Download presentation
Presentation is loading. Please wait.

1
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) What PPS Hospitals Need to Know About the UR and Discharge Planning Standards
 2013 What PPS Hospitals Need to Know About the UR and Discharge Planning Standards")
2
Speaker Sue Dill Calloway RN, Esq AD, BA, BSN, MSN, JD CPHRM
President of Patient Safety and Health Care Consulting Past Chief Learning Officer Emergency Medicine Foundation Dublin, Ohio 43017

3
The Conditions of Participation CoP
Regulations first published in 1986 with the current version published December 22, 2011 CMS made more than 2 dozen changes to the CMS CoP as published in the Federal Register on May 16, 2012 and effective July 16, 2012 None effected the UR/Discharge Planning standards First published in the Federal Register and then CMS published Interpretive Guidelines and some of the standards have a survey procedure which is direction to the surveyors

4
The Conditions of Participation
Good way to keep up is sign up for the Federal Register 1 Hospitals should check the survey and certification website once a month for changes 2 Another good place to check monthly is the transmittal website 3 Things are published in a transmittal before being added to the CMS CoP manual Have one person assigned to check these once a month 1 2 3

5
CMS Survey and Certification Website
6
CMS Transmittals

7
TJC Revised Requirements
TJC hospital manual has many changes Brought their standards into closer compliance with the CMS CoP and many R&S changes Different standards for those who use TJC for deemed status and those who do not Example: VA Hospitals do not use TJC for deemed status since they do not apply for Medicaid or Medicare

8
TJC Standard Changes LD Hospital is required to have a UR plan Added 2 EPs (Elements of Performance) 17 and 18 Must also have a UR committee which consists of at least two members who are physicians The committee is responsible for reviewing the medical necessity of admissions, LOS, and services for M&M patients Revisions made to comply with the CMS CoPs Also made a change to LD that went into effect January 12, 2011

9
TJC Standard Changes LD The hospital manages its programs effectively For psychiatric hospitals that use accreditation for deemed status purposes: The hospital has a director of social work services who monitors and evaluates the social work services furnished Note: Social work services are furnished in accordance with accepted standards of practice and established P&P

10
Mandatory Compliance Hospitals that participate in Medicare or Medicaid must meet the COPs for all patients in the facilities Not just those patients who are Medicare or Medicaid Hospitals accredited by TJC, AOA, or DNV Healthcare have what is called deemed status This means you can get reimbursed without going through a state agency survey Can still get complaint or validation survey

11
CMS Hospital CoPs All Interpretative guidelines under state operations manual are found at this website1 Appendix A, Tag A-0001 to A-1164 and 422 pages long Manuals Manuals are now being updated more frequently Still need to check survey and certification website once a month and transmittals 2 1 2

12
Location of All of CMS CoPs Manuals
all manuals at

13
Hospital CoP Manual Dec 22, 2011

14
CMS CoP The Utilization Review section (abbreviated UR) starts at tag 652 Has not been updated in long time TJC amended the leadership chapter (LD ) to require a UR plan and UR committee with at least two physician members Added 2 EPs to comply with the MIPPA or Medicare Improvements for Patient and Providers Act The Discharge Planning session starts at tag 800 Watch for changes in the future in discharge planning in light of the concern for preventing unnecessary readmissions
 to require a UR plan and UR committee with at least two physician members. Added 2 EPs to comply with the MIPPA or Medicare Improvements for Patient and Providers Act. The Discharge Planning session starts at tag 800. Watch for changes in the future in discharge planning in light of the concern for preventing unnecessary readmissions.")
15
Utilization Review Important in healthcare for many reasons
Making sure quality care is provided In most cost effective manner To reduce hospital admissions and length of stays Want to make sure care is medically necessary especially in light of the RACs or recovery audit contractors Hospital should make sure has good UR plan and UR staff So what’s in your UR plan and in your UR program?? Should update it on an annual basis

16
Utilization Review Plan

17
Utilization Review Critical Access Hospitals
Currently Medicare reimbursement for CAHs is not based on DRG designation so not subject to mandatory reviews No similar UR section in the CAH manual for Medicare patients However, Rural Healthcare Quality Network (RHQN) recommends hospitals conduct internal reviews using the InterQual criteria if possible (many private insurers use) Recommend this even though other criteria sets are available and less costly Notes that in the future mandatory reviews may become a reality
 recommends hospitals conduct internal reviews using the InterQual criteria if possible (many private insurers use) Recommend this even though other criteria sets are available and less costly. Notes that in the future mandatory reviews may become a reality.")
18
Utilization Review Certification (justification) may be required for certain procedures or a hospital stay before an insurance company will pay for the stay LOS usually assigned by physician or nurse reviewer, hospital committee, insurance provider or a combination of the four Medicare reviewers currently use InterQual criteria when reviewing medical records to establish if inpatient admissions were medically necessary InterQual (or Milliman-USA) criteria are used by case managers when conducting inpatient utilization review
 may be required for certain procedures or a hospital stay before an insurance company will pay for the stay. LOS usually assigned by physician or nurse reviewer, hospital committee, insurance provider or a combination of the four. Medicare reviewers currently use InterQual criteria when reviewing medical records to establish if inpatient admissions were medically necessary. InterQual (or Milliman-USA) criteria are used by case managers when conducting inpatient utilization review.")
19
Utilization Review InterQual criteria are clinically based on best practice, clinical data and medical literature The criteria are updated continually and released annually The criteria is the first level screening tool to assist in determining if the proposed services are clinically indicated and in the appropriate setting Can’t be use to deny a case as only physicians determine clinical appropriateness If does not meet then case is referred to a physician reviewer for further determination of medical necessity

