Download presentation
Presentation is loading. Please wait.

1
Donald E Low University of Toronto
Bacterial Pathogens in the Hospital and Community: The Need for Newer Antibiotics Donald E Low University of Toronto 1

2
1900 U.S. life expectancy 1900-1960 life expectancy Year 70 62 54 46
38 This decline resulted in a sharp drop in infant and child mortality and 30 year increase in life expectancy 1900 1910 1920 1930 1940 1950 1960 Year

3
4/6/2017 3 In 1900, the three leading causes of death were pneumonia, tuberculosis (TB), and diarrhea and enteritis, which (together with diphtheria) caused one third of all deaths (Figure 2). Of these deaths, 40% were among children aged less than 5 years (1). In 1997, heart disease and cancers accounted for 54.7% of all deaths, with 4.5% attributable to pneumonia, influenza, and human immunodeficiency virus (HIV) infection (2). Despite this overall progress, one of the most devastating epidemics in human history occurred during the 20th century: the 1918 influenza pandemic that resulted in 20 million deaths, including 500,000 in the United States, in less than 1 year--more than have died in as short a time during any war or famine in the world (3). HIV infection, first recognized in 1981, has caused a pandemic that is still in progress, affecting 33 million people and causing an estimated 13.9 million deaths (4). These episodes illustrate the volatility of infectious disease death rates and the unpredictability of disease emergence. MMWR (29); 621
, and diarrhea and enteritis, which (together with diphtheria) caused one third of all deaths (Figure 2). Of these deaths, 40% were among children aged less than 5 years (1). In 1997, heart disease and cancers accounted for 54.7% of all deaths, with 4.5% attributable to pneumonia, influenza, and human immunodeficiency virus (HIV) infection (2). Despite this overall progress, one of the most devastating epidemics in human history occurred during the 20th century: the 1918 influenza pandemic that resulted in 20 million deaths, including 500,000 in the United States, in less than 1 year--more than have died in as short a time during any war or famine in the world (3). HIV infection, first recognized in 1981, has caused a pandemic that is still in progress, affecting 33 million people and causing an estimated 13.9 million deaths (4). These episodes illustrate the volatility of infectious disease death rates and the unpredictability of disease emergence. MMWR (29); 621.")
4
4/6/2017 4 This decline contributed to a sharp drop in infant and child mortality (1,2) and to the 29.2-year increase in life expectancy (2). In 1900, 30.4% of all deaths occurred among children aged less than 5 years; in 1997, that percentage was only 1.4%. In 1900, the three leading causes of death were pneumonia, tuberculosis (TB), and diarrhea and enteritis, which (together with diphtheria) caused one third of all deaths (Figure 2). Of these deaths, 40% were among children aged less than 5 years (1). In 1997, heart disease and cancers accounted for 54.7% of all deaths, with 4.5% attributable to pneumonia, influenza, and human immunodeficiency virus (HIV) infection (2). Despite this overall progress, one of the most devastating epidemics in human history occurred during the 20th century: the 1918 influenza pandemic that resulted in 20 million deaths, including 500,000 in the United States, in less than 1 year--more than have died in as short a time during any war or famine in the world (3). HIV infection, first recognized in 1981, has caused a pandemic that is still in progress, affecting 33 million people and causing an estimated 13.9 million deaths (4). These episodes illustrate the volatility of infectious disease death rates and the unpredictability of disease emergence. MMWR (29); 621
 and to the 29.2-year increase in life expectancy (2). In 1900, 30.4% of all deaths occurred among children aged less than 5 years; in 1997, that percentage was only 1.4%. In 1900, the three leading causes of death were pneumonia, tuberculosis (TB), and diarrhea and enteritis, which (together with diphtheria) caused one third of all deaths (Figure 2). Of these deaths, 40% were among children aged less than 5 years (1). In 1997, heart disease and cancers accounted for 54.7% of all deaths, with 4.5% attributable to pneumonia, influenza, and human immunodeficiency virus (HIV) infection (2). Despite this overall progress, one of the most devastating epidemics in human history occurred during the 20th century: the 1918 influenza pandemic that resulted in 20 million deaths, including 500,000 in the United States, in less than 1 year--more than have died in as short a time during any war or famine in the world (3). HIV infection, first recognized in 1981, has caused a pandemic that is still in progress, affecting 33 million people and causing an estimated 13.9 million deaths (4). These episodes illustrate the volatility of infectious disease death rates and the unpredictability of disease emergence. MMWR (29); 621.")
5
Achievements in 20th Century
4/6/2017 5 Achievements in 20th Century Control of infectious diseases Sanitation and Hygiene Vaccination Antibiotics

7
So What Happened? Attitudinal

8
Antibiotics: the epitome of a wonder drug
4/6/2017 8 Antibiotics: the epitome of a wonder drug The introduction of antibiotics in the 1940s converted illness into a strictly technical problem: "virtual elimination of infectious disease as a significant factor in social life." Burnet FM. Natural history of infectious disease. 2nd ed. Cambridge: Cambridge University Press, 1953

