Download presentation
Presentation is loading. Please wait.

1
Improving Patient Safety in Primary Care
NHS Forth Valley 204/15 Neil Houston Clinical Lead,

2
Session Aims Review the safety work in Primary care in the last 12 months including: Improvements in safety of prescribing of NSAIDS Prescribing and monitoring of Warfarin and DMARDS Review use of Safety climate survey and trigger tool - Learn about the safety programme in 2014/15 which includes: Reliable medication reconciliation after discharge Appropriate use of antipsychotics in elderly patients Involving patients in making care safer

3
Session Aims What are we trying to achieve? Where have we got to?
What are our next steps?

4
Our Ambition To reduce the number of events which cause avoidable harm to people from healthcare delivered in any primary care setting. The programme ambition and aim support the Scottish Government’s Quality Strategy of safe, effective person-centred care. Primary care is a priority for the Scottish Government and will continue to be so.

5
Our Aim All NHS territorial boards and 95% of primary care clinical teams will be developing their safety culture and achieving reliability in 3 high-risk areas by 2016.

6
Safety at the interface
3 workstreams Safety Culture Safer medicines Safety at the interface How we going to achieve our aims -

7
Focus in 2013/14 National Trigger Tool Reviews (twice per annum) Safety Climate Survey (once per annum) Local Warfarin, DMARDS At this stage need to make reference to fact most people focusing this year on National areas and that these are supported within a contractual framework.

8
What are we trying to achieve?
Where have we got to? What are our next steps?

9
Health Board areas of focus
Warfarin NHS Ayrshire & Arran NHS Borders NHS Dumfries & Galloway NHS Fife NHS Forth Valley NHS Grampian NHS Highland NHS Lothian Medication Reconciliation NHS Ayrshire & Arran NHS Greater Glasgow and Clyde NHS Lothian NHS Orkney NHS Shetland NHS Western Isles DMARDS NHS Forth Valley NHS Lanarkshire NHS Tayside

10
Progress towards our aims
83% of all Scottish practices engaged in improving reliability of one high risk area 819 practices across Scotland currently collecting data and making improvements

11
Key Achievements All 57 FV practices signed up to Local Enhanced Service contracts using care bundle methodology for Near Patient Testing and Anti-coagulation in 2013/14 80% FV aggregate anticoagulation bundle compliance 56 (98.2%) of FV practices participated in the climate survey with 881 (89.8%) responses across practice staff 55 (96.5%) of practices participated in trigger tools reviews 36 practices undertook Significant Event Analysis around anticoagulation and NPT medications 100 + practice participants at FV Patient Safety Learning Session
 of FV practices participated in the climate survey with 881 (89.8%) responses across practice staff. 55 (96.5%) of practices participated in trigger tools reviews. 36 practices undertook Significant Event Analysis around anticoagulation and NPT medications practice participants at FV Patient Safety Learning Session.")
13
Anticoagulation Compliance
No of practices Prescribing INR duration Patient Advice Within 7 days Written Education Overall Apr 43 100.0 96.4 99.8 94.9 85.6 78.8 May 38 99.7 94.7 99.2 83.9 77.1 Jun 37 97.6 95.4 85.1 78.4 Jul 97.1 98.7 95.8 87.6 82.9 Aug 97.5 95.3 87.3 80.6 Sep 35 97.8 99.4 90.8 84.2 Oct 47 99.3 98.5 98.9 90.1 86.8 Nov 46 99.1 98.0 94.4 84.4 77.3 Dec 44 98.6 94.2 86.7 80.4 Jan 45 99.5 95.7 88.8 83.6 Feb 98.8 96.9 89.8 86.0 Mar 40 99.0 96.2 89.7 85.4

15
Efficiency!

16
MTX 2.5MG TABS AS % OF ALL ORAL RX :
FV VS OTHER HBS

17
Workstream Aims safety culture 95% of practices undertaking Trigger Tool Reviews and Safety Climate Survey, by April 2014 Individual boards have currently collating their Trigger Tool data and we heard some great examples of learning from trigger tool reviews this morning. In achieving our aim for the SCS – we’ve got to . . .

