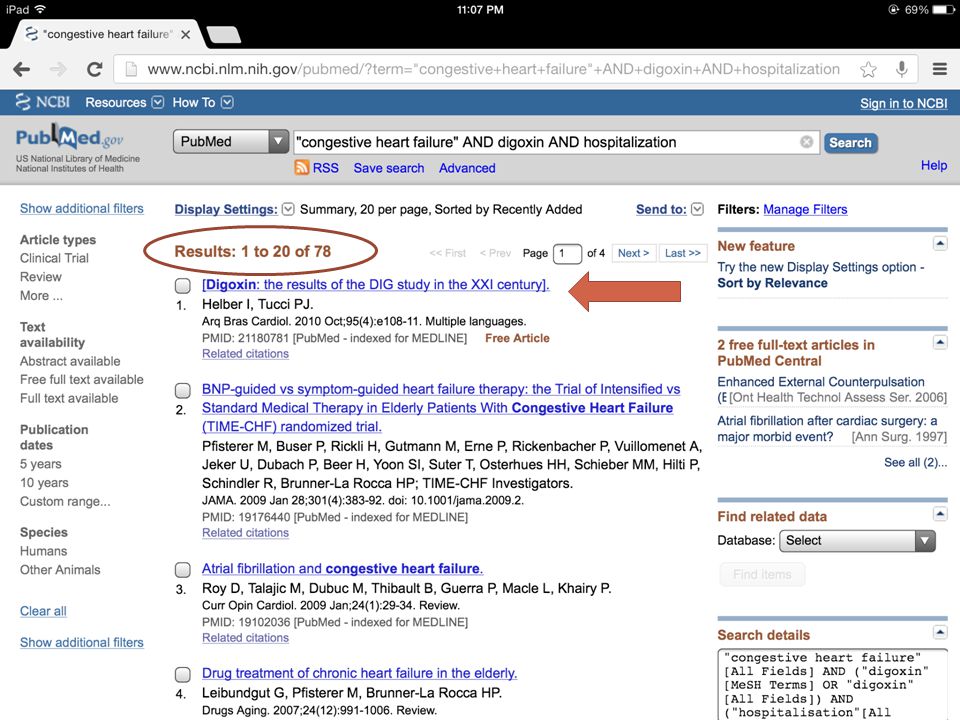
TOTAL: 31, 416 Use of Key Terms and Phrase Search. What is the purpose of using quotation marks?