9
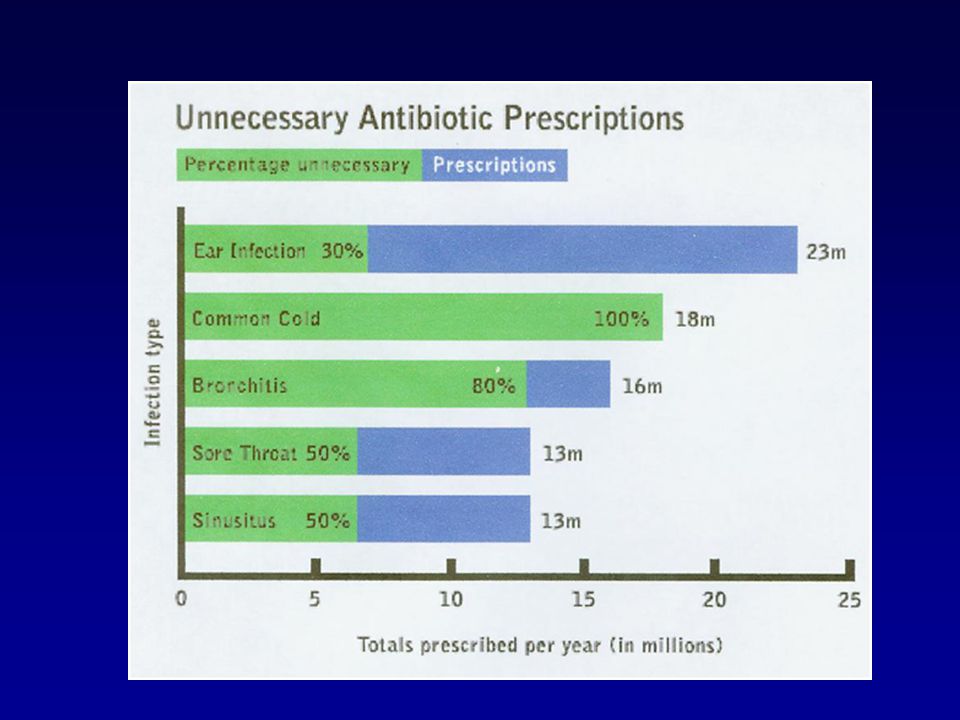
So What Happened? Attitudinal Antibiotic overuse/misuse

11
So What Happened? Attitudinal Antibiotic overuse/misuse
Fitness of organisms clonal spread

12
Spain 23F – one pneumococcal clone
4/6/2017 12 Spain 23F – one pneumococcal clone Finland France BM4200 1978 ? Cleveland Spain South Korea Tennessee Mexico Taiwan Hong Kong Philippines Thailand Colombia The spread of resistant bacteria. Present data on the spread of resistant bacteria: · Between countries - the 23f pneumococcus: clonal spread Malaysia Singapore Brazil Chile South Africa Uruguay Argentina

13
Global Travel and World Population
4/6/2017 13 Global Travel and World Population

14
Bad Bugs, No Drugs1 The Antimicrobial Availability Task Force of the IDSA1 identified as particularly problematic pathogens A. baumannii and P. aeruginosa ESBL-producing Enterobacteriaceae MRSA Vancomycin-resistant enterococcus Declining research investments in antimicrobial development2 1. Infectious Diseases Society of America. Bad Bugs, No Drugs: As Antibiotic Discovery Stagnates, A Public Health Crisis Brews. July, Accessed March 17, Talbot GH, et al. Clin Infect Dis. 2006;42:

15
Between 1962 and 2000, no major classes of antibiotics were introduced
Fischbach MA and Walsh CT Science 2009

16
A Changing Landscape for Numbers of Approved Antibacterial Agents
2 4 6 8 10 12 14 16 18 Number of agents approved Resistance 2008 Bars represent number of new antimicrobial agents approved by the FDA during the period listed. Infectious Diseases Society of America. Bad Bugs, No Drugs. July 2004; Spellberg B et al. Clin Infect Dis. 2004;38: ; New antimicrobial agents. Antimicrob Agents Chemother. 2006;50:1912

17
The Problems Gram negatives Gram positives
Resistant Enterobacteriaceae β-Lactamases Pseudomonas/Acinetobacter N. gonorrheae Gram positives MRSA Pneumococcus

18
The Gram Negatives

19
Prevalence of Isolates of Multidrug-Resistant Gram Negative Rods Recovered Within The First 48 h After Admission to the Hospital Background. The prevalence of multidrug resistance (MDR) among gram-negative bacilli is rapidly increasing. Quantification of the prevalence and the common antimicrobial coresistance patterns of MDR gram-negative bacilli (MDR-GNB) isolates recovered from patients at hospital admission, as well as identification of patients with a high risk of harboring MDR-GNB, would have important implications for patient care. Methods. Over a 6-year period, patients who harbored MDR-GNB (i.e., patients who had MDR-GNB isolates recovered from clinical cultures within the first 48 h after hospital admission) were identified. "MDR-GNB isolates" were defined as Pseudomonas aeruginosa, Escherichia coli, Enterobacter cloacae, and Klebsiella species isolates with resistance to at least 3 antimicrobial groups. A case-control study was performed to determine the independent risk factors for harboring MDR-GNB at hospital admission. Results. Between 1998 and 2003, the prevalence of MDR-GNB isolates recovered from patients at hospital admission increased significantly for all isolate species (P < .001), with the exception of P. aeruginosa (P = .09). Of 464 MDR-GNB isolates, 12%, 35%, and 53% of isolates were coresistant to 5, 4, and 3 antimicrobial groups, respectively. Multivariable analysis identified age 65 years (odds ratio [OR], 2.8; 95% confidence interval [CI], ; P < .04), prior exposure to antibiotics for 14 days (OR, 8.7; 95% CI, ; P < .001), and prior residence in a long-term care facility (OR, 3.5; 95% CI, ; P < .01) as independent risk factors for harboring MDR-GNB at hospital admission. Conclusion. A substantial number of patients harbor MDR-GNB at hospital admission. Identification of common coresistance patterns among MDR-GNB isolates may assist in the selection of empirical antimicrobial therapy for patients with a high risk of harboring MDR-GNB Pop-Vicas and D'Agata CID 2005;40:
 among gram-negative bacilli is rapidly increasing. Quantification of the prevalence and the common antimicrobial coresistance patterns of MDR gram-negative bacilli (MDR-GNB) isolates recovered from patients at hospital admission, as well as identification of patients with a high risk of harboring MDR-GNB, would have important implications for patient care. Methods. Over a 6-year period, patients who harbored MDR-GNB (i.e., patients who had MDR-GNB isolates recovered from clinical cultures within the first 48 h after hospital admission) were identified. MDR-GNB isolates were defined as Pseudomonas aeruginosa, Escherichia coli, Enterobacter cloacae, and Klebsiella species isolates with resistance to at least 3 antimicrobial groups. A case-control study was performed to determine the independent risk factors for harboring MDR-GNB at hospital admission. Results. Between 1998 and 2003, the prevalence of MDR-GNB isolates recovered from patients at hospital admission increased significantly for all isolate species (P < .001), with the exception of P. aeruginosa (P = .09). Of 464 MDR-GNB isolates, 12%, 35%, and 53% of isolates were coresistant to 5, 4, and 3 antimicrobial groups, respectively. Multivariable analysis identified age 65 years (odds ratio [OR], 2.8; 95% confidence interval [CI], ; P < .04), prior exposure to antibiotics for 14 days (OR, 8.7; 95% CI, ; P < .001), and prior residence in a long-term care facility (OR, 3.5; 95% CI, ; P < .01) as independent risk factors for harboring MDR-GNB at hospital admission. Conclusion. A substantial number of patients harbor MDR-GNB at hospital admission. Identification of common coresistance patterns among MDR-GNB isolates may assist in the selection of empirical antimicrobial therapy for patients with a high risk of harboring MDR-GNB. Pop-Vicas and D Agata CID 2005;40:")
20
Enterobacteriaceae The rapid and disturbing spread of:
extended-spectrum ß-lactamases AmpC enzymes carbapenem resistance metallo-β-lactamases KPC and OXA-48 β-lactamases quinolone resistance