18
Progress towards our aims
90% of all practices in Scotland completed the Safety Climate Survey, by April 2014 90% - this is a massive achievement – think they should all give themselves round of applause.

19
NSAID prescribing Impact Latest data Oct – Dec 2013
Patients age ≥ 65 years on triple whammy combination. (ACE/ARB + diuretic + NSAID) Reduced by 31% Patients age ≥ 65 years prescribed an NSAID without gastroprotection Reduced by 33% Current anticoagulant user prescribed an NSAID without gastroprotection. Reduced by 55%
 Reduced by 31% Patients age ≥ 65 years prescribed an NSAID without gastroprotection. Reduced by 33% Current anticoagulant user prescribed an NSAID without gastroprotection. Reduced by 55%")
24
What are we trying to achieve?
Where have we got to? What are our next steps?

25
Our Aim All NHS territorial boards and 95% of primary care clinical teams will be developing their safety culture and achieving reliability in 3 high-risk areas by 2016. So when do we move to a new area . . .

29
Safety Programme Safe and Reliable Medicines Reconciliation after discharge Safe and Reliable antipsychotics in elderly patients with dementia Significant safety issues that occur at discharge using an SEA form Activity to involve patients in safety improvement work Climate Survey and Trigger Tool

30
More than 40% of medication errors result from inadequate reconciliation in handoffs during admission, transfer and discharge of patients. 20% of these were believed to result in harm. Institute of Medicine’s Preventing Medication Errors,

32
Medication Reconciliation
This is the type of discharge letter that some practices still receive when a patient comes out of hospital and it makes it very difficult to reconciel those medications accurately Failure to reconcile the medications after dischareg has been shown to lead to increase readmissions

33
Med Reconciliation after discharge - CQC
Unreliable at admission Inaccurate and delayed at discharge, Unreliable systems in place in primary care for updating 17% of practices delegation of the responsibility for medicines reconciliation to managerial or clerical staff. ‘Managing patients medicines after discharge from hospital’ October 2009. Its easy to blame the hospital but work done by the Care Quality Comission revealed that altho med rec is done poorly at admission and that discharge letters are often inaccurate and delayed at discharge practices do not have reliable systems in place for reconciling the meds when the patient comes home

34
Discrepancies between the hospital discharge prescription and drugs subsequently prescribed to the patient. Discrepancies found in 43% of patients. Of drugs newly prescribed by the hospital, 28% were either not continued or altered dose Where suggested a change in dose, the dose was not changed by the GP practice in 35% of cases. But it is an active process by GP – the hospital may not be right! UK study (Avery et al) 2012
")
35
Margaret story

36
Where do thing go wrong with medicines when a patient is discharged?

37
“In God we trust. All others bring data.”
W. E. Deming 37

38
Medicines Reconciliation
Audit 10 of the following patients per month: Patients who have been discharged from an acute medical admission and Patients over 75 years of age who have been discharged from an inpatient stay from anywhere

39
Medication Reconciliation Measures- National
1) Has Electronic Discharge Document ( IDL) been received by a clinician on the day of receipt. 2) Has medicines reconciliation on occurred within 2 working days of the IDL being received by the GP. 3) It is documented that any changes to the medication from their pre admission prescription have been recorded in the clinical record ? 4) It is documented that any changes to the medication have been discussed with the patient or their representative within 7 days of receipt? 5) Have all the above measures have been met (composite).
 Has Electronic Discharge Document ( IDL) been received by a clinician on the day of receipt. 2) Has medicines reconciliation on occurred within 2 working days of the IDL being received by the GP. 3) It is documented that any changes to the medication from their pre admission prescription have been recorded in the clinical record 4) It is documented that any changes to the medication have been discussed with the patient or their representative within 7 days of receipt 5) Have all the above measures have been met (composite).")
40
Medicines Reconciliation Bundle Forth Valley 2014 / 15
1.Has the immediate discharge document (IDL) been forwarded to a clinician on the day of receipt? 2.Has medicine reconciliation occurred within 7 days of the IDL being received by the practice? 3.Is it documented that any changes to the medication following reconciliation have been updated in EMIS within 7 days of the IDL being received by the practice? 4.Is it documented that any *significant changes to medications have been discussed with the patient or their representative if appropriate within 7 days of the IDL being received by the practice? *significant changes include a repeat medication being started or stopped or alteration in dose 5.All measures have been met
 been forwarded to a clinician on the day of receipt 2.Has medicine reconciliation occurred within 7 days of the IDL being received by the practice 3.Is it documented that any changes to the medication following reconciliation have been updated in EMIS within 7 days of the IDL being received by the practice 4.Is it documented that any *significant changes to medications have been discussed with the patient or their representative if appropriate within 7 days of the IDL being received by the practice *significant changes include a repeat medication being started or stopped or alteration in dose. 5.All measures have been met.")
41
The truth will set you free…… But first it will piss you off !