15
TOTAL: 151, 951 We can also use multiple search terms. Going back to our PICOM, what search terms can we use?

19
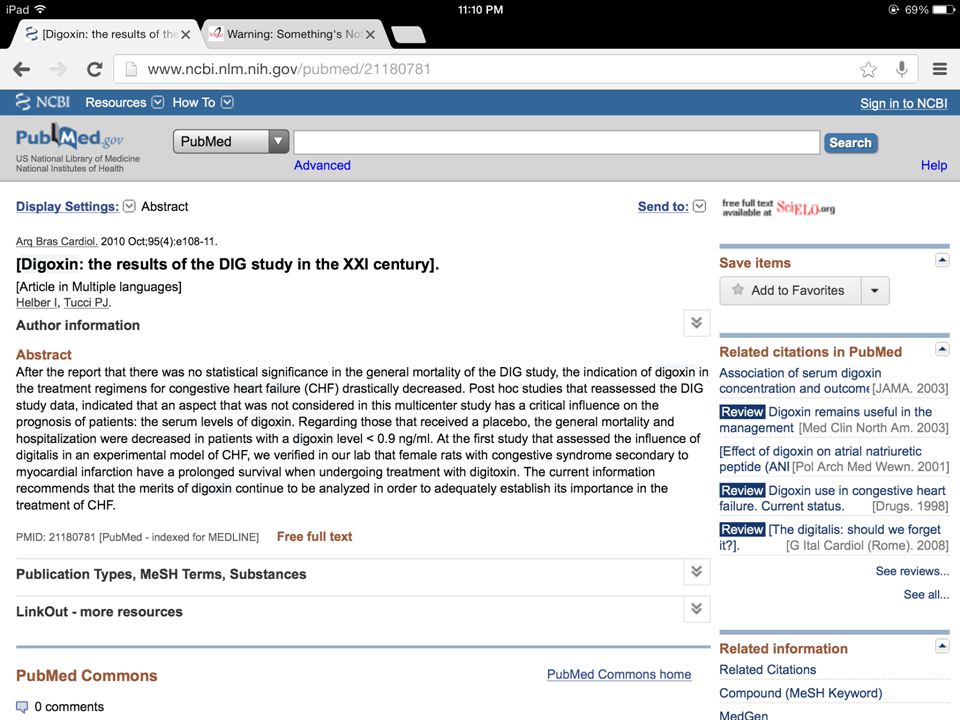
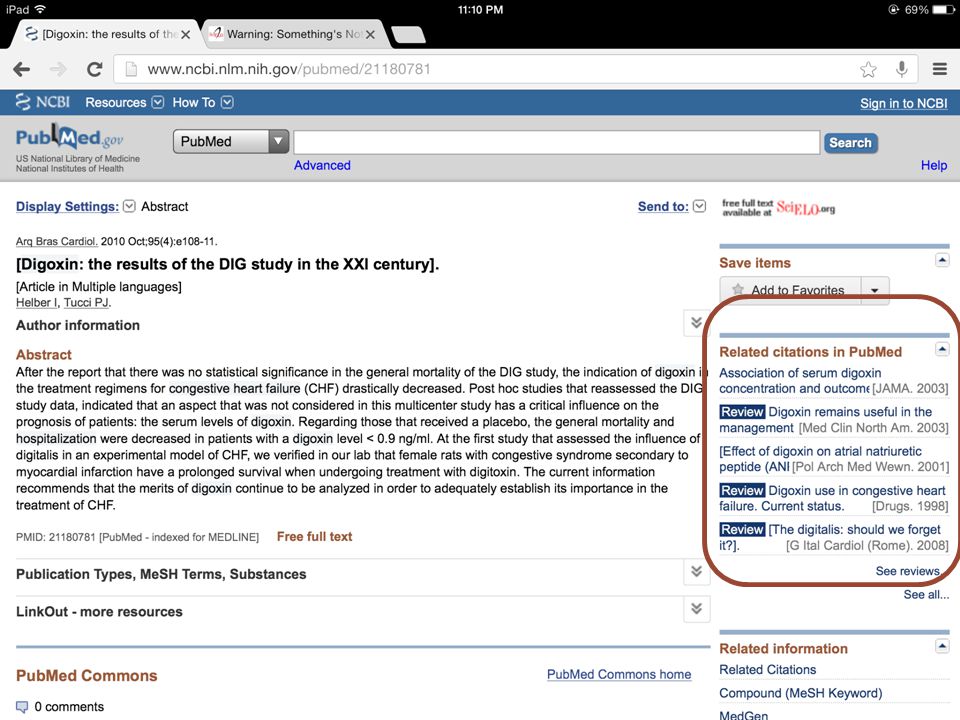
Search for Related Literature.