21
Rise in the proportions of E
Rise in the proportions of E. coli from bacteraemias in England, Wales and Northern Ireland resistant to fluoroquinolones (white), oxyimino-cephalosporins (grey) and both (black) Oxyimino cephs: cefotaxime, ceftazidime, ceftriaxone, cefuroxime, and cefepime Livermore, D. M. J. Antimicrob. Chemother :i29-36i; doi: /jac/dkp255 Copyright restrictions may apply.
, oxyimino-cephalosporins (grey) and both (black) Oxyimino cephs: cefotaxime, ceftazidime, ceftriaxone, cefuroxime, and. cefepime. Livermore, D. M. J. Antimicrob. Chemother :i29-36i; doi: /jac/dkp255. Copyright restrictions may apply.")
22
Increase in numbers of Group 1, 2 and 3 β-lactamases from 1970 to 2009
Group 2/class A and class D β-lactamases Group 1/class C cephalosporinases Group 3/class B metallo- β-lactamases Group 2 (Class A and D) inhibitor-resistant and extended-spectrum β-lactamases, and serine carbapenemases Bush K and Jacoby G AAC 2010
 inhibitor-resistant and extended-spectrum β-lactamases, and serine carbapenemases. Bush K and Jacoby G AAC")
23
Major families of β-lactamases of clinical importance
Group 1 cephalosporinases. Group 1 enzymes are cephalosporinases belonging to molecular class C that are encoded on the chromosome of many Enterobacteriaceae and a few other organisms (27). They are more active on cephalosporins than benzylpenicillin and are usually resistant to inhibition by clavulanic acid and active on cephamycins, such as cefoxitin. When produced in large amounts, especially in a host with reduced β–lactam accumulation, group 1 enzymes can provide resistance to carbapenems, especially ertapenem Group 2 serine β-lactamases. Functional Group 2, including molecular classes A and D, β-lactamases represent the largest group of β-lactamases, due primarily to the increasing identification of ESBLs during the past 20 years. TEM and SHV ESBLs have been joined by the functionally similar but more rapidly proliferating CTX-M enzymes that are related to chromosomally determined β-lactamases in species of Kluyvera (8). As the name implies, most (but not all) CTX-M enzymes hydrolyze cefotaxime more readily than ceftazidime. Many hydrolyze cefepime as well. Serine carbapenemases from molecular class A populate subgroup 2f. More worrisome, however, are the plasmid-encoded subgroup 2f β-lactamases including KPC and some GES (formerly IBC) enzymes. The KPC carbapenemases in particular have recently been associated with major outbreaks of multidrug-resistant gram-negative infections in hospitals including those in the New York City metropolitan area (10, 12, 70) and in Israel (32), with their spread now becoming worldwide Bush K and Jacboy G AAC 2010
. They are more active on cephalosporins than benzylpenicillin and are usually resistant to inhibition by clavulanic acid and active on cephamycins, such as cefoxitin. When produced in large amounts, especially in a host with reduced β–lactam accumulation, group 1 enzymes can provide resistance to carbapenems, especially ertapenem. Group 2 serine β-lactamases. Functional Group 2, including molecular classes A and D, β-lactamases represent the largest group of β-lactamases, due primarily to the increasing identification of ESBLs during the past 20 years. TEM and SHV ESBLs have been joined by the functionally similar but more rapidly proliferating CTX-M enzymes that are related to chromosomally determined β-lactamases in species of Kluyvera (8). As the name implies, most (but not all) CTX-M enzymes hydrolyze cefotaxime more readily than ceftazidime. Many hydrolyze cefepime as well. Serine carbapenemases from molecular class A populate subgroup 2f. More worrisome, however, are the plasmid-encoded subgroup 2f β-lactamases including KPC and some GES (formerly IBC) enzymes. The KPC carbapenemases in particular have recently been associated with major outbreaks of multidrug-resistant gram-negative infections in hospitals including those in the New York City metropolitan area (10, 12, 70) and in Israel (32), with their spread now becoming worldwide. Bush K and Jacboy G AAC")
24
Extended-Spectrum β-Lactamases
β-lactamases capable of conferring bacterial resistance to the penicillins first-, second-, and third-generation cephalosporins aztreonam (but not the cephamycins or carbapenems) These enzymes are derived from group 2b β-lactamases (TEM-1, TEM-2, and SHV-1) differ from their progenitors by as few as one AA
 These enzymes are derived from group 2b β-lactamases (TEM-1, TEM-2, and SHV-1) differ from their progenitors by as few as one AA.")
25
25

