Download presentation
Presentation is loading. Please wait.

1
Incretin Based Therapy of Type 2 Diabetes Mellitus
BY Prof. ADEL A EL-SAYED MD Prof. of Internal Medicine Sohag Faculty of Medicine SOHAG EGYPT

2
Pathophysiology of Type 2 Diabetes
Insulin resistance. Beta cell dysfunction.

3
Pathophysiology of Type 2 Diabetes Insulin Resistance
Insulin Resistance starts very early in the course of the disease. insulin resistance alone will not produce diabetes. If beta-cell function is normal, one can compensate for insulin resistance by increasing insulin secretion.

4
Pathophysiology of Type 2 Diabetes Beta cell defect
all type 2 patients have at least a relative defect in both beta-cell function and mass. Function: in the (UKPDS), newly diagnosed people with diabetes had, on average, only about 50% of normal beta-cell function.[Diabetes. 1995;44: , Diab Res Clin Pract. 1998;40(suppl):S21-S25.] Mass: Autopsy studies comparing the volume of beta cells in nondiabetic individuals with that of people with diabetes found a 41% decrease in beta-cell mass among people with type 2 diabetes
, newly diagnosed people with diabetes had, on average, only about 50% of normal beta-cell function.[Diabetes. 1995;44: , Diab Res Clin Pract. 1998;40(suppl):S21-S25.] Mass: Autopsy studies comparing the volume of beta cells in nondiabetic individuals with that of people with diabetes found a 41% decrease in beta-cell mass among people with type 2 diabetes.")
5
Pathophysiology of Type 2 Diabetes Beta cell defect
IV glucose infusion to a nondiabetic individual results in a biphasic insulin response: - Immediate first-phase insulin response in the first few minutes. - Second-phase response, more prolonged.

6
Pathophysiology of Type 2 Diabetes Beta cell defect
This first-phase insulin response is absent in type 2 diabetic patients contributing to the excessive and prolonged glucose rise after a meal in those with diabetes Diabetologia. 2004;47(suppl 1):A279. Infusing insulin can only partially improve this condition.
:A279. Infusing insulin can only partially improve this condition.")
7
Pathophysiology of Type 2 Diabetes Other Factors
Historically, hyperglycemia in diabetes has been viewed as a failure of insulin-mediated glucose disposal into muscle and adipose tissue. This looks to be an over simplification of a more complicated issue.

8
Pathophysiology of Type 2 Diabetes Other Factors
Two other factors: - Glucagon. - Gastric emptying.

9
Pathophysiology of Type 2 Diabetes The Glucagon Factor
In response to a carbohydrate-containing meal, individuals without diabetes not only increase insulin secretion but also simultaneously decrease pancreatic alpha-cell glucagon secretion. The decrease in glucagon is associated with a decrease in hepatic glucose production, and along with the insulin response, results in a very modest increase in postprandial glucose. N Engl J Med. 1971;285:

10
Pathophysiology of Type 2 Diabetes The Glucagon Factor
In contrast, the glucagon secretion in type 2 diabetics is not decreased, and may even be paradoxically increased. These insulin and glucagon abnormalities produce an excessive postprandial glucose excursion. more than 35 years ago, Roger Unger presciently stated, "One wonders if the development of a pharmacologic means of suppressing glucagon to appropriate levels would increase the effectiveness of available treatments for diabetes”. N Engl J Med. 1971;285:

12
Pathophysiology of Type 2 Diabetes The Gastric Emptying Factor
Many factors can affect the rate of gastric emptying. studies suggest that all other factors being equal, most people with type 1 and type 2 diabetes have accelerated gastric emptying compared to those without diabetes. Gastroenterology. 1990;98:A378.

13
Pathophysiology of Type 2 Diabetes One last observation
In 1930 La Barre described a greater effect of oral rather parenteral glucose in increasing insulin secretion. In 1986 Nauck demonstrated that a glucose infusion graded to achieve plasma glucose levels identical o those achieved with oral glucose led to a insulin response that was only one quarter as great. J Clin Endocrinol Metab. 1986;63: Incretin hormones were discovered during researchers trials to find out interpretation to this phenomenon which has been called the incretin effect.