21
What is MeSH? What does it do?

22
PubMed Articles: 76,707

23
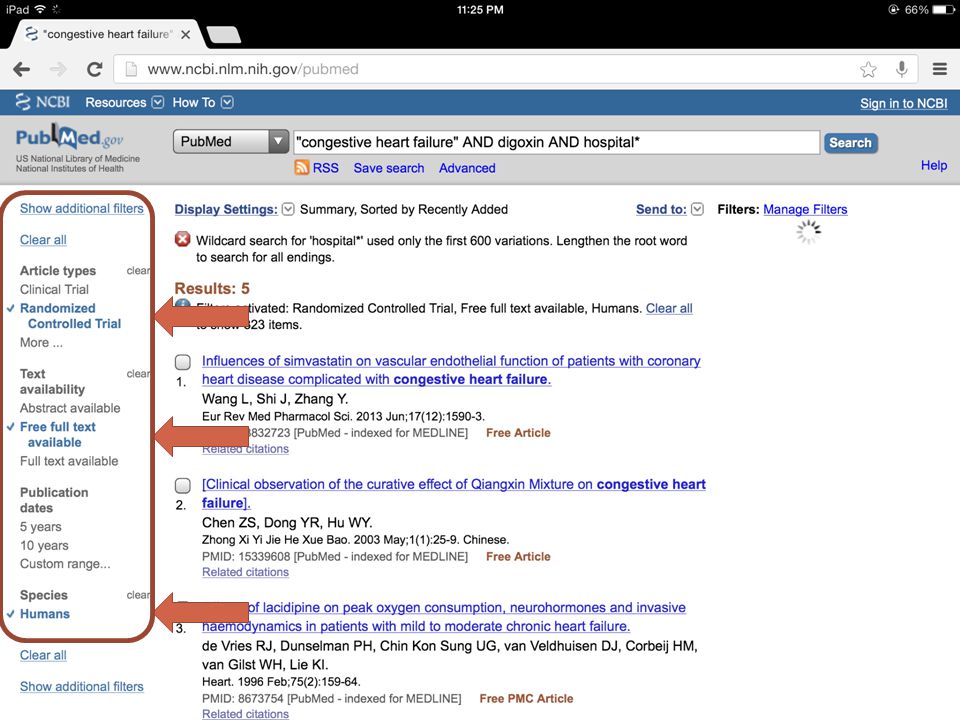
Example of truncation or wild card
Example of truncation or wild card. This search will bring out words such as hospital, hospitalization, hospitality, etc. You will used this strategy in dire times.

25
OTHER WEBSITES National Guideline Clearinghouse
The Cochrane Collaboration New England Journal of Medicine Specialty Journals

26
Once you find an article, What will you do with it?

27
Do the Critical Appraisal!
USE The Evidence-Based Family and Community Practice (EBFCP) and Quality Improvement in Health Care Manual (FMRG, 2003) Other source to Understand: Painless EBM by Dr. Dans World Wide Web BUT the guide questions to be answered must come from the EBFCP Manual
 and Quality Improvement in Health Care Manual (FMRG, 2003) Other source to Understand: Painless EBM by Dr. Dans. World Wide Web. BUT the guide questions to be answered must come from the EBFCP Manual.")
28
FORMAT OF JOURNAL REPORT
Case Scenario Research Question Search Title Source Authors Appraisal

29
EVIDENCE-BASED FAMILY AND COMMUNITY PRACTICE
Is it relevant? Is it valid? What are the results? Is it applicable to my patient?

30
Critical Appraisal of An Article on Diagnostics

31
Decision analysis appraisal of an article on diagnostics start with the decision analysis line %(DT) % % % (TT) % Diagnostic Pre-test Treatment Treshold Probability Treshold
 50% 60% 80% (TT) 100% Diagnostic Pre-test Treatment. Treshold Probability Treshold.")
32
Decision Analysis Line
Diagnostic Threshold (DT): arbitrary point at which you rule out the disease below this point After this point, you will request for a diagnostic test Therapeutic Threshold: arbitrary point at which you decide to treat beyond this point Below this point, you will request for a diagnostic test Pre-Test Probability: probability that the patient has the disease Post-Test probability: probability that the patient has the disease after doing the diagnostic exam These are ALL arbitrary points set by the MD.
: arbitrary point at which you rule out the disease below this point. After this point, you will request for a diagnostic test. Therapeutic Threshold: arbitrary point at which you decide to treat beyond this point. Below this point, you will request for a diagnostic test. Pre-Test Probability: probability that the patient has the disease. Post-Test probability: probability that the patient has the disease after doing the diagnostic exam. These are ALL arbitrary points set by the MD.")
33
Case Scenario 24 year old male
Presenting with 1 month history of RUQ pain Started out as epigastric pain then localizing in the RUQ Usually associated with intake of fatty food No other associated symptom PE: (-) Murphy’s What is our pre test probability that this patient has Acute Cholelithiasis? Will we request for an HBT ULTRASOUND?
 Murphy’s. What is our pre test probability that this patient has Acute Cholelithiasis Will we request for an HBT ULTRASOUND")
34
Determine the POST TEST PROBABILITY
APPRAISE SEARCH %(DT) % % (TT) 100% pre-test probability
 60% 90% (TT) 100% pre-test probability.")
35
Is it relevant? Is the objective of the study similar to your clinical dilemma? CLINICAL DILEMMA STUDY Population Intervention and comparative intervention Methodology Outcome ? ? This question is trying to see if you can use the study in your dilemma. If the article is not relevant, maybe you can do another search. Remember, there are valid article that may not be relevant. Validity and relevance are not the same. If the answer is yes to this, proceed.