42
Help Provided Guidance Data collection Identifying patients Templates

44
Codes and their meaning --?!
Read Code Term Display on template and record 1 8HE2 Discharged from inpatient care IDL received and workflowed 2 8B318 Medication reconciliation 3 67Is Advice to continue with drug treatment No changes to drug treatment 8B3R Drug therapy discontinued 8B3A3 New medication commenced 8B316 Medication changed Medication dose altered 8B314 Medication review done Medication record updated 4 8B3S0 Post hospital discharge medication reconciliation with pt Medication discussed with patient or carer 8BIo Drug directions adequate and appropriate Not appropriate / necessary to discuss with patient / carer 671G0 Medication discussed with pharmacist And/ or practice admin staff

45
Information appears clearly in EMIS consultation history

46
If templates are used coded information can be searched

47
GP IT site

48
NHS Ayrshire & Arran’s Experience
John Freestone – GP Clinical lead East and South Ayrshire

49
What have we done so far? Local Enhanced Service
Medicine reconciliation Warfarin management Patient safety SEAs Reconciliation of addiction medication Local collaborative meetings 47 out of 55 practices taking part

50
Medicines Reconciliation
Audit 10 of the following patients per month: Patients who have been discharged from an acute medical admission, and Patients over 75 years of age who have been discharged from an inpatient stay from anywhere Has the Immediate Discharge Document been workflowed on the day of receipt? Has medicines reconciliation occurred within 2 working days of the Immediate Discharge Document being workflowed to the GP/Pharmacist? Is it documented that any changes to the medications have been discussed with the patient or their representative? Are all the above measures met?

51
Medicines Reconciliation
Compliance with bundle – May Compliance with bundle – Feb 2014

52
Medicines Reconciliation – how did we improve?
Data and feedback – so practices knew if they were improving Local collaborative – sharing systems and learning Attempting to institute a whole systems approach

53
Data and Feedback

54
Data and Feedback

55
Collaborative Meetings
1 launch day and then 3 half day meetings in localities Attended by GP, manager and practice nurse Discuss progress, patient stories, QI tools Small group work Review results – benchmarking Discuss systems Discuss SEAs Feedback with commitment to change Systems employed - variable Newsletter with summary of learning and sharing of resources

56
Patient Story – Mr D (84) Admitted with chest pain PMH Angina
Atrial fibrillation Discharge diagnosis: Acute Coronary Syndrome Medication on IDL - angina meds changed Nicorandil added Bisoprolol seemed to be stopped Medicines reconciled Patient story that illustrates some of these challenges and successes

57
Patient Story – Mr D (84) Patient phoned
Unsure of meds - daughter deals with them Patient asked to get daughter to phone 2 weeks later – house visit request short of breath Pulse 120 irreg, signs of LVF Admitted - Bisoprolol restarted Patient story that illustrates some of these challenges and successes

58
Patient Story – Mr D (84) SEA – unnecessary admission. Discussed with consultant. Error on IDL Not picked up by practice system due to patient confusion about medications Change to practice system How record carers and how record contact them Used stories like these to allow practices to reflect on their systems