20
Utilization Review Hospital and the attending physician will have the opportunity to provide additional information on the inpatient Medicare patient that may not have been available to the physician reviewer Of course, case may still be denied and there will be opportunity to request a review by a different physician reviewer If second physician reviewer denies it then opportunity to have case reviewed by an administrative law judge (ALJ) If denied, Medicare takes money back for payment of the hospital stay
 If denied, Medicare takes money back for payment of the hospital stay.")
21
QIO Role in UR This is why it is important for hospitals to respond back to notices in a timely manner This is the amount of time indicated on the letters received from the Quality Improvement Organizations or QIOs The QIO does the peer review activity for CMS Every state has a QIO under contract by CMS QIO is involved with the Scope of Work (SOW) which is updated every 3 years 9th SOW started August 2008 thru July 31, 2012 and 14 states worked on care transition project (See MedQic)
 which is updated every 3 years. 9th SOW started August 2008 thru July 31, 2012 and 14 states worked on care transition project (See MedQic)")
22
Medicare Quality Improvement Org Program
The Medicare QIO program was created by law in 1982 to improve quality and efficiency of services to Medicare patients First phase in the early nineties did this through peer review (PRO) to identify cases where professional standards were not met for initiating corrective actions In second phase, had significant changes with how to improve care and promotion of public reporting and development of scope of work projects
 to identify cases where professional standards were not met for initiating corrective actions. In second phase, had significant changes with how to improve care and promotion of public reporting and development of scope of work projects.")
23
CMS and Quality of Care IOM March 2006 report recommended changes and CMS makes improvements as result of the MMA Law Medicare Prescription Drug, Improvement, and Modernation Act of 2003, section 109(d)(1) CMS views QIO program as the cornerstone to improve quality and efficiency for Medicare patients CMS undertaking activities to manage and measure quality and they want value based purchasing and has a roadmap More under discharge planning
(1) CMS views QIO program as the cornerstone to improve quality and efficiency for Medicare patients. CMS undertaking activities to manage and measure quality and they want value based purchasing and has a roadmap. More under discharge planning.")
24
9th Scope of Work SOW Many times surveyor will ask to see if the hospital has signed a contract with their QIO to participate in the SOW Many times if this is done CMS surveyor may not scrutinize the UR standards 14 states worked on the Care Transition Project to promote seamless transition across settings including hospital to home and to prevent readmissions Ten focus areas; heart failure, MRSA, pressure ulcers, R&S, AHRQ culture tool, surgical care, drug safety, public reporting, LD and quality assessment tool Focused disparities (diabetes) and chronic kidney disease
 and chronic kidney disease.")
25
9th Scope of Work SOW QIOs will continue to review quality of care given to Medicare patients, beneficiary appeals of certain notices, potential EMTALA, and implementing QI activities as a result of case reviews, sanctions etc Some states adopted some of the initiatives Some measures overlap with IHI (Institute for Healthcare Improvement) 5 Million Lives Campaign and 100K live campaign Some also overlap with American Heart Association on the Get with the Guidelines campaign (GWTG)
 5 Million Lives Campaign and 100K live campaign. Some also overlap with American Heart Association on the Get with the Guidelines campaign (GWTG)")
26
10th Scope of Work QIO 10th scope of work started August 1, 2011 and continues for three years Will continue efforts to prevent unnecessary hospitals and goal is 20% reduction Has community based care transition program Also patient safety goals as to reduce hospital acquired conditions by 40% (falls, CAUTIs, staff turnover, etc.), reduce ADEs, Improve quality through value-based purchasing Reduce HAI (CAUTIs, CLABSIs, CDIs, SSI)
, reduce ADEs, Improve quality through value-based purchasing. Reduce HAI (CAUTIs, CLABSIs, CDIs, SSI)")
27
Medical Necessity CMS takes the position that whether a patient should be admitted as an inpatient is a complex medical judgment that should be made by the physician based on; Severity of the “signs and symptoms” exhibited by the patient, Medical probability of an adverse outcome for the patient, and The need and availability of diagnostic studies See MLN Matter SE1037

28
Transmittal SE /25/2011

29
Inpatient Review for Medicare Patients
A tool used by the QIO may be helpful to determine medical necessity but does not guarantee payments for admission or continued stay Demographics Patient name, ID number Attending Name and contact information The day or dates under review SI (symptom intensity) How sick is the patient? This places the patient’s services in context with their clinical condition and is needed both for the initial review and for concurrent review
 How sick is the patient This places the patient’s services in context with their clinical condition and is needed both for the initial review and for concurrent review.")
30
Medical Necessity Symptom intensity (continued)
What is the main clinical issue? Abnormal vital signs? Pain present- where, what is the cause? Neurological status: alert to obtunded Brief description of diagnostic tests (especially if lab or x-rays are abnormal) Any consultations and evaluations or procedures?
 Any consultations and evaluations or procedures")
31
Intensity of Services IS (Intensity of services) What care is the patient receiving? IV medications and frequency Any IV PRN meds given for nausea, pain? How often each day? IV Fluids/ TPN Blood or blood products (should have a HCT as a reason) Oxygen needed? FiO2 and route? ABGs done or O2 sats?
 Oxygen needed FiO2 and route ABGs done or O2 sats")
32
Discharge Screens DS (Discharge Screens) What is the long-term plan? An “unsafe” discharge will initiate a quality of care review. What is the expected destination after hospitalization? What discharge planning activities are being done What care needs are there post discharge? Educational Needs? Are there any significant psychosocial issues?

33
Intensity of Services Intensity of Services continued
Diet/Tube feeds/gavage (what is infants weight) If patient is on a sliding scale, What were the high/low glucose values? How many coverage units were given on each day (not the routine doses)? Wound management: describe wound and dressing/debridement/special issues Any other treatments or therapies?
 If patient is on a sliding scale, What were the high/low glucose values How many coverage units were given on each day (not the routine doses) Wound management: describe wound and dressing/debridement/special issues. Any other treatments or therapies")
34
MedQIC MedQIC has the quality net website with free resources for QI interventions, tools, and toolkits Sign up to get their free monthly publication called MedQiC (Medicare Quality Improvement Community) Purpose is to share resources including resources on the 9th scope of work, delirium, depression, infections, incontinence, restraint, UTI, patient safety, transitions in care, AV fistula first, etc.
 Purpose is to share resources including resources on the 9th scope of work, delirium, depression, infections, incontinence, restraint, UTI, patient safety, transitions in care, AV fistula first, etc.")
36
CMS Guidance on Hospital Inpatient Admissions
Medical necessity is a hot button with the RACs, Medicare Administrative Contractors (MACs), fiscal intermediaries (FIs) and comprehensive error rate testing (CERT) contractors CMS released an educational guideline to assist hospitals regarding inpatient admission decisions To help ensure that hospitals are using proper screening criteria to analyze documentation and make medical necessity determinations Chapter 6 of the Medicare Program Integrity Manual, Section 6.5 is available at on the CMS website
, fiscal intermediaries (FIs) and comprehensive error rate testing (CERT) contractors. CMS released an educational guideline to assist hospitals regarding inpatient admission decisions. To help ensure that hospitals are using proper screening criteria to analyze documentation and make medical necessity determinations. Chapter 6 of the Medicare Program Integrity Manual, Section 6.5 is available at on the CMS website.")
38
Utilization Review A-0652 Hospital must have a UR plan that provides for review of services furnished by the institution and the members of the MS to Medicare and Medicaid beneficiaries UR plan should state responsibility and authority of those involved in the UR process Surveyor will make sure activities performed as in UR plan Need to include review of medical necessity of admissions

39
Utilization Review Review of medical necessity for:
Appropriateness of the setting Extended stays and Professional services rendered This is really important in light of the Recovery Audit Contractors or RACs American Hospital Association, AHIMA, and CMS has website of resources for the RACs RAC program to identify improper Medicare payments including overpayment and underpayments

40
AHA Website on RAC Program

41
CMS RAC Website

43
Survey Procedure Tag 652 These are the questions to the surveyors to verify Determine that the hospital has a utilization review plan for those services furnished by the hospital and its medical staff to M&M patients. Verify through review of records and reports, and interviews with the UR chairman and/or members that UR activities are being performed as described in the hospital UR plan. Review the minutes of the UR committee to verify that they include dates, members in attendance, extended stay reviews with approval or disapproval noted in a status report of any actions taken.