36
Is it valid? PRIMARY VALIDITY GUIDES
Was there an independent comparison with a reference standard? Did the patient sample include an appropriate spectrum of patients to whom the test will be done? SECONDARY VALIDITY GUIDES Was the reference standard done regardless of the result of the of the diagnostic test being evaluated? Were the methods for performing the test described in sufficient detail to permit replication?

37
PRIMARY VALIDITY GUIDES
1. Was there an independent comparison with a reference standard? Reference standard. Accuracy. Precision. * The reference standard should not be part of the diagnostic procedure in question. A reference standard for a diagnostic test is the test that gives the information nearest to the “truth”. Thus the accuracy of the test should be compared against the standard. If the diagnostic test approximated the standard, that means the test also approximates the “truth”. Thus the first question you should answer is whether there was a comparison with the reference standard and whether the reference standard used is acceptable to your setting.

38
PRIMARY VALIDITY GUIDES
2. Did the patient sample include an appropriate spectrum of patients to whom the test will be done? Inclusion and Exclusion Criteria. Baseline Characteristics (table 1). Representativeness includes subjects with the whole spectrum of the disease The accuracy of a diagnostic test among patients with low risk for the disease is different from patients with high risk for the disease. The accuracy of a diagnostic test among patients with low risk for the disease is different from patients with high risk of the disease. While a test may always distinguish who is healthy and who is very sick, the clinical utility of a test can be seen when used among persons who are healthy, patients who are very sick and those in-between. Patients consulting in family practice usually belong to the healthy and in-between groups.
. Representativeness includes subjects with the whole spectrum of the disease. The accuracy of a diagnostic test among patients with low risk for the disease is different from patients with high risk for the disease. The accuracy of a diagnostic test among patients with low risk for the disease is different from patients with high risk of the disease. While a test may always distinguish who is healthy and who is very sick, the clinical utility of a test can be seen when used among persons who are healthy, patients who are very sick and those in-between. Patients consulting in family practice usually belong to the healthy and in-between groups.")
39
SECONDARY VALIDITY GUIDES
1. Was the reference standard done regardless of the result of the of the diagnostic test being evaluated?

40
SECONDARY VALIDITY GUIDES
2. Were the methods for performing the test described in sufficient detail to permit replication?

41
2. Were the methods for performing the test described in sufficient detail to permit replication?
Look at the results and methodology section. Clear procedure including the preparation of subjects. Diets, drugs to avoid. Precautions. Step by step descriptions. Be able to duplicate the exam in your setting and still get the same results. This is necessary so that the reader will be able to duplicate the test in his/her own setting and get the same result. Description should include preparation for the patient such as diet, drugs to avoid, precautions, ideal conditions for performing the diagnostic test and a step by step description of how the diagnostic test is done and interpreted.

42
II. Overall is the study valid?
If you want to be strict about it, you should answer yes in all 4 questions. A simple rule might be to answer yes to at least, one primary guide and two secondary guides.