14
What are incretins? Hormones produced by the gastrointestinal tract in response to incoming nutrients, and have important actions that contribute to glucose homeostasis. Two hormones: - Gastric inhibitory polypeptide (GIP) Glucagon-like peptide-1 (GLP-1).
 . - Glucagon-like peptide-1 (GLP-1).")
15
What are incretins? Gastric Inhibitory Polypeptide (GIP)
Secreted by the K cells of the proximal gut. However, type 2 diabetes patients are resistant to its action (high blood level), making it a less attractive therapeutic target.
, making it a less attractive therapeutic target.")
16
What are incretins? Glucagon-like peptide-1 (GLP-1)
a 30-amino acid peptide secreted in response to the oral ingestion of nutrients by L cells, primarily in the ileum and colon. There are GLP-1 receptors in islet cells and in the central nervous system, among other places. GLP-1 is metabolized by the enzyme dipeptidyl peptidase-IV (DPP-IV) .
 .")
17
Actions of GLP-1 It enhances glucose-dependent insulin secretion.
Inhibits glucagon secretion and therefore hepatic glucose production. Slows gastric emptying. Increases satiety resulting in less food intake. Appears to stimulate insulin gene transcription and insulin synthesis.

18
Actions of GLP-1 In animal studies it increases beta-cell mass by:
- Decreasing beta cell apoptosis. - Stimulating the growth of new beta cells. Diabetes Care. 2003;26: ???... Long term benefit in reversing the progressive insulin deficiency.

19
Actions of GLP-1 Important, as glucose levels approach the normal range, the GLP-1 effects on insulin stimulation and glucagon inhibition declined (glucose dependence - reduction of hypoglycemia. - therapeutic advantage) Diabetologia. 1993;36:
 Diabetologia. 1993;36:")
21
Actions of GLP-1 The Problem
Unfortunately, GLP-1 is rapidly broken down by the DPP-IV enzyme (very short half-life in plasma - requires continuous IV infusion).
.")
22
The solution Two options:
Incretin mimetics are glucagon-like peptide-1 (GLP-1) agonists. Dipeptidyl peptidase-IV (DPP-IV) antagonists inhibit the breakdown of GLP-1.
 agonists. Dipeptidyl peptidase-IV (DPP-IV) antagonists inhibit the breakdown of GLP-1.")
23
Incretin mimetics Exenatide
The first incretin-related therapy available for patients with type 2 diabetes. Naturally occurring peptide from the saliva of the Gila Monster. Has an approximate 50% amino acid homology with GLP-1. Binds to GLP-1 receptors and behaves as GLP-1.

25
Incretin mimetics Exenatide
Resistant to DPP-IV inactivation. Following injection, it is measurably present in plasma for up to 10 hours. Suitable for twice a day administration by subcutaneous injection. Regul Pept. 2004;117:77-88. Am J Health Syst Pharm. 2005;62:

27
Clinical Trials of Exenatide
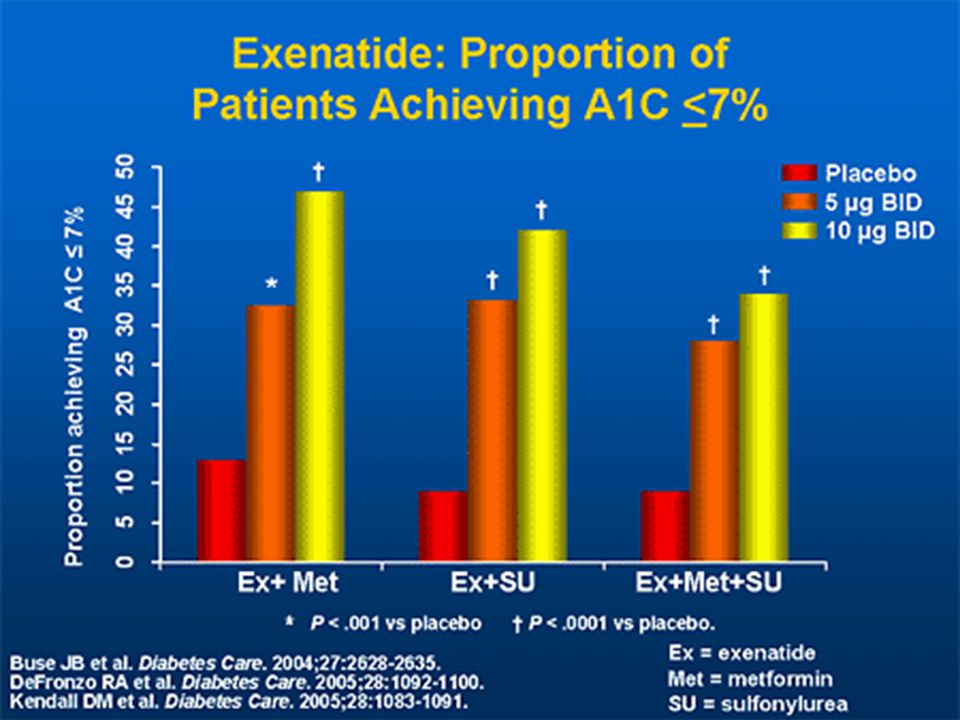
Three pivotal randomized, double-blind, placebo-controlled, multicenter clinical trials were conducted to support the approval of exenatide (the AMIGO studies). patients with type 2 diabetes who had not achieved adequate glycemic control despite treatment with metformin, a sulfonylurea, or the combination of metformin and a sulfonylurea. Patients were randomized to two well matched groups to receive either placebo or exenatide (5 and 10 (mcg) twice daily by subcutaneous injection).
. patients with type 2 diabetes who had not achieved adequate glycemic control despite treatment with metformin, a sulfonylurea, or the combination of metformin and a sulfonylurea. Patients were randomized to two well matched groups to receive either placebo or exenatide (5 and 10 (mcg) twice daily by subcutaneous injection).")
29
Weight Loss With Exenatide
After adding exenatide: the group that was on metformin alone lost about 3 kg of body weight at 30 weeks, while the sulfonylurea group experienced a 1.5- to 2-kg weight reduction. Patients receiving metformin and a sulfonylurea in combination along with exenatide lost an average of 2 kg. Weight loss of up to 10 kg has been documented, but it varies from person to person. recently published findings have shown progressive weight loss continuing for 82 weeks. Patients convenience Diabetes Care. 2004;27: , 2005;28: , 2005;28: Diabetes, Obesity and Metabolism. 2006; 8(4):436; ISSN: 4.
:436; ISSN: 4.")
30
Nausea With Exenatide was seen uniformly across the clinical trials, although most episodes were mild-to-moderate in intensity and generally intermittent. more frequent at the initiation of treatment and decreased over the course of several weeks.