26
CTX-M-type ESBLs Until 2000, most ESBL producers were hospital Klebsiella spp. with TEM and SHV mutant β-lactamases Now, the dominant ESBLs across most of Europe and Asia are CTX-M enzymes, which originated as genetic escapes from Kluyvera spp Currently recognized as the most widespread and threatening mechanism of antibiotic resistance, both in clinical and community settings 80% of ESBL-positive E. coli from bacteraemias in the UK and Ireland are resistant to fluoroquinolones 40% are resistant to gentamicin These enzymes were named for their greater activity against cefotaxime than other oxyimino-beta-lactam substrates (eg, ceftazidime, ceftriaxone, or cefepime). Rather than arising by mutation, they represent examples of plasmid acquisition of beta-lactamase genes normally found on the chromosome of species, a group of rarely pathogenic commensal organisms. These enzymes are not very closely related to TEM or SHV beta-lactamases in that they show only approximately 40% identity with these two commonly isolated beta-lactamases. More than 40 CTX-M enzymes are currently known. Despite their name, a few are more active on ceftazidime than cefotaxime. They have mainly been found in strains of Salmonella enterica serovar Typhimurium and E. coli, but have also been described in other species of Enterobacteriaceae and are the predominant ESBL type in parts of South America. (They are also seen in eastern Europe) CTX-M-14, CTX-M-3, and CTX-M-2 are the most widespread. CTX-M-15 is currently (2006) the most widespread type in E. coli the UK and is widely prevalent in the community.[11] Livermore, DM J. Antimicrob. Chemother 2009
. Rather than arising by mutation, they represent examples of plasmid acquisition of beta-lactamase genes normally found on the chromosome of species, a group of rarely pathogenic commensal organisms. These enzymes are not very closely related to TEM or SHV beta-lactamases in that they show only approximately 40% identity with these two commonly isolated beta-lactamases. More than 40 CTX-M enzymes are currently known. Despite their name, a few are more active on ceftazidime than cefotaxime. They have mainly been found in strains of Salmonella enterica serovar Typhimurium and E. coli, but have also been described in other species of Enterobacteriaceae and are the predominant ESBL type in parts of South America. (They are also seen in eastern Europe) CTX-M-14, CTX-M-3, and CTX-M-2 are the most widespread. CTX-M-15 is currently (2006) the most widespread type in E. coli the UK and is widely prevalent in the community.[11] Livermore, DM J. Antimicrob. Chemother")
27
Carbapenemases Ability to hydrolyze penicillins, cephalosporins, monobactams, and carbapenems Resilient against inhibition by all commercially viable ß-lactamase inhibitors Subgroup 2df: OXA (23 and 48) carbapenemases Subgroup 2f : serine carbapenemases from molecular class A: GES and KPC Subgroup 3b contains a smaller group of MBLs that preferentially hydrolyze carbapenems IMP and VIM enzymes that have appeared globally, most frequently in non-fermentative bacteria but also in Enterobacteriaceae
 carbapenemases. Subgroup 2f : serine carbapenemases from molecular class A: GES and KPC. Subgroup 3b contains a smaller group of MBLs that preferentially hydrolyze carbapenems. IMP and VIM enzymes that have appeared globally, most frequently in non-fermentative bacteria but also in Enterobacteriaceae.")
28
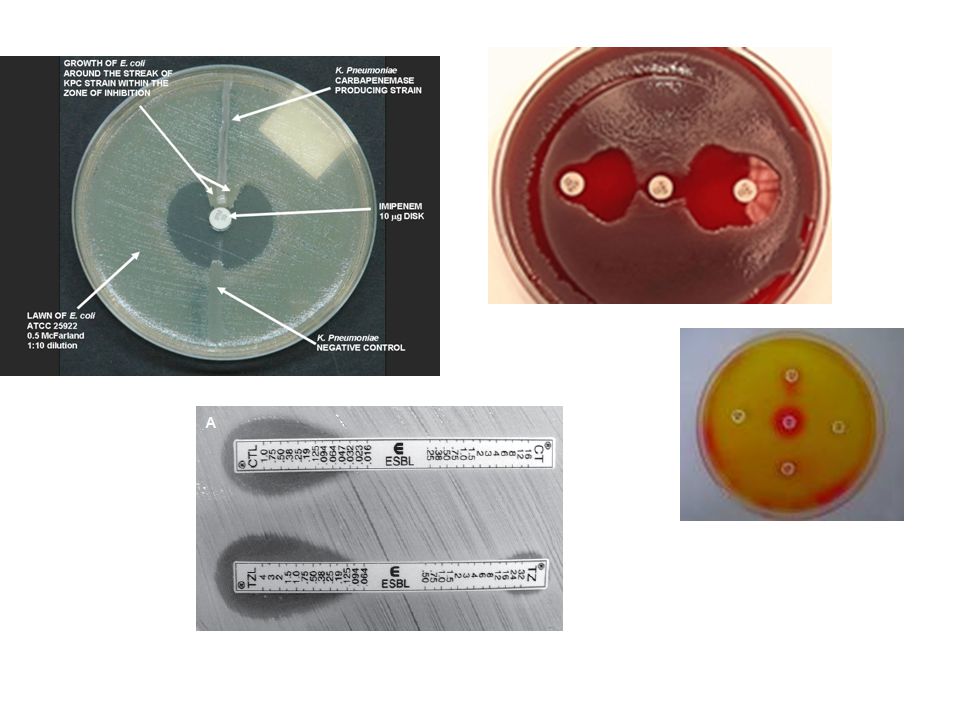
KPC (K. pneumoniae carbapenemase)
KPCs are the most prevalent of this group of enzymes, found mostly on transferable plasmids in K. pneumoniae Substrate hydrolysis spectrum includes cephalosporins and carbapenems A few class A enzymes, notably the plasmid-mediated KPC enzymes, are effective carbapenemases as well. Three variants are known, distinguished by one or two amino-acid substitutions. KPC-1 was found in North Carolina, KPC-2 in Baltimore and KPC-3 in New York. They have only 45% homology with SME and NMC/IMI enzymes and, unlike them, can be encoded by self-transmissible plasmids.