43
III. What are the results?
What are the likelihood ratios for the different test results? Likelihood ratios indicates by how much a given test result increases the pre-test probability of the disease. LR of 1 means that the pre-test probability is same after doing the test LR >1 increases the probability that the disease is present

44
Sensitivity & Specificity
Disease Present Absent Positive TP FP Negative FN TN Test SENSITIVITY: probability/likelihood that the diseased patient will test positive: TP / TP + FN Explain the 2x2 table using the formulas. Then remember, when a test has a high Specificity and a patient test Positive, it means you can totally rule IN the disease. If a test has a high SeNsitivity and a patient test Negative, you can totally rule OUT the disease. THUS, good screening test has to have high sensitivity while good confirmatory test high specificity. SPECIFICITY: probability/likelihood that those without the disease will test negative: TN/ TN + FP Remember? SpPIN & SnNOUT

45
LIKELIHOOD RATIO Likelihood ratio of a positive test
Probability that the test is + among diseased person Probability that the test is + among non-diseased person LR (+) = Sensitivity/1-Specificity Likelihood ratio of a negative test Probability that the test is - among diseased person Probability that the test is - among non-diseased person LR (-) = 1-Sensitivity/Specificity Some papers give the sensitivity and specificity values rather than the likelihood ratio.
 = Sensitivity/1-Specificity. Likelihood ratio of a negative test. Probability that the test is - among diseased person. Probability that the test is - among non-diseased person. LR (-) = 1-Sensitivity/Specificity. Some papers give the sensitivity and specificity values rather than the likelihood ratio.")
46
What do Likelihood ratios do?
It can change the probability of the disease after a diagnostic test is done. Remember our Case Scenario %(DT) % % (TT) 100% pre-test probability
 60% 90% (TT) 100% pre-test probability.")
47
Will the likelihood ratios shift the pre-test probability
Use a NOMOGRAM Given a pre test probability of 60% The HBT UTZ yielded a LR of 2.5 PLOT Post test Probability is 93% What does this mean? Our pre test probability is 60% and for example we found a study stating that the LR (+) of an HBT UTZ in detecting gallbladder stone is 5.5, with the use of the nomogram, we can look for the post test probability. It is 93% in this case. Thus, we can request an HBT UTZ for our patient to shift our pre test probability.
 of an HBT UTZ in detecting gallbladder stone is 5.5, with the use of the nomogram, we can look for the post test probability. It is 93% in this case. Thus, we can request an HBT UTZ for our patient to shift our pre test probability.")
48
Determine the POST TEST PROBABILITY
APPRAISE SEARCH This means that a good diagnostic test should shift your pretest probability to a post probability that is above the treatment threshold. If an HTB UTZ will do this, then go ahead and request it for your patient. BUT, if an HBT UTZ won’t shift your probabilities to after the treatment treshold, then look for other diagnostic modalities. %(DT) % % (TT) 100% pre-test probability
 60% 90% (TT) 100% pre-test probability.")
49
IV. Can the results help me in caring for my patients?
Will the reproducibility of the test result and its interpretation be satisfactory in my setting? Is the interpretation simple enough? Is the basis of the interpretation clear and specific? 2. Are the results applicable to my patient? setting is somewhat similar inclusion criteria include characteristics of your patient clinical judgment is required 3. Will the results change my management?

50
Critical appraisal of an article on therapeutics

51
Is it relevant? Is the objective of the study similar to your clinical dilemma? CLINICAL DILEMMA STUDY Population Intervention and comparative intervention Methodology Outcome ? ? This question is trying to see if you can use the study in your dilemma. If the article is not relevant, maybe you can do another search. Remember, there are valid articles that may not be relevant. Validity and relevance are not the same. If the answer is yes to this, proceed. If the answer is no, search for other articles.

52
I. Is it valid? Primary Validity Guides
Was the assignment of patients to treatment randomized? Were all the patient who entered the trial properly accounted for and attributed at its conclusion? Secondary Validity Guides Were patient, their clinicians and study personnel “blinded”? Were the groups similar at the start of the trial? Aside from the experimental intervention, were the groups treated equally?