59
Positive SEAs Potential errors picked up early by new systems
IDLs often questioned Communication between practice, patient, carer and pharmacist better

60
Systems

61
Medicines reconciliation - template
Screen shot of Johns template

62
Whole System Working Developing links with IT Secondary care Pharmacy

63
Review of IDLs from Interface Issues Crosshouse Hospital 2012
Quality and accuracy of IDLs HEPMA – electronic discharges Access to Key Information Summary Induction training Audit of IDLs

64
Medicines reconciliation - successes
Improvement to systems Sharing of ideas between GPs Development of links between practices Development of links between leads and other areas of health care Identification of “local champions” “I don’t think it is difficult [medicines reconciliation]. It takes a bit more work but it’s what we should be doing after all.” North Ayrshire GP

65
Medicines reconciliation – challenges
Buy in by GPs – “problem is with secondary care not with us” Workload issues in GP Problem with systems Patients with cognitive impairment Patients who are not aware of the changes made in hospital Carers Blister packs Interface issues including the quality of Immediate discharge letters

66
Future SPSP LES 2014 Continue medicines reconciliation
Option of enhanced SEA Re-launch and learning sets Closer working between patient safety leads in primary and secondary care

67
NHS GG&C Reflections from 13/14
Q1: does the meds rec work improve patient safety? 86% Yes % No % possibly Q2: does the meds rec work improve practice processes? 76% Yes % No % formalised existing process Q3: did you use your data to make improvements? 62% Yes % No % made improvements but not specifically from the data

68
Reflections from 13/14 LES practices so far (n=21)
Main +ve Time: less calls/queries from patient standard process reduces time spent rectifying error better organisation/reduced frustration better practice communication Patients really like it Main –ve Time: chasing secondary care more admin work trying to contact patients identifying cohort

69
Questions?

70
A possible way to improve your systems Process mapping made easy!

71
What about secondary care?

72
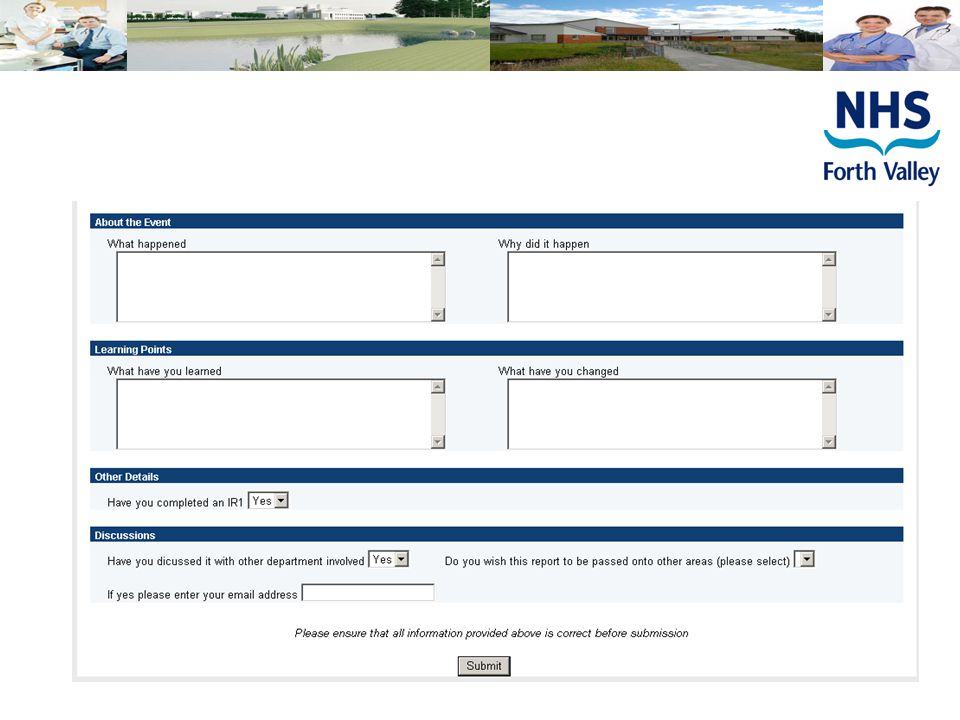
SEAs Practices will highlight to the Board significant safety issues that occur at discharge using an SEA form.