31
Incretin mimetics Recent Advances
Liraglutide: Another GLP-1 analog with longer half-life, similar to exenatide with once-daily injection. Diabetes Care. 2007;30: Long acting exenatide: Highly effective with once weekly injection. Diabetes Care. 2007;30:

32
Dipeptidyl Peptidase-IV Antagonists
The concept is to allow the endogenous GLP-1 to remain in circulation for a longer period. DPP-IV inhibitors are oral, rather than injectable. Weight neutral. associated with a low incidence of hypoglycemia or gastrointestinal side effects. Diabetes Care. 2004;27: Preliminary long-term studies suggest a durable effect on glycemia and improvement in some parameters of beta-cell function. (

34
Dipeptidyl Peptidase-IV Antagonists Sitagliptin and Vildagliptin
Sitagliptin and vildagliptin are the first agents in this class to have received FDA approval. Incidence of adverse reactions was reported to be very low in a pooled safety data from 5141 patients. ADA meeting, Chicago, June 2007. They are indicated as monotherapy and in combination with metformin, thiazolidinediones and insulin. They look to be at least weight neutral.

35
Dipeptidyl Peptidase-IV Antagonists Recent Advances
During the last ADA meeting in Chicago, Illiois, June 2007, fifty-five presentations addressed 12 different DPP-IV inhibitors and “… more will be seen during the coming months…” Some members seem particularly interesting as saxagliptin (? potent) and alogliptin (long acting… ? Better affecting fasting glucose).
 and alogliptin (long acting… Better affecting fasting glucose).")
36
Summary Insulin resistance and relative insulin secretory defect are key elements of the pathogenesis of type 2 diabetes. GLP-1 deficiency is another key component in diabetic pathophysiology contributing to: - insulin secretory deficit. - excess of plasma glucagon. - postprandial hyperglycemia.

37
Summary Incretin mimetics offer a new approach in the management of type 2 diabetes. Exenatide is the first agent in this class and is administered via injection twice a day. In addition to improving glycemic control, exenatide has the unique benefit of causing weight loss that appears to be prolonged based on initial studies.

38
Summary DPP-IV inhibitors raise GLP-1 levels 2- to 3-fold.
They appear to be weight neutral and have a remarkable low incidence of adverse reactions. Sitagliptin ad vildagliptin are the first of the DPP-IV inhibitors to receive FDA approval. these promising new therapies should be undertaken in combination not only with existing oral antidiabetes medications as indicated, but also with other proven cardiovascular risk-reduction strategies, including lifestyle reduction and pharmacologic therapy, as needed.

40
THANK YOU

Similar presentations










 ELISA ‘Total Amide’ ‘Active’.>")
 + GIP = incretin effect =Augmentation of insulin after oral glucose Type 2 diabetics little incretin effect Reduced GLP-1 secretion.>")
 HbA1c – IFFC (mmol/mol) 6.042 6.548 7.053 7.559 8.064 9.075.>")












