Download presentation
Presentation is loading. Please wait.

1
Herpes Zoster and Post-Herpetic Neuralgia
Carol Sue Carlson, MD March 28, 2008

2
Zoster (AKA “Shingles”)
")
3
Case – MR Dx: CN V3 Herpes Zoster 53 yo ♂
C5 Tetraplegic 2o to Spinal Cord Infarct PMHx: NonHodgkins Lymphoma s/p Chemo/RT on Decadron po c/o burning, achy pain in posterior neck ~36-48 hrs later rash Dx: CN V3 Herpes Zoster Pain!! PCA, Acyclovir, Amitryptiline, Oxcarbazepine, Pregabalin, Duloxetine, Capsaicin, Lidoderm 5% patch, Methadone, Hydrocortisone Cream, Triamcinolone Cream

4
Case – MR

5
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
6
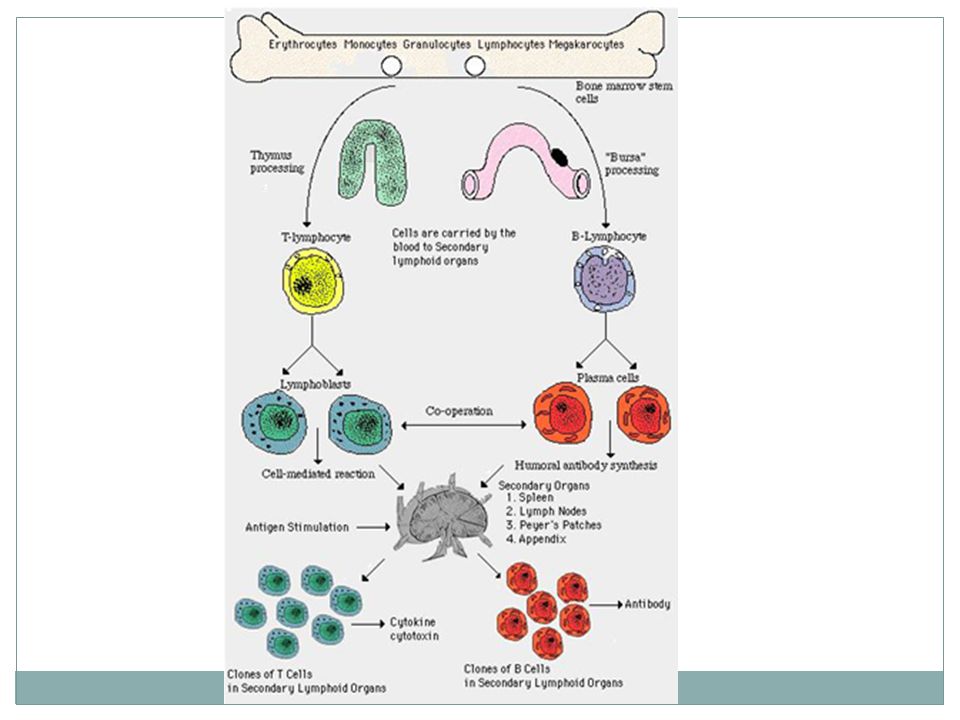
Varicella-Zoster Virus
Herpes Virus Family includes HSV-1, HSV-2, EBV, CMV, VZV Large, enveloped virus replicates in the cell’s nucleus

7
Varicella Zoster Virus
Varicella “Chicken Pox” Zoster “Shingles” 1st – Infection w/ Varicella Chicken Pox Latent infection established in Dorsal Root Ganglion Reactivation of VZV Shingles Shingles = a painful, unilateral vesicular eruption in a restricted dermatomal distribution Initial Zoster infxn can occur 2o to wild-type or vaccine-type VZV infxn

8
Varicella Zoster Virus – Pathogenesis
Viral Latency Limited # of Proteins Expressed Emergence from Latency Not Well-Understood Reactivation Spreads w/in Ganglion Multiple Sensory Neurons Infection of Skin 1 of proteins expressed is “Immediate Early Protein 63” Immunity to this protein can be detected in immune pts w/o evidence of Zoster This may play a role in maintaining the virus in a latent state EMERGENCE from Latency Active Zoster – in both Nucleus and Cytoplasm Latent Zoster – in Nucleus only REACTIVATION -once this occurs, virus spreads to other cells w/i the ganglion to involve multiple sensory neurons and establishes infxn of the skin