73
Process for recording Quick Easy Links to appraisal – submit and save
Takes account of SAER policy Allows links to M & M in other departments Emerging themes – newsletter and risk register

76
Questions?

77
A Scottish Government CEL A strategic plan medicines reconciliation across the single system
Admission Goals 95% compliance with medicines reconciliation within 24 hours of admission Discharge Goals 95% compliance with medicines reconciliation on discharge 95% of patients have an accurate medicines list on the Interim Discharge Letter (IDL) Patient demographics documented Allergy status on discharge documented Changes from admission medicines documented to include changes, discontinuations and new medicines started
 Patient demographics documented. Allergy status on discharge documented. Changes from admission medicines documented to include changes, discontinuations and new medicines started.")
78
Medicines Reconciliation and patient safety– Acute Care
Scott Hill Lead Pharmacist Acute Services

79
Medicines reconciliation
Medicines most common healthcare intervention Inadequate medicines reconciliation accounts for up to 20% of adverse drug events and 46% of all medication errors amongst hospital in patients (Roizic 2001)
")
80
Safer Use of Medicines SGHD/CMO (2013) 18 Key messages
Provides national definition, goals, measures and recommended practice statements Patient centred approach Clinical leadership and champions Monitoring of goals

81
Measurement Goal - 95 % compliance with medicines reconciliation within 24 hours of admission Month October 2013 November 2013 December 2013 January 2014 February 2014 March 2014 Demographics 90% 95% 100% 94% Allergy status 60% 65% 85% 87% Two or more sources 35% 70% 73% 93% 75% Plan for each medicine 30% 55% 84% Accurate list of medicines 80% Med. Rec. in 24 hours (all 5 of above) 10% 20% 45% 63% 50%
 10% 20% 45% 63% 50%")
82
Pharmacy in Primary Care – Our Aims
Improve patient safety by strengthening the contribution of pharmacists to : Improve the reliability medication reconciliation when patients are discharged from hospital Deliver reliable processes underpinning the safe prescribing monitoring dispensing and administering of high risk medications Improve the safety culture of pharmacy teams in the community

83
Implement a care bundle for medicines reconciliation
HIS will support 3 health boards to participate in a collaborative (June 14 – June 16) Each NHS board will recruit - Pharmacy clinical lead, 8 pharmacy teams, section of the acute sector and 2 GP practices Pharmacy Teams will attend National and Local Learning Sessions run by the participating boards. After attending a learning event and learning about the Model for Improvement pharmacy teams will: Implement a care bundle for medicines reconciliation high risk medicines, ie Warfarin, Lithium, Methotrexate Carry out a safety climate survey Timeframe – Received applications from 7 health boards – shortlisting this week Interviews taking place on 27th May and successful boards will commence in June 2014.
 Each NHS board will recruit - Pharmacy clinical lead, 8 pharmacy teams, section of the acute sector and 2 GP practices. Pharmacy Teams will attend National and Local Learning Sessions run by the participating boards. After attending a learning event and learning about the Model for Improvement pharmacy teams will: Implement a care bundle for. medicines reconciliation. high risk medicines, ie Warfarin, Lithium, Methotrexate. Carry out a safety climate survey. Timeframe – Received applications from 7 health boards – shortlisting this week. Interviews taking place on 27th May and successful boards will commence in June")
84
Coming soon – Involving Community Pharmacy in making care safer Med rec andf high risk medicines Communication of IDL Testing work begins late 2015 Hopefully Fv involved – need 2 interested practices

86
2 data collections per year
What about the others Warfarin and NPT 2 data collections per year £200 per practice in ES

87
Safety Programme Safe and Reliable Medicines Reconciliation after discharge Safe and Reliable antipsychotics in elderly patients with dementia Significant safety issues that occur at discharge using an SEA form Activity to involve patients in safety improvement work Two half day patient safety learning sets within existing PLT (eg CREATE) Climate Survey and Trigger Tool
 Climate Survey and Trigger Tool.")
88
WSW LES Timeline