44
UR Plan UR Plan should say who is on the UR committee
Such as the physician advisor, CNO, discharge planners, social services, business office manager, HIM director, administration, UR nurse, billing office, etc. Should discuss meeting frequency such as meets once a month It should address conflicts of interest so anyone with financial interest in the hospital can not be on the committee Should include a confidentiality section so all data, minutes, worksheets are confidential

45
Functions of a UR Committee
Should include functions of the UR committee such as: To establish and carry out a program of admission certification and continued stay review of all patients in accordance with applicable state and federal laws and regulations To supervise the utilization review activities of non physician reviewers To assure coordination between concurrent review activities, quality assurance, and risk management activities, and reimbursement agencies

46
Functions of the UR Committee
To assist in the selection and ongoing modification of criteria and standards To recommend changes in hospital procedures, medical Staff practices or continuing education programs as indicated on analysis of review findings To serve as utilization review committee for the skilled swing bed activities To act on any topics referred to them by the Medical Staff, Administration, or any other hospital committee To address potential over-utilization or under utilization issues

47
UR Plan UR plan can include the method of review
All patients admitted to the hospital will reviewed by the UR nurse for appropriateness and medical necessity Includes M&M patients, CHAMPUS, patient insurance covered by private contract, self pay, etc What guidelines are used such as InterQual or Milliman etc. Concurrent reviews are done using the same criteria or the information provided by the insurers If criteria does not exist then will work with physician and patient and family to move the patient to the appropriate level of service

48
UR Plan If UR nurse sees unusually high costs or frequent ordering of excessive services then can talk to physician advisor Or can subject case to Preadmission Review or in-depth peer review Decisions made by UR nurse will be based on standards adopted by the MS and QIO Include in the policy the preadmission review process Precertification of elective surgeries should be done by the physician’s office but hospital will verify precert Include admission review process

49
Utilization Review Make sure you get observation rules correct especially with condition code 44 CMS issue UR CoP Memo June 2, 2007 Exception for UR plan is if the Hospital has an agreement with the QIO in their state to assume binding review Hospitals may have a contract with QIO to review admissions, quality, appropriateness and diagnostic information related to Medicare inpatients Surveyor will look to see if hospital has a signed contract with their state QIO

50
Composition of UR Committee 654
Consists of 2 or more practitioners who carry out UR function At least 2 members must be doctors The UR committee must be either a staff committee of the hospital or A group outside that has been established by the local medical society for hospitals in that locale and established in a manner approved by CMS

51
UR Committee 654 A committee may not be conducted by an individual who has a direct financial or ownership interest (5% or more) or Who was professionally involved in the care of the patient whose case is being reviewed Surveyor will look to see if the governing board has delegated UR function to a outside group if impracticable to have a staff committee

52
Frequency of Review 655 UR plan must provide review for Medicare/Medicaid (M/M) patients with respect to medical necessity Admissions (before, at, or after admission) Usually should screen within one working day of admission and use severity of illness or intensity of service as discussed previously Duration of stay Professional services furnished including drugs and biologicals
 Usually should screen within one working day of admission and use severity of illness or intensity of service as discussed previously. Duration of stay. Professional services furnished including drugs and biologicals.")
53
Scope of Reviews A-0655 Reviews may be on a sample basis except for reviews of cases assumed to outlier cases because of extended stay cases or high costs Surveyor will examine UR plan to determine if medical necessity is reviewed P&P should state what to do such as UR nurse speaks with attending, goes to the physician reviewer, when ABNs are issued, IM Notices, QIO guidelines etc. If IPPS hospital there should be a review of the duration of stay in cases assumed to be outlier

54
Admissions or Continued Stay
Determination that admission or continued stay is not medically necessary is made by one member of UR committee if the physician concurs with determination or fails to present their views when afforded the opportunity Must be made by two members in all other cases (656) Before determination not medically necessary, UR committee must consult the MD responsible for the care and afford opportunity to present their views
 Before determination not medically necessary, UR committee must consult the MD responsible for the care and afford opportunity to present their views.")
55
Hospital Discharge Summary Form

56
Admissions or Continued Stay
Then committee must provide written notification no later than two days after determination to the hospital, patient and practitioner responsible for care If attending doctor does not respond or contest the findings of the committee, the findings are final If physician of UR committee finds not medically necessary no referral of committee is necessary and he may notify the attending doctor If non-physician makes the determination it must go to the committee or the physician reviewer A non-physician can not make this final determination

57
Review of Professional Services 658
The committee must review professional services provided To determine medical necessity And to promote the most efficient use of available health facilities and services Topics for the committee may include overuse or underuse of necessary services Timeliness of scheduling of services such as diagnostic and operating rooms

58
Discharge Planning Discharge planning is important in today’s environment especially in light of reform laws If hospital do not do this right and the result is a higher that average readmission rate in 2012, the hospital could be financially penalized by CMS 20% of Medicare patients are readmitted within 30 days CMS is expected to make some changes to this section because of this Hospitals need to reengineer the discharge process

59
Patient Protection and Affordable Care Act
The new law establishes a VBP program, or value-bases purchasing, to pay hospitals for their actual performance Measures selected for pay include those used in the Medicare pay for reporting program such as measures for heart attack, heart failure, pneumonia, surgical care and patient satisfaction (HCAHPS) Purpose to improve coordination, quality and efficiency of health care services
 Purpose to improve coordination, quality and efficiency of health care services.")
60
Patient Protection and Affordable Care Act
Must develop episode-of-care and post-acute care quality measures Hospitals are required to submit data on these quality measures through an EHR which will be posted on hospital compare Law specifies the following episode-of-care quality measures Functional status improvement Rates of avoidable hospital readmissions Rates of discharge to the community Rates of admission to an emergency department after a hospitalization