29
K. pneumoniae carbapenemase-producing bacteria
A few class A enzymes, notably the plasmid-mediated KPC enzymes, are effective carbapenemases as well. Three variants are known, distinguished by one or two amino-acid substitutions. KPC-1 was found in North Carolina, KPC-2 in Baltimore and KPC-3 in New York. They have only 45% homology with SME and NMC/IMI enzymes and, unlike them, can be encoded by self-transmissible plasmids. Nordmann P et al. LID 2009

30
Major families of β-lactamases of clinical importance
Group 1 cephalosporinases. Group 1 enzymes are cephalosporinases belonging to molecular class C that are encoded on the chromosome of many Enterobacteriaceae and a few other organisms (27). They are more active on cephalosporins than benzylpenicillin and are usually resistant to inhibition by clavulanic acid and active on cephamycins, such as cefoxitin. When produced in large amounts, especially in a host with reduced β–lactam accumulation, group 1 enzymes can provide resistance to carbapenems, especially ertapenem Group 2 serine β-lactamases. Functional Group 2, including molecular classes A and D, β-lactamases represent the largest group of β-lactamases, due primarily to the increasing identification of ESBLs during the past 20 years. TEM and SHV ESBLs have been joined by the functionally similar but more rapidly proliferating CTX-M enzymes that are related to chromosomally determined β-lactamases in species of Kluyvera (8). As the name implies, most (but not all) CTX-M enzymes hydrolyze cefotaxime more readily than ceftazidime. Many hydrolyze cefepime as well. Serine carbapenemases from molecular class A populate subgroup 2f. More worrisome, however, are the plasmid-encoded subgroup 2f β-lactamases including KPC and some GES (formerly IBC) enzymes. The KPC carbapenemases in particular have recently been associated with major outbreaks of multidrug-resistant gram-negative infections in hospitals including those in the New York City metropolitan area (10, 12, 70) and in Israel (32), with their spread now becoming worldwide Bush K and Jacboy G AAC 2010
. They are more active on cephalosporins than benzylpenicillin and are usually resistant to inhibition by clavulanic acid and active on cephamycins, such as cefoxitin. When produced in large amounts, especially in a host with reduced β–lactam accumulation, group 1 enzymes can provide resistance to carbapenems, especially ertapenem. Group 2 serine β-lactamases. Functional Group 2, including molecular classes A and D, β-lactamases represent the largest group of β-lactamases, due primarily to the increasing identification of ESBLs during the past 20 years. TEM and SHV ESBLs have been joined by the functionally similar but more rapidly proliferating CTX-M enzymes that are related to chromosomally determined β-lactamases in species of Kluyvera (8). As the name implies, most (but not all) CTX-M enzymes hydrolyze cefotaxime more readily than ceftazidime. Many hydrolyze cefepime as well. Serine carbapenemases from molecular class A populate subgroup 2f. More worrisome, however, are the plasmid-encoded subgroup 2f β-lactamases including KPC and some GES (formerly IBC) enzymes. The KPC carbapenemases in particular have recently been associated with major outbreaks of multidrug-resistant gram-negative infections in hospitals including those in the New York City metropolitan area (10, 12, 70) and in Israel (32), with their spread now becoming worldwide. Bush K and Jacboy G AAC")
31
AmpC β-lactamases Once expressed at high levels, confer resistance to many β-lactam antimicrobials (excluding cefepime and carbapenems) In E. coli, constitutive over expression of AmpC β-lactamases can occur because of mutations in the promoter and/or attenuator region (AmpC hyperproducers) the acquisition of a transferable ampC gene on a plasmid or other transferable elements (plasmid-mediated AmpC β-lactamases)
 the acquisition of a transferable ampC gene on a plasmid or other transferable elements (plasmid-mediated AmpC β-lactamases)")
32
Emerging Metallo-β-Lactamases with Mobile Genetics (SENTRY Program 2001-2005)
32

34
Enterobacteriaceae: Breakpoints revised
Agent CLSI 2009 CLSI 2010 S I R Cefazolin ≤8 16 ≥32 ≤1 2 ≥4 Cefotaxime 16-32 ≥64 Ceftriaxone Ceftazidime ≤4 8 ≥16 Aztreonam Cefipime

35
Neisseria gonorrhoeae
Wang SA et al. Ann Int Med 2008

36
Prevalence of and risk factors for quinolone-resistant Neisseria gonorrhoeae infection in Ontario
Oto KV et al. CMAJ 2009

37
Treatment of N. gonorrhoeae
Only current CDC-recommended options for treating N. gonorrhoeae infections are from a single class of antibiotics, the cephalosporins. Ceftriaxone, available only as an injection, is the recommended treatment for all types of gonorrhea infections (i.e., urogenital, rectal, and pharyngeal). Cefixime is the only oral agent recommended for treatment of uncomplicated urogenital or rectal gonorrhea Reduced susceptibility to cefixime being described in Japan and other countries
. Cefixime is the only oral agent recommended for treatment of uncomplicated urogenital or rectal gonorrhea. Reduced susceptibility to cefixime being described in. Japan and other countries.")
38
The Gram Positives Staphylococcus aureus MDR Streptococcus pneumoniae
MRSA Reduced-vancomycin susceptibility MRSA MDR Streptococcus pneumoniae

39
adapted from Klevens et al. JAMA I2007
MRSA DeLeo and Chambers JCI 2009 adapted from Klevens et al. JAMA I2007

41
Worldwide Prevalance of MRSA Among S. aureus Isolates
Grundmann H et al. Lancet 2006;368:874.

42
Community -Associated MRSA
Sports participants Inmates in correctional facilities Military recruits Children in daycare Native Americans, Alaskan Natives, Pacific Islanders Men who have sex with men Hurricane evacuees in shelters Foal watchers Rural crystal methamphetamine users 42