89
Med Rec Data Entry Sheet

90
Med Rec Paper Data Collection Sheet

91
Med Rec Compliance Run Charts

92
Med Rec Reflection Form

93
Questions?

94
FV Safety Climate 2014 Dr Simon Randfield
What does safety climate mean? FV Safety Climate Dr Simon Randfield

95
The way things are done around here
Safety Culture “ Individual and group values, attitudes, perceptions and patterns of behavior that determine their commitment to safety management” The way things are done around here NHS Education for Scotland 2010 It’s a snap shot of an organisations safety culture- the way things are done around here – when no ones watching….

96
Adverse Event Causation
Technical Factors (30-20%) Accident Causation Why is it important? Because of role of safety culture on accident causation % of such Human Factors Safety Culture Operator Behaviour (70-80%) = +
 Accident. Causation. Why is it important Because of role of safety culture on accident causation % of such. Human. Factors. Safety. Culture. Operator. Behaviour. (70-80%) = +")
97
Safety Climate- QOF QOF - QI002 (now QS008) The practice conducts a safety climate survey with all staff, clinical and non-clinical, using a validated tool, meets to discuss the results, and shares a reflective report on action that arise from this with the NHS Board. And why are you here? Well because of 5 qof points of course!

98
Progress towards our aims
90% of all practices in Scotland completed the Safety Climate Survey, by April 2014 90% - this is a massive achievement – think they should all give themselves round of applause.

99
Completed numbers in each Health Board April 2014
Registered Completed Not Completed All practices % of Practices Registered Board A&A 54 56 100% 96% Borders 23 22 1 D&G 32 34 94% Fife 55 59 98% 95% FORTH VALLEY 57 Grampian 68 63 5 81 93% 84% GG&C 249 242 7 261 97% Highland 83 100 83% Lanarkshire 87 86 96 99% 91% Lothian 115 111 4 127 Orkney 10 9 90% Shetland 8 89% Tayside 67 Western Isles Registered of all 914 893 77 991 92% Completed of all registered 21 Completed of all practices - excellent buy in across Scotland, a real interest for many to see how this tool might benefit their own practices. Even better in forth valley- HIGHLIGHT FORTH VALLEY FIGURES well done!!

100
Forth Valley - Simply the best!
In Forth Valley 881 of 981 practice staff took part in the climate survey With in practices, uptake varied from 50% to 100%, but only 6 practices achieved less than 80% uptake and 26 achieved 100% uptake

101
Using the SafeQuest Safety Climate Survey work in practice?
PRACTICE EXPERIENCE… WHO?

102
POINTS TO REMEMBER 1 Engage all practice
Protected time for staff to complete. Anonymised Negative questions

103
The good..

104
The bad..

105
..and the ugly The blob fish . There were no ugly returns, although some were cursory, and perhaps unlikley to find any benefit from the processes, many were of a high quality and showed remarkable commitment to the process

106
Safety Climate Survey - Pros
Good for staff morale Communication Work well as a team Interesting to look at different views on safety issues Positive experience Makes you think about team more Staff talking to GPs Help to make positive changes We found this a particularly useful forum for open discussion within the team.. actually helped us pinpoint areas of specific need… Trouble Shooting Time Got team thinking Good insight

107
Safety Climate Survey - Cons
Communication could be better Used PLT -> Chair facilitate GP/PM Didn’t benefit much from it Not that anonymous Age/gender Are things really that bad? Didn’t feel staff would give true response Small number of return/survey completed Involve more Team Members into SEA Despite concerns that the process might disturb the hornets nest that lies buried in dome practices, there was very little fallout and NO practices have asked for additional facilitation on the outcomes of their surveys. workload Can be difficult in a small practice Time consuming Time loss

108
How to use this information?

109
Practice experience - what to do with it
‘Viewpoint – Point of view’ Our experience – the highs and lows. Results – Problems highlighted: Communication, meetings. Areas of improvement: Communications book - a visual reference tool. Admin meetings. G.P. involvement. Open forum - team participation. PRACTICE EXPERIENCE… WHO?