53
1. Was the assignment of patients to treatment randomized?
Look at the abstract or methodology. Define randomization. Random sampling? Randomization assures that both known and unknown determinants of outcome are even distributed between the treatment and control Avoids selection bias More severe disease = worse results less severe disease = better results Randomization means that patients are given equal chances of being assigned to either the treatment of control. Selection bias is done when more severe patients are put in the control while those with less severe disease are put in the treatment. If randomization is done, this can be avoided. If patients with less sever disease are put in the treatment, the intervention will have better outcomes and it will look better than the control

54
2. Were all the patient who entered the trial properly accounted for and attributed at its conclusion? b. Were the patients analyzed in the group to which they were randomized? patients, including drop outs or withdrawn, were analyzed to their original grouping at the start of the study This preserves the value of randomization No crossing over It simply means that all those belonging to the control group or treatment group are analyzed from beginning to end in this same grouping including those who were dropped or withdrawn or changed treatment. No crossing over treatment modalities were done as this would likely lead to biased results. Excluding non-compliant patients from the analysis leaves behind those who may be destined to have a better outcome and destroys the unbiased comparison provided by randomization. This principle of attributing all patients to the group to which they were randomized results in an "intention-to-treat" analysis. This strategy preserves the value of randomization: prognostic factors that we know about, and those we don't know about, will be, on average, equally distributed in the two groups, and the effect we see will be just that due to the treatment assigned.

55
2. Were all the patient who entered the trial properly accounted for and attributed at its conclusion? a. Was follow up complete? Methodology and Results Section Look at the number of patients enrolled at the outset and compare this with the number of patient reported at the results table. What is the drop out rate? 20 % or more is considered substantial If less than 20% dropped out, check if and intention to treat analysis was done What is intention to treat analysis? Every patient who entered the trial should be accounted for at its conclusion. If substantial numbers are “lost to follow-up”, the validity of the conclusions are open to question. A drop-out rate of 20% or more is usually declared as substantial. If the number of lost to follow-up is less than this, the reader can decide if this affects the conclusion by assuming a “worst case scenario”. This means that the numbers lost in the treatment group are assumed to have bad outcomes and the numbers lost in the control group are assumed to have been cured and if the conclusions differ, a substantial number was lost to follow-up. Another way of deciding whether follow-up was complete is to check whether an intention to treat analysis was done. If this is reported one can safely assume that follow-up was complete.

56
I. Is it valid? Primary Validity Guides
Was the assignment of patients to treatment randomized? Were all the patient who entered the trial properly accounted for and attributed at its conclusion? Secondary Validity Guides Were patient, their clinicians and study personnel “blinded”? Were the groups similar at the start of the trial? Aside from the experimental intervention, were the groups treated equally?

57
1. Were patients, their clinicians, and study personnel "blind" to treatment?
Look at the abstract or methodology. Define blinding. What is its importance? SINGLE blinding? DOUBLE blinding? TRIPLE blinding? Blinding is the process by which the intervention being given is concealed from the patient, the clinicians and the one who analyzes the data. Patients, clinicians and data analysts are likely to have an opinion regarding the experimental treatment. These opinions, whether optimistic or pessimistic, can systematically distort reporting of treatment outcomes. As to avoid these “reporter and observer” bias, blinding is necessary.

58
2. Were the groups similar at the start of the trial?
Baseline characteristics usually labeled Table no. 1 The greater the similarity between known prognostic factors for the control and experimental group, the more likely that the results can be attributed to the intervention, rather than due to the differences in these factors To answer this question, one should look for a report of the comparison of the baseline characteristics of the experimental and control group. For most studies, this is labeled as table 1. In the 4S trial, baseline characteristics were similar. For reassurance about the study’s validity, readers would like to be informed that the treatment and control groups were similar for all the factors that determine clinical outcomes of interest save for the experimental therapy. The greater the similarity between known prognostic factors for the control and experimental group, the more likely that the results can be attributed to the intervention, rather than due to the differences in these factors.