43
MRSA Infections Among Patients In The Emergency Department
Adult patients with acute, purulent skin and soft-tissue infections presenting to 11 University-affiliated EDs during August 2004 S. aureus was isolated from 320/422 patients 59% overall were MRSA (15% to 74%) 97% of MRSA were USA300 74% were a single strain (USA ) 98% of MRSA had SCCmec type IV and the PVL toxin gene Methicillin-resistant Staphylococcus aureus (MRSA) is increasingly recognized in infections among persons in the community without established risk factors for MRSA. We enrolled adult patients with acute, purulent skin and soft-tissue infections presenting to 11 university-affiliated emergency departments during the month of August Cultures were obtained, and clinical information was collected. Available S. aureus isolates were characterized by antimicrobial-susceptibility testing, pulsed-field gel electrophoresis, and detection of toxin genes. On MRSA isolates, we performed typing of the staphylococcal cassette chromosome mec (SCCmec), the genetic element that carries the mecA gene encoding methicillin resistance. S. aureus was isolated from 320 of 422 patients with skin and soft-tissue infections (76 percent). The prevalence of MRSA was 59 percent overall and ranged from 15 to 74 percent. Pulsed-field type USA300 isolates accounted for 97 percent of MRSA isolates; 74 percent of these were a single strain (USA ). SCCmec type IV and the Panton-Valentine leukocidin toxin gene were detected in 98 percent of MRSA isolates. Other toxin genes were detected rarely. Among the MRSA isolates, 95 percent were susceptible to clindamycin, 6 percent to erythromycin, 60 percent to fluoroquinolones, 100 percent to rifampin and trimethoprim-sulfamethoxazole, and 92 percent to tetracycline. Antibiotic therapy was not concordant with the results of susceptibility testing in 100 of 175 patients with MRSA infection who received antibiotics (57 percent). Among methicillin-susceptible S. aureus isolates, 31 percent were USA300 and 42 percent contained pvl genes. MRSA is the most common identifiable cause of skin and soft-tissue infections among patients presenting to emergency departments in 11 U.S. cities. When antimicrobial therapy is indicated for the treatment of skin and soft-tissue infections, clinicians should consider obtaining cultures and modifying empirical therapy to provide MRSA coverage. Nebraska 48% (n = 203) North Dakota 30% (n = 218) South Dakota 42% (n = 226) Wisconsin 21% (n = 198) Moran GJ et al. NEJM 2006; 355: 43
 97% of MRSA were USA % were a single strain (USA ) 98% of MRSA had SCCmec type IV and the PVL toxin gene. Methicillin-resistant Staphylococcus aureus (MRSA) is increasingly recognized in infections among persons in the community without established risk factors for MRSA. We enrolled adult patients with acute, purulent skin and soft-tissue infections presenting to 11 university-affiliated emergency departments during the month of August Cultures were obtained, and clinical information was collected. Available S. aureus isolates were characterized by antimicrobial-susceptibility testing, pulsed-field gel electrophoresis, and detection of toxin genes. On MRSA isolates, we performed typing of the staphylococcal cassette chromosome mec (SCCmec), the genetic element that carries the mecA gene encoding methicillin resistance. S. aureus was isolated from 320 of 422 patients with skin and soft-tissue infections (76 percent). The prevalence of MRSA was 59 percent overall and ranged from 15 to 74 percent. Pulsed-field type USA300 isolates accounted for 97 percent of MRSA isolates; 74 percent of these were a single strain (USA ). SCCmec type IV and the Panton-Valentine leukocidin toxin gene were detected in 98 percent of MRSA isolates. Other toxin genes were detected rarely. Among the MRSA isolates, 95 percent were susceptible to clindamycin, 6 percent to erythromycin, 60 percent to fluoroquinolones, 100 percent to rifampin and trimethoprim-sulfamethoxazole, and 92 percent to tetracycline. Antibiotic therapy was not concordant with the results of susceptibility testing in 100 of 175 patients with MRSA infection who received antibiotics (57 percent). Among methicillin-susceptible S. aureus isolates, 31 percent were USA300 and 42 percent contained pvl genes. MRSA is the most common identifiable cause of skin and soft-tissue infections among patients presenting to emergency departments in 11 U.S. cities. When antimicrobial therapy is indicated for the treatment of skin and soft-tissue infections, clinicians should consider obtaining cultures and modifying empirical therapy to provide MRSA coverage. Nebraska 48% (n = 203) North Dakota 30% (n = 218) South Dakota 42% (n = 226) Wisconsin 21% (n = 198) Moran GJ et al. NEJM 2006; 355:")
44
MRSA Infections Among Patients In The Emergency Department
Portland 54% Minneapolis 39% New York 15% Philadelphia 55% Charlotte 68% Phoenix 60% Kansas City 74% Los Angeles 51% Atlanta 72% Methicillin-resistant Staphylococcus aureus (MRSA) is increasingly recognized in infections among persons in the community without established risk factors for MRSA. We enrolled adult patients with acute, purulent skin and soft-tissue infections presenting to 11 university-affiliated emergency departments during the month of August Cultures were obtained, and clinical information was collected. Available S. aureus isolates were characterized by antimicrobial-susceptibility testing, pulsed-field gel electrophoresis, and detection of toxin genes. On MRSA isolates, we performed typing of the staphylococcal cassette chromosome mec (SCCmec), the genetic element that carries the mecA gene encoding methicillin resistance. S. aureus was isolated from 320 of 422 patients with skin and soft-tissue infections (76 percent). The prevalence of MRSA was 59 percent overall and ranged from 15 to 74 percent. Pulsed-field type USA300 isolates accounted for 97 percent of MRSA isolates; 74 percent of these were a single strain (USA ). SCCmec type IV and the Panton-Valentine leukocidin toxin gene were detected in 98 percent of MRSA isolates. Other toxin genes were detected rarely. Among the MRSA isolates, 95 percent were susceptible to clindamycin, 6 percent to erythromycin, 60 percent to fluoroquinolones, 100 percent to rifampin and trimethoprim-sulfamethoxazole, and 92 percent to tetracycline. Antibiotic therapy was not concordant with the results of susceptibility testing in 100 of 175 patients with MRSA infection who received antibiotics (57 percent). Among methicillin-susceptible S. aureus isolates, 31 percent were USA300 and 42 percent contained pvl genes. MRSA is the most common identifiable cause of skin and soft-tissue infections among patients presenting to emergency departments in 11 U.S. cities. When antimicrobial therapy is indicated for the treatment of skin and soft-tissue infections, clinicians should consider obtaining cultures and modifying empirical therapy to provide MRSA coverage. Albuquerque 60% New Orleans 67% Nebraska 48% (n = 203) North Dakota 30% (n = 218) South Dakota 42% (n = 226) Wisconsin 21% (n = 198) Moran GJ et al. NEJM : 44
 is increasingly recognized in infections among persons in the community without established risk factors for MRSA. We enrolled adult patients with acute, purulent skin and soft-tissue infections presenting to 11 university-affiliated emergency departments during the month of August Cultures were obtained, and clinical information was collected. Available S. aureus isolates were characterized by antimicrobial-susceptibility testing, pulsed-field gel electrophoresis, and detection of toxin genes. On MRSA isolates, we performed typing of the staphylococcal cassette chromosome mec (SCCmec), the genetic element that carries the mecA gene encoding methicillin resistance. S. aureus was isolated from 320 of 422 patients with skin and soft-tissue infections (76 percent). The prevalence of MRSA was 59 percent overall and ranged from 15 to 74 percent. Pulsed-field type USA300 isolates accounted for 97 percent of MRSA isolates; 74 percent of these were a single strain (USA ). SCCmec type IV and the Panton-Valentine leukocidin toxin gene were detected in 98 percent of MRSA isolates. Other toxin genes were detected rarely. Among the MRSA isolates, 95 percent were susceptible to clindamycin, 6 percent to erythromycin, 60 percent to fluoroquinolones, 100 percent to rifampin and trimethoprim-sulfamethoxazole, and 92 percent to tetracycline. Antibiotic therapy was not concordant with the results of susceptibility testing in 100 of 175 patients with MRSA infection who received antibiotics (57 percent). Among methicillin-susceptible S. aureus isolates, 31 percent were USA300 and 42 percent contained pvl genes. MRSA is the most common identifiable cause of skin and soft-tissue infections among patients presenting to emergency departments in 11 U.S. cities. When antimicrobial therapy is indicated for the treatment of skin and soft-tissue infections, clinicians should consider obtaining cultures and modifying empirical therapy to provide MRSA coverage. Albuquerque. 60% New Orleans. 67% Nebraska 48% (n = 203) North Dakota 30% (n = 218) South Dakota 42% (n = 226) Wisconsin 21% (n = 198) Moran GJ et al. NEJM :")
45
Chambers H www.mrsai.org