61
Readmission Rates Vary
Readmission rates vary widely in the US Too often quality of care during transition from hospital to home is not good Data shows readmission rate for MI and CHF vary Found only modest association between performance on discharge measures and patient readmission rates Public reporting unlikely to yield large reductions in unnecessary readmissions We need to improve in the ambulatory section See A. K. Jha, E. J. Orav, and A. M. Epstein, Preventing Readmissions with Improved Hospital Discharge Planning, NEJM Dec 31, (27):
:")
62
Readmissions and Discharges
One in 5 hospital discharges (20%) is complicated by adverse event within 30 days 20% were readmitted within 30 days with 1/3 leading to disability Often leads to visits to the ED and rehospitalization 6% of these patients had preventable adverse events 66% were adverse drug events The incidence and severity of adverse events affecting patients after discharge from the hospital. Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. Ann Intern Med. 2003;138:
 is complicated by adverse event within 30 days. 20% were readmitted within 30 days with 1/3 leading to disability. Often leads to visits to the ED and rehospitalization. 6% of these patients had preventable adverse events. 66% were adverse drug events. The incidence and severity of adverse events affecting patients after discharge from the hospital. Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. Ann Intern Med. 2003;138:")
63
Preventing Readmissions
HHS study finds a high rate of Medicare patient deaths due to adverse events (AE) 15,000 Medicare patients experience an AE during healthcare delivery that lead to their death every month Nov 16, 2010 OIG study Found 1 in every 7 discharges (13.5%) experience an AE and the cost to CMS is $324 million 44% of all AE were preventable and 51% were not November 2010, OEI
 15,000 Medicare patients experience an AE during healthcare delivery that lead to their death every month. Nov 16, 2010 OIG study. Found 1 in every 7 discharges (13.5%) experience an AE and the cost to CMS is $324 million. 44% of all AE were preventable and 51% were not. November 2010, OEI")
65
AHA Guide to Reduce Avoidable Readmissions
AHA had committees look at the issue of how to reduce unnecessary hospital readmissions AHA published several memos and a 2010 Health Care Leader Guide to Reduce Avoidable Readmissions Issues memo on Sept on Reducing Avoidable Hospital Readmissions Includes evaluation of post acute transition process which is the process of moving from the hospital to home or other settings

66
AHA Guide to Reduce Readmissions

67
CMS Discharge Checklist
CMS website recommends the discharge planning team use a checklist to make transfer more efficient It is available at Previously research showed the value of hospital discharge planners using a discharge checklist We need to dictate the discharge summary immediately when the patient is discharged We need to document that it is in the hands of the family physician

68
CMS Your Discharge Planning Checklist

70
CMS Discharge planners should be a member of the hospital committee to prevent unnecessary readmissions Discharge planners and transition coaches may actually make the physician appointments Ensure medication information is clearly understood by the patients and use pharmacists when needed in the process CMS discharging planning standards start at tag number 800

71
Things to Consider Form a committee on redesigning the discharge process Do a literature search and pull articles Look at the different transition studies that have been done and which ones have been successful Care Transition, Transition of Care, RED, Guided care, H2H, IHI Transforming Care at the Bedside, STAAR, Boost, GRACE, Interact, Evercare, etc. Have physician dictate discharge summary as soon as patient is discharge Hospitals needs to get it into the hands of the primary care physician and document this in the chart

72
Things to Consider Medical staff should dictate what needs to be in the discharge summary beyond what CMS and TJC require Hospital should schedule all follow up appointments with practitioners for the patients Hospital should put in writing for the patient and in the discharge summary Any tests that are pending that are not back yet Any future tests and these should be scheduled before the patient leaves the hospital

73
Things to Consider Use a discharge checklist for staff to use
Pa Patient Safety Authority has one called “Care at Discharge” at Society of Hospital Medicine has one at Give patients a copy of the CMS checklist “Your Discharge Planning Checklist” at Give a list of medications with times and reason for taking

74
Things to Consider Ensure education on all new meds and use teach back to ensure education and give information in writing Ensure patient is given a copy of the plan of care Give patient in writing their diagnosis and written information about their diagnosis Have patient repeat back in 30 seconds understanding of their discharge instructions Includes symptoms that if they occur what you want to do and who to call

75
Things to Consider Call back all patients discharged and review information and reinforce discharge instructions Have a call back number that patients and families can use 24 hours a day, seven days a week Reconciling the discharge plan with national guidelines and critical pathways when relevant Assess your hospital’s readmission rate Pull charts and review for any patient who is readmitted within 30 days

76
Medication List

77
Appointments for Follow Up

78
Discharge Planning A-800 Must have a discharge planning process that applies to all patients Inpatients and outpatients P&P must be in writing Written discharge planning process must reveal a clear process to be followed Necessary to prevent readmission Surveyor will review patient care plans for discharge planning interventions

79
So What’s in Your P&P?

80
Discharge Protocol for Babies

81
Identification of Patients 800
Must identify at early stage of hospitalization, all patients who are likely to suffer adverse consequences if no discharge planning No national tool to do this May include factors as functional status, cognitive ability and family support Patients at high risk should be identified from screening process Time to do left up to the hospital but as early as possible

82
Case Management Consults

83
Discharge Planning Evaluation 806
Hospital must provide a discharge planning evaluation to patients or upon the request of the physician Needs assessment can be formal or informal Assess factors on what the patient will need when discharged; bio-psychosocial needs and patient and caregiver’s understanding of discharge needs Can be a tool or protocol

84
Discharge Planning Evaluation
Surveyor will ask how patients are made aware of their right to request a discharge plan Many hospitals include this in the patient’s rights which are given to the patient in writing Can also be posted in signs Must be given the pamphlet “Important message from Medicare” if Medicare patient Patients given within 2 days of admission and must sign and date Patients are given again within 2 days of discharge if admitted more than two days

85
Discharge Planning Responsibility 807
RN, SW, or qualified person must develop and supervise the development of the evaluation Person who does discharge planning evaluation needs to have experience and knowledge of social and physical factors that affect functional status to meet patient needs Such as in emphysema if needed to coordinate respiratory therapy, nursing care, financials for home health Must have knowledge of community resources Ideally, discharge planning is interdisciplinary process

86
Evaluation 808 Discharge planning evaluation must include likelihood of needing post-hospital services and availability of services Keep complete file on community based services such as LTC, sub acute care, and home care Is physical, speech, OT or RT needed? Use the QAPI program to determine if discharge planning process is effective

87
Self Care Evaluation 809 Discharge planning evaluation must include if patient can do self care and return to pre-hospital environment Assess willingness of patient and family to do care Inform patient of freedom to choose providers or post hospital care (823) Give list of Medicare certified HHA that serve your area (SSA 1861) including ownership information Must assess if need hospice or LTC and give list of Medicare certified ones in your area Document in the medical record that the list was given
 Give list of Medicare certified HHA that serve your area (SSA 1861) including ownership information. Must assess if need hospice or LTC and give list of Medicare certified ones in your area. Document in the medical record that the list was given.")
88
Discharge Planning 809 Hospital can develop its own list or can for SNF can also print out list from nursing home compare website Surveyor to review a sample of discharge planning evaluations Will note if interdisciplinary input is documented Counsel patient and family for post hospital care (822)
")
89
Timely Discharge Evaluation 810
Hospital must complete the evaluation timely to avoid unnecessary delays in discharge So appropriate arrangements can be made Assessment should start soon after admission Surveyor will review several patient discharge plans for appropriate coordination of health and social resources

90
Discharge Evaluation 811 The hospital must include the discharge planning evaluation in the patient’s medical record This is necessary to establish an appropriate discharge plan Must discuss the results of the evaluation with the patient Transitions in care project show increased utilization of home health and LTC services