59
3. Aside from the experimental intervention, were the groups treated equally?
Look for interventions other than the treatment under study “co-interventions” distort the results Where outcomes measurements clearly described and determined in the same way between interventions? DEFINE Clinical Outcomes Surrogate Outcomes Interventions other than the treatment under study, when differentially applied to the treatment and control groups, are called “co-interventions”. This might distort the results since they in themselves might cause changes in reported outcomes.

60
II. Overall is the study? If you want to be strict about it, you should answer yes in all 5 questions. A simple rule might be to answer yes to at least, one primary guide and two secondary guides. If you want to be strict about it, you should answer yes in all 5 questions. However, you as the user of the journal can make the decision. A simple rule might be to answer yes to at least, one primary guide and two secondary guides.

61
III. WHAT ARE THE RESULTS?
How large was the treatment effect? RISK IN TREATMENT (Rt) No. of patients who did not get well in the treatment group Total no. of patients in the treatment group RISK IN CONTROL (Rc) No. of patients who did not get well in the control group Total no. of patients in the control group These figures shows only proportion. They show how many did not get well in the treatment, and how many did not get well in the control. They don’t mean anything unless we get the values in the next slides.
 No. of patients who did not get well in the treatment group. Total no. of patients in the treatment group. RISK IN CONTROL (Rc) No. of patients who did not get well in the control group. Total no. of patients in the control group. These figures shows only proportion. They show how many did not get well in the treatment, and how many did not get well in the control. They don’t mean anything unless we get the values in the next slides.")
62
a. What are the results? Absolute Risk Reduction (ARR) = Rc – Rt
Relative Risk (RR) = Rt/Rc RR of 1 : No difference between Treatment and Control RR of >1: Treatment is more harmful RR of <1: Treatment is more effective Relative Risk Reduction (RRR) = 1 – RR Absolute risk reduction is the absolute difference between the proportion who did not get well in the control group compared to the treatment group. Relative risk is the risk of events in the treatment group relative to the control group. The most useful measure to use in explaining the benefit of treatment to patients is the RELATIVE RISK REDUCTION. In this case, a 29% relative risk reduction means that the treatment reduces the adverse events by 29% more than placebo.
 = Rt/Rc. RR of 1 : No difference between Treatment and Control. RR of >1: Treatment is more harmful. RR of <1: Treatment is more effective. Relative Risk Reduction (RRR) = 1 – RR. Absolute risk reduction is the absolute difference between the proportion who did not get well in the control group compared to the treatment group. Relative risk is the risk of events in the treatment group relative to the control group. The most useful measure to use in explaining the benefit of treatment to patients is the RELATIVE RISK REDUCTION. In this case, a 29% relative risk reduction means that the treatment reduces the adverse events by 29% more than placebo.")
63
B. How precise was the treatment effect?
What is the confidence interval? What is the p-value? Confidence interval is the value set by the authors. This value means that the results are true and valid and within the confidence interval. For example, the effect of a BP lowering drug is 95% confidence interval, systolic BP of mmHg. This means that given this drug, a patient’s BP will fall in between mmHg, 95% of the time, if he takes the drug. P value is a value in which the results may be attribute to chance. To decide regarding precision, one should look at the reported 95% confidence interval. The closer these values, the more precise your estimates. If this is not reported check the p-value, anywhere from </= .10 is acceptable. Ideally, the reported minimum and maximum values of this interval should all be positive or all be negative for the absolute risk reduction, all above below one for the relative risk and relative risk reduction to be considered precise.

64
IV. Are the results applicable to my patients?
Are the medical, social and economic resources needed to administer the treatment available in your setting? Consider the acceptability by your patient, his family and community. Are the likely treatment benefits worth the potential harm and costs? Number needed to treat – 1/ARR Cost effectiveness Formula: NNT x price/unit x dose x duration

65
Thomas A. Edison US inventor (1847 - 1931)
THANK YoU! The doctor of the future will give no medicine, but will interest her or his patients in the care of the human frame, in a proper diet, and in the cause and prevention of disease. Thomas A. Edison US inventor ( )
")
Similar presentations




















. Formulate Clinical Question Patient/ population Intervention Comparison Outcome (s) Women with IBS Alosetron.>")