110
110

111
Communication: Forms of communication tasks/ docman/ messages
More regular meetings, including admin Communications book White board Distribution of agenda and minutes from meetings Shared storage of data (guidelines , etc) Doctors whereabouts and contractibility Difference between management and non Mx perceptions
 Doctors whereabouts and contractibility. Difference between management and non Mx perceptions.")
113
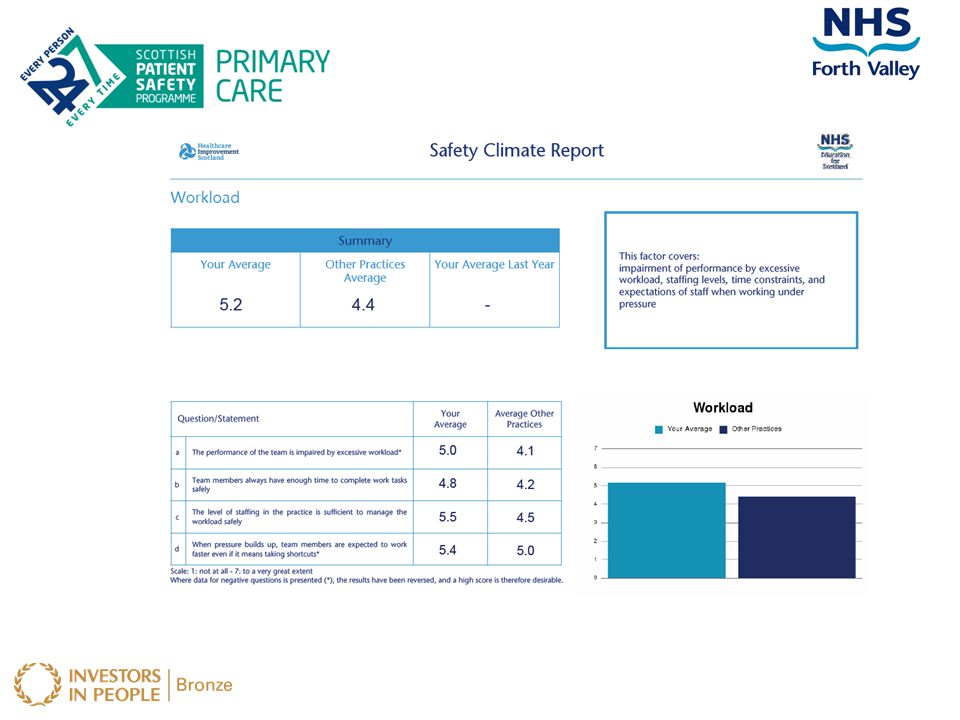
Workload: “Pace of work leaves little time for planning”
Changing staff hours to cover peak times Installation of touch screen arrival system Discussion re doctors sessions

115
Leadership: Practice vision unclear/ poorly communicated
Training for dealing with “problem staff members”

117
Teamwork: Team building event Better planning of (limited) CREATE PLT
Grumble board Staff shadowing

119
Safety systems: Involving admin in SEAs (admin staff keen)
Each member of admin is expected to produce 1 SEA annually Concerns re IT communications limitation (MIDIS)
")
120
POINTS TO REMEMBER 2 Time for adequate practice discussion
Motivation to address findings PRACTICE EXPERIENCE… WHO?

121
POINTS TO REMEMBER 3 The findings are for your practice teams
Don't get too focused on the numbers Concentrate on how you might use the results to drive improvements It’s a tool, a snapshot Takes time to change PRACTICE EXPERIENCE… WHO?

122
Changes? QOF 2014-15 same format
How to make it more useful on repeated use? Confidence limits Free text options additional questions confidential feedback questionnaire asking for further details.

123
Climate Survey Learning
“a very useful discussion for all” “Embrace the Challenge – its worth it!”

124
Tea and Coffee

Similar presentations