91
Patient Discharge Plan

92
Discharge Plan The hospital must make sure that the discharge plan requirements are met (817) RN, social worker, or other qualified person must develop or supervise the development of the discharge plan if one is needed (818) Make sure staff are trained and licensed Patients have the right to participate in the development and implementation of their plan of care Physicians can request a discharge plan (819)
 Make sure staff are trained and licensed. Patients have the right to participate in the development and implementation of their plan of care. Physicians can request a discharge plan (819)")
93
Discharge Plan Hospital must arrange for the initial implementation of the patient’s discharge plan (820) This includes arranging for the post hospital services and care This includes educating the patient about their post hospital care plans Hospital must reassess the patient discharge plan if there are factors that affect the continuing need of the plan Reassessment takes place and the plan is updated as needed

94
Discharge Plan Patients and family members or other interested parties are counseled to prepare them for post hospital care (822) Patients need to be kept of the progress May need to demonstrate or verbalize the care need Teach back is good method to verify knowledge or return demonstrations of procedures such as emptying a foley or packing a wound

95
Discharge Plan If in MCO hospital must indicated which ones have contract with home health or LTC (826) Hospital must now document in the medical record that the list of home health or LTC facilities was presented to the patient (827) Rewrite your P&P to include this Hospital must inform patient of freedom to choose post hospital provider (828) and respect their wishes (829) Disclose any financial interests HHA may request to be on the list
 Rewrite your P&P to include this. Hospital must inform patient of freedom to choose post hospital provider (828) and respect their wishes (829) Disclose any financial interests. HHA may request to be on the list.")
96
Transfer or Referral 837 Must transfer or refer patients to appropriate facilities, agencies, or outpatient services for follow up care Must send along necessary medical records Make sure patients get appropriate post hospital care Remember the federal EMTALA law for ED patients Must document if patient refuses discharge planning services Written authorization before release of information

97
CMS Hospital Worksheets Third Revision
October 14, 2011 CMS issues a 137 page memo in the survey and certification section Memo discusses surveyor worksheets for hospitals by CMS during a hospital survey Addresses discharge planning, infection control, and QAPI It was pilot tested in hospitals in 11 states and on May 18, 2012 CMS published a second revised edition Piloted test each of the 3 in every state over summer 2012 November 9, 2012 CMS issued the third revised worksheet which is now 88 pages

98
CMS Hospital Worksheets
Will select hospitals in each state and will complete all 3 worksheets at each hospital This is the third and most likely final pilot and in 2013 will use whenever a validation survey is done at a hospital by CMS Third pilot is non-punitive and will not require action plans unless immediate jeopardy is found Hospitals should be familiar with the three worksheets

99
Third Revised Worksheets
100
CMS Hospital Worksheets
Goal is to reduce hospital acquired conditions (HACs) including healthcare associated infections Goal to prevent unnecessary readmission and currently 1 out of every 5 Medicare patients is readmitted within 30 days Many hospitals (66%) financially penalized after October 1, 2012 because they had a higher than average rate of readmissions The underlying CoPs on which the worksheet is based did not change
 including healthcare associated infections. Goal to prevent unnecessary readmission and currently 1 out of every 5 Medicare patients is readmitted within 30 days. Many hospitals (66%) financially penalized after October 1, 2012 because they had a higher than average rate of readmissions. The underlying CoPs on which the worksheet is based did not change.")
101
CMS Hospital Worksheets
However, some of the questions asked might not be apparent from a reading of the CoPs A worksheet is a good communication device It will help clearly communicate to hospitals what is going to be asked in these 3 important areas Hospitals might want to consider putting together a team to review the 3 worksheets and complete the form in advance as a self assessment Hospitals should consider attaching the documentation and P&P to the worksheet

102
CMS Hospital Worksheets
The regulations are the basis for any deficiencies that may be cited and not the worksheet per se The worksheets are designed to assist the surveyors and the hospital staff to identify when they are in compliance Will not affect critical access hospitals (CAHs) but CAH would want to look over the one on PI and especially infection control Questions or concerns should be addressed to
 but CAH would want to look over the one on PI and especially infection control. Questions or concerns should be addressed to")
103
Discharge Planning There are 23 pages in the discharge planning section and starts at page 66 Includes hospital information such as name, address, CCN number as previously discussed Will cite deficiencies on a CMS Form 2567 if observed which is a statement of deficiencies and plan of correction when used for validation surveys CMS discharge planning regulations and interpretive guidelines start at tag 800

104
Discharge Planning Worksheet 3rd Revision

106
Discharge Planning Worksheet
Are discharge P&P in effect for all inpatients? Is there evidence on every unit that there is discharge planning activities? Are staff following the discharge planning P&P? Is there a discharge planning process for certain categories of outpatients such as observation, ED patients and same day surgery patients? Could add questions to the assessment tool and include in questions asked in pre-admission tests for OP surgery

107
Discharge Planning Worksheet
For patients not initially identified as in need of discharge plan, is there a process for updating this based on changes in a patient’s condition? Many hospitals have the nurse doing the admission assessment ask a set of predetermined questions to see if assistance is needed How do you update this when there is a change? Is a discharge plan prepared for each inpatient? Does hospital have a process for notifying patients they can request a discharge planning evaluation? Or process for the patient representative to request

108
Discharge Planning Worksheet
Surveyor will interview patient to see if they were aware they could request a discharge planning evaluation Can the hospital show that they gave the patient a notice of their rights? Will interview doctors and make sure they know they can request a discharge planning evaluation (819 and 806) If doctor not aware will ask hospital to provide evidence on how it informs the MS about this
 If doctor not aware will ask hospital to provide evidence on how it informs the MS about this.")
109
Discharge Planning Worksheet
Will ask staff to describe the process for physicians to order a discharge plan Does P&P provide a process for ongoing reassessment of discharge plan in case of changes to the patient’s condition (819)? Does hospital review discharge planning process on an ongoing manner as through PI?
 Does hospital review discharge planning process on an ongoing manner as through PI")
110
Discharge Planning Worksheet
Does hospital track readmission rates as part of discharge planning? Does assessment include if readmission was potentially preventable? If preventable then did the hospital make changes to the planning process? Does hospital collect feedback from post-acute providers for effectiveness of the hospital’s discharge planning process? This would include places like LTC, assisted living or home health agencies

111
Discharge Planning Tracers
Has a discharge planning tracer section 4 Surveyors is to interview one or two inpatients Surveyor is to review the closed medical record of two or three patients who was discharged Will try and include one patient who was readmitted within 30 days Will mark worksheet to show if it was an interview, discharge planning document review, medical record review or other document that was reviewed

113
Discharge Planning Tracers
Was the screening done to identify if the inpatient needed a discharge planning evaluation? Includes at the time of admission, after an admission but at least 48 hours prior to discharge, or N/A In some hospitals all patients get a discharge plan Can staff demonstrate that the hospital’s criteria and screening process for discharge evaluation were correctly applied (800)? Was discharge planning evaluation done by qualified person (SW, RN) as defined in the P&P? (806)
 Was discharge planning evaluation done by qualified person (SW, RN) as defined in the P&P (806)")
114
Discharge Planning Tracers
Are the results of the discharge planning evaluation documented in the chart? Did the evaluation include an assessment of the patients post-discharge care needs? Patient need home health referral Patient needs bedside commode Patient needs home oxygen Patient needs post hospital physical therapy Meals on wheels, etc.