46
S. aureus resistant or with reduced susceptibility to vancomycin
VRSA, VISA and hVISA

47
Streptococcus pneumoniae
Most important pathogen in mild-to-moderate RTIs Greatest morbidity Greatest mortality

48
Invasive Pneumococcal Disease in Children 5 Years After Conjugate Vaccine Introduction 1998 - 2005
The overall incidence of IPD among children aged <5 years declined from 99 cases/100,000 during to 23 cases/100,000 in 2005 The largest percentage decline (82%) and the largest absolute rate reduction in overall IPD (175.8 cases per 100,000) were observed among children aged 1 year, the age group with the highest baseline rate (Table). The incidence of PCV7-type IPD decreased significantly among all children aged <5 years from to The largest absolute rate reduction in PCV7-type disease was observed among children aged 1 year (175.7 cases per 100,000). Non-PCV7--type IPD increased significantly among children aged <1 year and 4 years (Table). MMWR Feb 2008.
 and the largest absolute rate reduction in overall IPD (175.8 cases per 100,000) were observed among children aged 1 year, the age group with the highest baseline rate (Table). The incidence of PCV7-type IPD decreased significantly among all children aged <5 years from to The largest absolute rate reduction in PCV7-type disease was observed among children aged 1 year (175.7 cases per 100,000). Non-PCV7--type IPD increased significantly among children aged <1 year and 4 years (Table). MMWR Feb")
49
Impact of PCV7 Vaccination On NVT-IPD in Children <5 Years, USA 1998-2003
ABCs data vs 1998/99.

50
Dortet L et al. Diag Micro ID 2009
Serotype distribution of S. pneumoniae isolated from invasive disease in children and adults (France: 2007) Dortet L et al. Diag Micro ID 2009
 Dortet L et al. Diag Micro ID")
51
Multi-locus sequence typing of MDR serotype 19A isolates (n = 97)
Pillai D et al. BMC Genomics 2009