115
Discharge Planning Tracers
Did the evaluation include an assessment of: Patient’s ability to perform ADL (feeding, personal hygiene, ambulation, etc.)? Family support and ability to do self care? Whether patient will need specialized medical equipment or modifications to their home? Is support person or family able to meet the patient’s needs and assessment of community resources ? Was patient given a list of HHA or LTC facilities in the community and must be documented in the record and the list appropriate (806)
 Family support and ability to do self care Whether patient will need specialized medical equipment or modifications to their home Is support person or family able to meet the patient’s needs and assessment of community resources Was patient given a list of HHA or LTC facilities in the community and must be documented in the record and the list appropriate (806)")
116
Discharge Planning Tracers To LTC
Separate set of questions if patient admitted from LTC or assisted living Did evaluation include if LTC has capacity for patient to go back there? Does it include assessment if insurance coverage will cover it if they go back there? Was the discharge planning evaluation timely to allow for arrangements if the patient needs to go back there Was the patient’s representative involved in these discussions? Discharge plan needs to match the patient’s needs (811, 130)
")
117
Discharge Planning Tracers
Will look for evidence of hospital of patients and support persons Was patient referred back for follow up with their PCP or a health center? Was there a referral to PT, mental health, hospice, OT etc. as needed? Was there a referral for community based resources such as transportation services, Department of Aging, elder services etc.? Arranged for needed equipment such as oxygen, commode, wheel chair etc.

118
Discharge Planning Worksheet
If transferred to another inpatient facility was the discharge summary ready and sent with patient? The following controversial section was changed in the 3rd revision Was discharge summary sent before first post-discharge appointment or within 7 days of discharge? Was follow up appointment scheduled? Now says send necessary medical record information to providers the patient was referred prior to the first post-discharge appointment or 7 days, whichever comes first

119
Discharge Planning Worksheet
Was the necessary medical record information ready at the time of transfer if patient sent to another facility Was there any part of the discharge plan that the hospital failed to implement that resulted in a delay in discharge Was there documentation in the medical record of results of tests pending at the time of discharge both to the patient and the post hospital provider? Was patient readmitted within 30 days?

120
Preventing Readmissions
It is the preventable ones that hospitals need to work on Medicare data shows that over half of patients readmitted received no follow up care Recent studies show interventions targeted at post-acute care transition can reduce readmissions by one third (Coleman and Naylor) Technologies for Improving Post-acute Care Transitions, Center for technology and Aging, Sept 2010
 Technologies for Improving Post-acute Care Transitions, Center for technology and Aging, Sept")
121
The End! Questions???? Sue Dill Calloway RN, Esq
AD, BA, BSN, MSN, JD CPHRM President of Patient Safety and Health Care Consulting Chief Learning Officer of the Emergency Medicine Foundation Dublin, Ohio 43017 Additional slides on TJC standards

122
Joint Commission Standard for Hospitals
PC and RC EP2 Medical record must contain information on plan of care and revisions to the plan of care and discharge diagnosis TJC has PC which provided information on planning the patient’s care PC has end of life standards This is provided for reference Discharge planners and social workers should be familiar with these standards in addition to the floor nurse caring for the patient

123
Planning the Patient’s Care PC.01.03.01
The hospital plans the patient’s care Need to individualize the patient’s treatment based on their unique needs Treatment must be appropriate to the results of the assessment performed May need to modify the plan of care based on the assessments done Could result in transfer to another facility or discharge EP1 Patient’s care is based on what is identified by the assessments and reassessments and the results of the diagnostic tests

124
Planning the Patient’s Care PC.01.03.01
EP5 The written plan of care is based on the patient’s goals and the time frames, settings, and services required to meet those goals EP22 Staff need to evaluate the patient’s progress in light of the goals and the patient’s plan of care EP23 Hospital revises the plan of care and goals based on the patient’s need Failure to do a plan of care soon after the patient is admitted and maintained it in the medical record after the patient is discharged is a top problematic standard with CMS

125
Patient Education PC The hospital provides patient education and training based on each patient’s needs and abilities Patients are often discharged home earlier than in the past Patients may have to do more self care such as changing bandages, drains to home infusion therapy This makes patient education even more important Also important to prevent unnecessary readmission especially related to medication use Patient learning needs must be assessed Patient education is important issue to TJC

126
Patient Education PC EP10 Education and training to patient will include the following based on the patient’s condition and assessed needs Explanation of the plan for care Basic health practices and safety Safe medication use Nutritional interventions, diets, supplements Pain issues such as pain management and methods Information on oral health (much information later on this including oral bacterium (periodontal disease) as cause of cardiovascular disease, MI, VAP, stroke, CAD)
 as cause of cardiovascular disease, MI, VAP, stroke, CAD)")
127
Patient Education PC EP10 Education and training to the patient (continued) Safe use of medical equipment Safe use of supplies Rehab to help the patient reach maximum independence EP25 Must evaluate the understanding of the education and training provided Teach back is one method to verify understanding Ask me three program by the National Patient Safety Foundation

129
Use a Patient Education Form

130
Use a Patient Education Form

131
http://www. docstoc. com/docs/downloaddoc. aspx/

132
Patient Education Checklist

133
Patient Education PC EP27 The hospital provides the patient education on how to communicate concerns about patient safety issues that occur before, during, and after care is received Instructions might be to contact their physician after discharge May be if certain condition reoccurs to call 911 or go to the closest emergency department Patients when discharge should be informed of signs and symptoms of when to return (TJC discharge tracer)
")
134
Care After Discharge or Transfer
PC states that the hospital has a process that addresses the patient’s need for continuing care after discharge or transfer EP1 Hospital describes the reason for and conditions under which the patient is discharged or transferred For example care may no longer be medically necessary Patient may need services that are not provided by your hospital such as open heart surgery EP2 Need to describe the process for shifting responsibility to a new clinician or hospital or service

135
Care After Discharge or Transfer
EP3 Hospital describes mechanism for external transfer of patient Example would be to contact receiving hospital and get acceptance, fill out transfer form, send medical records, send in ambulance when appropriate etc. Remember the federal EMTALA law for patients who in the ED and are unstable EP4 The hospital agrees with the receiving organization about each of their roles to keep the patient safe during transfer May need transported by helicopter or ACLS or BLS unit