52
Minimum spanning tree of MDR and non-MDDR serotype 19A
Pillai D et al. BMC Genomics 2009

53
Emergence of a multidrug-resistant clone (ST320) among invasive serotype 19A pneumococci in Spain
Objectives: Multidrug-resistant Streptococcus pneumoniae isolates of serotype 19A have emerged all over the world in recent years. The aim of this study was to characterize highly penicillin-resistant pneumococcal strains of the 19A serotype, collected in Spain from 1997 to 2007 from patients with invasive disease. Methods: Antibiotic susceptibility was studied by microdilution. All penicillin-resistant pneumococci were typed by PFGE and selected strains were studied by multilocus sequence typing (MLST). The presence of genes related to the Tn916 family of transposons was investigated by PCR. Results: From a total of 1197 invasive pneumococcal isolates of serotype 19A received at the Spanish Reference Laboratory between 1997 and 2007, 51 (4.3%) strains showed high-level resistance to penicillin (MICs of 2–4 mg/L). These 51 isolates belonged to three multiresistant clones related to sequence type (ST)81 (n521), ST320 (n519) and ST276 (n511). All 51 serotype 19A pneumococci were tetracycline-resistant and had the tet(M) gene, and 41 strains were macrolide-resistant, harbouring the erm(B) gene. The presence of int and xis genes was detected in all strains associated with other genes of the Tn916 family. Conclusions: The rise in penicillin-resistant serotype 19A invasive pneumococci in Spain was associated with the emergence and clonal spread of two worldwide-disseminated multiresistant clones (ST276 and ST320). The Spain23F-1-19A (ST81) clone remained stable throughout the study period. Multidrug resistance was associated with transposons of the Tn916 family. Distribution of penicillin-resistant serotype 19A isolates belonging to different clones throughout the study period. The bars indicate the proportion of each serotype 19A clone among penicillin-resistant pneumococci
. The. presence of genes related to the Tn916 family of transposons was investigated by PCR. Results: From a total of 1197 invasive pneumococcal isolates of serotype 19A received at the Spanish. Reference Laboratory between 1997 and 2007, 51 (4.3%) strains showed high-level resistance to penicillin. (MICs of 2–4 mg/L). These 51 isolates belonged to three multiresistant clones related to sequence. type (ST)81 (n521), ST320 (n519) and ST276 (n511). All 51 serotype 19A pneumococci were. tetracycline-resistant and had the tet(M) gene, and 41 strains were macrolide-resistant, harbouring the. erm(B) gene. The presence of int and xis genes was detected in all strains associated with other genes. of the Tn916 family. Conclusions: The rise in penicillin-resistant serotype 19A invasive pneumococci in Spain was associated. with the emergence and clonal spread of two worldwide-disseminated multiresistant clones. (ST276 and ST320). The Spain23F-1-19A (ST81) clone remained stable throughout the study period. Multidrug resistance was associated with transposons of the Tn916 family. Distribution of penicillin-resistant serotype 19A isolates belonging to different clones throughout the study period. The bars indicate the proportion of each serotype 19A clone among penicillin-resistant pneumococci.")
54
S. pneumoniae Serotype 19A in Children, South Korea
From 1991 through 2006, 538 strains of S. pneumoniae were obtained from various clinical specimens Figure 2. Distribution of serotypes with regard to 7-valent conjugate vaccine (PCV7) among 107 pneumococci isolated from children <5 years of age with an invasive pneumococcal infection (IPD) during fi ve 3- or 4- year periods from 1991 through 2006, South Korea. *The observed increase in the proportion of 19A (p = 0.005)and decrease in the proportion of 19F (p = 0.008) among invasive isolates were statistically signifi cant. Choi EH et al. EID 2008
 among 107 pneumococci isolated from children <5 years of. age with an invasive pneumococcal infection (IPD) during fi ve 3- or 4- year periods from 1991 through 2006, South Korea. *The observed increase. in the proportion of 19A (p = 0.005)and decrease in the proportion of 19F (p = 0.008) among invasive isolates were statistically signifi cant. Choi EH et al. EID")
55
S. pneumoniae Serotype 19A in Children, South Korea
However, there is no evidence of capsular switching as a contributing factor to the increasen in serotype 19A in our study. According to eBURST analysis, 1 major CC (CC271) accounted for most of the isolates (n = 116, 92% of serotypes 19A and 19F). CC271 comprised 16 STs, where ST271 was predicted as the founder, and ST320 was the predominant allelic profi le. The 5 ST lineages that were unrelated to CC271 were nonlinked singlets (ST1203, ST1374, ST2394, ST2395, and ST2399) (Figure 3). ST320 was the only ST found among serotypes 19A and 19F; ST320 was the most common ST (n = 52, 90% of total 19A isolates) among serotype 19A. ST320 was observed in only 9% (n = 6) of serotype 19F isolates. The genetic structure of serotype 19A comprised primarily ST1374 during periods 1 and 2 (1991–1997), but ST1374 isolates were not recovered after In contrast, ST320 was the most common sequence type from 1998, and all 19A isolates from 2002–2006 were of ST320. The numbers of 19A isolates increased consistently from 1996 through 2003, which suggests that single clonal expansion of ST320 was responsible for the increase of serotype 19A isolates during this period (Figure 4). Unlike serotype 19A, serotype 19F comprises diverse STs grouped within CC271 (16 STs) and 5 different singlets. All STs, except ST1203, were associated with multidrugresistant mef/erm-containing isolates. The distributions of predominant STs among serotype 19F isolates varied during each study period (Figure 4). For example, ST2395 predominated in period 1 (1991–1994), but ST1464 (an SLV of ST271) predominated in periods 4 and 5 (2001–2006). Choi EH et al. EID 2008
 accounted for most of the isolates (n = 116, 92% of serotypes. 19A and 19F). CC271 comprised 16 STs, where. ST271 was predicted as the founder, and ST320 was the. predominant allelic profi le. The 5 ST lineages that were. unrelated to CC271 were nonlinked singlets (ST1203, ST1374, ST2394, ST2395, and ST2399) (Figure 3). ST320 was the only ST found among serotypes 19A. and 19F; ST320 was the most common ST (n = 52, 90% of total 19A isolates) among serotype 19A. ST320 was observed. in only 9% (n = 6) of serotype 19F isolates. The. genetic structure of serotype 19A comprised primarily. ST1374 during periods 1 and 2 (1991–1997), but ST1374. isolates were not recovered after In contrast, ST320. was the most common sequence type from 1998, and all. 19A isolates from 2002–2006 were of ST320. The numbers. of 19A isolates increased consistently from 1996 through. 2003, which suggests that single clonal expansion of ST320. was responsible for the increase of serotype 19A isolates. during this period (Figure 4). Unlike serotype 19A, serotype 19F comprises diverse. STs grouped within CC271 (16 STs) and 5 different singlets. All STs, except ST1203, were associated with multidrugresistant. mef/erm-containing isolates. The distributions of. predominant STs among serotype 19F isolates varied during. each study period (Figure 4). For example, ST2395 predominated. in period 1 (1991–1994), but ST1464 (an SLV. of ST271) predominated in periods 4 and 5 (2001–2006). Choi EH et al. EID")
56
Conclusions Old and continued antimicrobial resistance trends
- MRSA (hVISA, VISA, VRSA, tolerance, MDR) - DRSP (MDR, ST320) - VRE (MDR CC-17 E. faecium) - ESBLs in Enterobacteriaceae (CTX-M clones) - MDR P. aeruginosa and Acinetobacter spp. New resistance trends - CA-MRSA (increasing MDR patterns) - Serine carbapenemase in Enterobacteriaceae - Metallo-β-lactamases in all Gram-negative bacilli - MDR N. gonorrhoeae 56
 - DRSP (MDR, ST320) - VRE (MDR CC-17 E. faecium) - ESBLs in Enterobacteriaceae (CTX-M clones) - MDR P. aeruginosa and Acinetobacter spp. New resistance trends. - CA-MRSA (increasing MDR patterns) - Serine carbapenemase in Enterobacteriaceae. - Metallo-β-lactamases in all Gram-negative bacilli. - MDR N. gonorrhoeae. 56.")
Similar presentations


 in the Nordic countries Petter Elstrøm Advisor Norwegian Institute of Public Health.>")









. What is Antibiotic resistance ? Antibiotic resistance is a type of drug resistance where a microorganism is able to survive.>")

 surveillance (2009Q1-4) **** Data as.>")