136
Care After Discharge or Transfer
EP22 Patients are informed of their rights to choose among participating Medicare providers and the hospital does not limit those qualified providers (DS) EP23 and 24 During discharge planning if determine patient needs home health or LTC then give them a list of the ones available and document you gave the list (DS) This is a CMS requirement The hospital can not just automatically send the patient to their home health agency It is truly the patient’s freedom of choice
 EP23 and 24 During discharge planning if determine patient needs home health or LTC then give them a list of the ones available and document you gave the list (DS) This is a CMS requirement. The hospital can not just automatically send the patient to their home health agency. It is truly the patient’s freedom of choice.")
137
Care After Discharge or Transfer
EP26 The hospital has written discharge planning P&P applicable to all patients (DS) Must also disclose any financial interest such as the hospital owns the nursing home or the home health agency Remember to take care to prevent any unnecessary readmissions to the hospital Dictate the discharge summary immediately and document that you got it into the hands of the PCP who is going to see the patient post discharge
 Must also disclose any financial interest such as the hospital owns the nursing home or the home health agency. Remember to take care to prevent any unnecessary readmissions to the hospital. Dictate the discharge summary immediately and document that you got it into the hands of the PCP who is going to see the patient post discharge.")
138
Assessment & Discharge PC.04.01.03
The hospital discharges or transfers the patients based their assessed needs and the hospital’s ability to meet those needs EP1 Need to begin the discharge process early in the patient’s admission EP2 Identify any need for psychosocial or physical care after discharge EP3 Patient, family, staff, physician, LIPs etc all participate in the planning the patient’s discharge or transfer

139
Assessment & Discharge PC.04.01.03
EP4 Arrange the services the patient will need after discharge before they leave EP10 The hospital conducts reassessments of its discharge planning process within its established time frames for reassessment (DS) EP11 The reassessment of the discharge planning process includes a review of discharge plans to determine if the discharge plans meet the needs of patients (DS)
 EP11 The reassessment of the discharge planning process includes a review of discharge plans to determine if the discharge plans meet the needs of patients (DS)")
140
Education Before Discharge PC.04.01.05
Before the hospital discharges or transfers a patient is informed and educated the patient follow-up care EP1 When the patient needs to be discharged or transferred this information is shared with the patient along with the patient’s needs EP2 Hospital informs the patient the kinds of care that will be needed after discharge Some patients will need to be in a LTC or might need home health services or assisted living

141
Education Before Discharge PC.04.01.05
EP3 Hospital needs to give the patient information about why they are being discharged or transferred EP5 Patient must also be provided about any alternatives to the transfer EP7 The hospital needs to educate the patient about continuing care the patient will need and how to obtain this care EP8 Patient must be given understandable discharge instructions Remember issue of low health literacy and studies show patients may not understand discharge instructions

142
Communication Discharge to Service Providers
PC state that when a patient is discharged or transferred The hospital gives information about the care provided to the patient And to other service providers who will provide the patient with care Continuity of care is important so that the next treating practitioner has the information need to take care of the patient Communication is important for patient safety reasons and to prevent readmissions

143
Communicate Information to Next Provider
PC states that the hospital must inform other service providers who will provide care to the patient When they are discharged or transferred about the following (EP1); Reason for discharge or transfer Patient’s physical and psychosocial status A summary of care provided Patient’s progress toward goals List of community resources given to the patient
; Reason for discharge or transfer. Patient’s physical and psychosocial status. A summary of care provided. Patient’s progress toward goals. List of community resources given to the patient.")
144
Utilization Review Plans
2 new EPs effective January 1, 2011 LD EP 17 and 18 (deemed status) LD EP 17: The hospital (and CAH distinct units) has a utilization review plan that provides for review of services furnished by the hospital and the medical staff to patients entitled to benefits under the Medicare and Medicaid programs. LD EP 18: Utilization review activities are implemented by the hospital/critical access hospital in accordance with the plan
 LD EP 17: The hospital (and CAH distinct units) has a utilization review plan that provides for review of services furnished by the hospital and the medical staff to patients entitled to benefits under the Medicare and Medicaid programs. LD EP 18: Utilization review activities are implemented by the hospital/critical access hospital in accordance with the plan.")
145
Discharge Planning Revised
There are 22 pages in the discharge planning section and starts at page 66 Includes hospital information such as name, address, CCN number as previously discussed Will cite deficiencies on a CMS Form 2567 if observed which is a statement of deficiencies and plan of correction CMS discharge planning regulations and interpretive guidelines start at tag 800 Remember hospitals with a higher than average readmission rate after Oct 2012 can be financially penalized

146
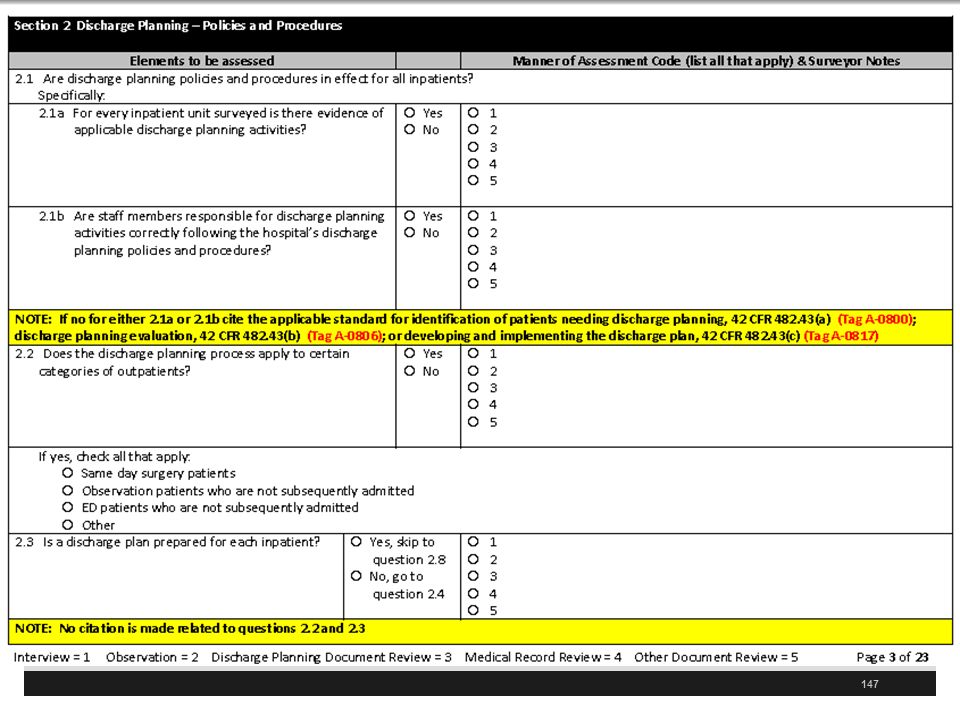
Discharge Planning Worksheet

148
Discharge Planning Worksheet
Are discharge P&P in effect for all inpatients? Is there evidence on every unit that there is discharge planning activities? Are staff following the discharge planning P&P? Is there a discharge planning process for certain categories of outpatients such as observation, ED patients and same day surgery patients? Could add questions to the assessment tool and include in questions asked in pre-admission tests for OP surgery

149
Discharge Planning Worksheet
For patients not initially identified as in need of discharge plan, is there a process for updating this based on changes in a patient’s condition? Many hospitals have the nurse doing the admission assessment ask a set of predetermined questions to see if assistance is needed How do you update this when there is a change? Is a discharge plan prepared for each inpatient? Does hospital have a process for notifying patients they can request a discharge planning evaluation? Or process for the patient representative to request

150
Discharge Planning Worksheet
Surveyor will interview patient to see if they were aware they could request a discharge planning evaluation Can the hospital show that they gave the patient a notice of their rights? Will interview doctors and make sure they know they can request a discharge planning evaluation (819 and 806) If doctor not aware will ask hospital to provide evidence on how it informs the MS about this
 If doctor not aware will ask hospital to provide evidence on how it informs the MS about this.")
151
Discharge Planning Worksheet
Will ask staff to describe the process for physicians to order a discharge plan Does P&P provide a process for ongoing reassessment of discharge plan in case of changes to the patient’s condition (819)? Does hospital review discharge planning process on an ongoing manner Removed section that said at least quarterly How often does your hospital do this?
 Does hospital review discharge planning process on an ongoing manner. Removed section that said at least quarterly. How often does your hospital do this")
152
Discharge Planning Worksheet
Does hospital track readmission rates as part of discharge planning? Does assessment include if readmission was potentially preventable? If preventable then did the hospital make changes to the planning process? Does hospital collect feedback from post-acute providers for effectiveness of the hospital’s discharge planning process? This would include places like LTC, assisted living or home health agencies

153
Discharge Planning Tracers
Has a discharge planning tracer section 4 Surveyors is to interview one or two inpatients Surveyor is to review the closed medical record of two or three patients who was discharged Will try and include one patient who was readmitted within 30 days Will mark worksheet to show if it was an interview, discharge planning document review, medical record review or other document that was reviewed

155
Discharge Planning Tracers
Was the screening done to identify if the inpatient needed a discharge planning evaluation? Includes at the time of admission, after an admission but at least 48 hours prior to discharge, or N?A In some hospitals all patients get a discharge plan Can staff demonstrate that the hospital’s criteria and screening process for discharge evaluation were correctly applied (800)? Was discharge planning evaluation done by qualified person (SW, RN) as defined in the P&P?
 Was discharge planning evaluation done by qualified person (SW, RN) as defined in the P&P")
156
Discharge Planning Tracers
Are the results of the discharge planning evaluation documented in the chart? Did the evaluation include an assessment of the patients post-discharge care needs? Patient need home health referral Patient needs bedside commode Patient needs home oxygen Patient needs post hospital physical therapy Meals on wheels, etc.

157
Discharge Planning Tracers
Did the evaluation include an assessment of: Patient’s ability to perform ADL (feeding, personal hygiene, ambulation, etc.)? Family support and ability to do self care? Whether patient will need specialized medical equipment or modifications to their home? Is support person or family able to meet the patient’s needs and assessment of community resources ? Was patient given a list of HHA or LTC facilities in the community and must be documented in the record and the list appropriate
 Family support and ability to do self care Whether patient will need specialized medical equipment or modifications to their home Is support person or family able to meet the patient’s needs and assessment of community resources Was patient given a list of HHA or LTC facilities in the community and must be documented in the record and the list appropriate.")
158
Discharge Planning Tracers To LTC
Separate set of questions if patient admitted from LTC or assisted living Did evaluation include if LTC has capacity for patient to go back there? Does it include assessment if insurance coverage will cover it if they go back there? Was the discharge planning evaluation timely to allow for arrangements if the patient needs to go back there Was the patient’s representative involved in these discussions? Discharge plan needs to match the patient’s needs (811, 130)
")
159
Discharge Planning Tracers
If patient discharged home is their initial implementation of the discharge plan? Did staff provide training to patient including recognized methods such as teach back? Were the written discharge instructions legible and use non-technical language (low health literacy) Was a list of all medication patient will take after discharge given with a clear indication of any changes? TJC revised their 5 EPs on medication reconciliation July 1, 2011
 Was a list of all medication patient will take after discharge given with a clear indication of any changes TJC revised their 5 EPs on medication reconciliation July 1,")
160
Medication List

161
Discharge Planning Tracers
Will look for evidence of hospital of patients and support persons Was patient referred back for follow up with their PCP or a health center? Was there a referral to PT, mental health, hospice, OT etc. as needed? Was there a referral for community based resources such as transportation services, Department of Aging, elder services etc.? Arranged for needed equipment such as oxygen, commode, wheel chair etc.

162
Discharge Planning Worksheet
If transferred to another inpatient facility was the discharge summary ready and sent with patient? Was discharge summary sent before first post-discharge appointment or within 7 days of discharge? Was follow up appointment scheduled? Was there documentation in the medical record of results of tests pending at the time of discharge both to the patient and the post hospital provider? Was patient readmitted within 30 days?

163
Appointments for Follow Up

164
Outstanding Labs or Tests

165
Patient Discharge Plan

166
Discharge Planning Tracers
Will look to make sure these were done and did not delay discharge Scheduling follow-up appointments Filling prescriptions Pharmacist meeting with patient and/or family/support persons to review medication regimen Pharmacist reviewing discharge medication orders prior to hospital departure

167
Discharge Planning Tracers
Will look to make sure these were done and did not delay discharge (continued): Home setting visitation by hospital staff Transportation arranged for follow-up appointments Discharge planning checklists, e.g. CMS, AHRQ, CAPS checklists Note CMS has one for patients and PaPSA and hospitalists have a checklist for physicians and staff
: Home setting visitation by hospital staff. Transportation arranged for follow-up appointments. Discharge planning checklists, e.g. CMS, AHRQ, CAPS checklists. Note CMS has one for patients and PaPSA and hospitalists have a checklist for physicians and staff.")
168
CMS Your Discharge Planning Checklist

170
Two Discharge Check Lists
This lead to the development of a formal discharge checklist to ensure communication at discharge Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. Halasyamani L, Kripalani S, Coleman E, et al. J Hosp Med. 2006;1: The Pa Patient Safety Authority has excellent resources including suggested elements for a discharge checklist See Care at discharge—a critical juncture for transition to post hospital care. Pa Pat Saf Advis 2008 Jun;5(2):39-43
:")
171
PaPSA Checklist

172
See Society of Hospital Medicine at http://www. hospitalmedicine

173
The End! Questions??? Sue Dill Calloway RN, Esq
AD, BA, BSN, MSN, JD CPHRM President of Patient Safety and Health Care Consulting Chief Learning Officer of the Emergency Medicine Foundation Dublin, Ohio 43017

Similar presentations


























 Grants Chapter 6.>")
 Changes Iowa Medicaid Enterprise October 14, 2008.>")