9
Varicella Zoster Virus – Pathogenesis

10
Acute Zoster Pathogenesis
1st - Hemorrhagic Inflammation Peripheral Nerve Dorsal Root DRG Spinal Cord Leptomeninges Nociceptor Activation Poorly Localized Pain “Pre-Herpetic Neuralgia” Nociceptor Sensitization Clinical Ramifications Pathogenesis of Acute Herpes Zoster: Virus persists for a period of years in DRG Reactivation of virus in DRG With waning cellular immunity, Virus is transported along peripheral nerves acute neuritis At Cellular Level – FIRST Hemorrhagic Inflammation of the (1) peripheral nerve, (2) dorsal root, (3) DRG MAY SEE: extension centrally into Spinal Cord and Leptomeninges Replicating virus can cause damage within the spinal ganglion and peripheral nerve DUE TO SEVERAL FACTORS! (1) direct neurolytic injury in heavily infected cell bodies and axons (2) indirect damage 2o to inflammatory rxn – which is accompanied by intraneural and intraganglionic hemorrhage DIRECT and INDIRECT injury “injury discharges” ~ ”short circuit” -neuron can seal itself off proximally single axon can emit multiple injury discharges -in some cases, if the damage to the axon is so severe, the primary afferent neuron can die The escape of the herpes virus from the sensory nerve fibers into the skin and subcutaneous tissues MASSIVE INFLAMMATORY RESPONSE actual tissue damage The cutaneous inflammation and tissue damage give rise to pain in much the same way as an ordinary burn Tissue damage DIRECTLY EXCITES NOCICEPTORS AND nociceptors become sensitized in the presence of inflammation NOCICEPTOR SENSITIZATION: characterized by 3 acquired abnormalities Spontaneous discharge (nociceptors are normally silent) a lowered activation threshold (they are excited by normally innocuous stimuli) exaggerated response to stimuli that exceed the NL pain threshold CLINICALLY these abnormalities cause ongoing/spontaneous pain, ALLODYNIA, HYPERALGESIA The inflammatory response that excites and sensitizes the nociceptors that innervate the sheath surrounding the nerve and ganglion (ie: the nervi nervorum) poorly localized, deep, aching pain -inflammation of the nerve sheath and injury discharge from nociceptors may account for “pre-herpetic neuralgia” – pain and dysesthesia that precede the cutaneous rash SECOND Fibrosis in DRG, Nerve root, Peripheral Nerve UPON RESOLUTION OF ACUTE PROCESS AUTOPSY RESULTS: dorsal horn atrophy, cellular, axonal, and myelin loss with fibrosis in the sensory ganglion -BUT!! Seen in both pts w/ and w/o PHN
 peripheral nerve, (2) dorsal root, (3) DRG. MAY SEE: extension centrally into Spinal Cord and Leptomeninges. Replicating virus can cause damage within the spinal ganglion and peripheral nerve. DUE TO SEVERAL FACTORS! (1) direct neurolytic injury in heavily infected cell bodies and axons. (2) indirect damage 2o to inflammatory rxn – which is accompanied by intraneural and intraganglionic hemorrhage. DIRECT and INDIRECT injury injury discharges ~ short circuit -neuron can seal itself off proximally single axon can emit multiple injury discharges. -in some cases, if the damage to the axon is so severe, the primary afferent neuron can die. The escape of the herpes virus from the sensory nerve fibers into the skin and subcutaneous tissues MASSIVE INFLAMMATORY RESPONSE. actual tissue damage. The cutaneous inflammation and tissue damage give rise to pain in much the same way as an ordinary burn. Tissue damage DIRECTLY EXCITES NOCICEPTORS AND nociceptors become sensitized in the presence of inflammation. NOCICEPTOR SENSITIZATION: characterized by 3 acquired abnormalities. Spontaneous discharge (nociceptors are normally silent) a lowered activation threshold (they are excited by normally innocuous stimuli) exaggerated response to stimuli that exceed the NL pain threshold. CLINICALLY these abnormalities cause ongoing/spontaneous pain, ALLODYNIA, HYPERALGESIA. The inflammatory response that excites and sensitizes the nociceptors that innervate the sheath surrounding the nerve and ganglion (ie: the nervi nervorum) poorly localized, deep, aching pain. -inflammation of the nerve sheath and injury discharge from nociceptors may account for pre-herpetic neuralgia – pain and dysesthesia that precede the cutaneous rash. SECOND Fibrosis in DRG, Nerve root, Peripheral Nerve UPON RESOLUTION OF ACUTE PROCESS. AUTOPSY RESULTS: dorsal horn atrophy, cellular, axonal, and myelin loss with fibrosis in the sensory ganglion. -BUT!! Seen in both pts w/ and w/o PHN.")
11
Acute Zoster Pathogenesis
2nd - Fibrosis DRG Nerve Root Peripheral Nerve Autopsy Results Similar +/- PHN Pathogenesis of Acute Herpes Zoster: Virus persists for a period of years in DRG Reactivation of virus in DRG With waning cellular immunity, Virus is transported along peripheral nerves acute neuritis At Cellular Level – FIRST Hemorrhagic Inflammation of the (1) peripheral nerve, (2) dorsal root, (3) DRG MAY SEE: extension centrally into Spinal Cord and Leptomeninges Replicating virus can cause damage within the spinal ganglion and peripheral nerve DUE TO SEVERAL FACTORS! (1) direct neurolytic injury in heavily infected cell bodies and axons (2) indirect damage 2o to inflammatory rxn – which is accompanied by intraneural and intraganglionic hemorrhage DIRECT and INDIRECT injury “injury discharges” ~ ”short circuit” -neuron can seal itself off proximally single axon can emit multiple injury discharges -in some cases, if the damage to the axon is so severe, the primary afferent neuron can die The escape of the herpes virus from the sensory nerve fibers into the skin and subcutaneous tissues MASSIVE INFLAMMATORY RESPONSE actual tissue damage The cutaneous inflammation and tissue damage give rise to pain in much the same way as an ordinary burn Tissue damage DIRECTLY EXCITES NOCICEPTORS AND nociceptors become sensitized in the presence of inflammation NOCICEPTOR SENSITIZATION: characterized by 3 acquired abnormalities Spontaneous discharge (nociceptors are normally silent) a lowered activation threshold (they are excited by normally innocuous stimuli) exaggerated response to stimuli that exceed the NL pain threshold CLINICALLY these abnormalities cause ongoing/spontaneous pain, ALLODYNIA, HYPERALGESIA The inflammatory response that excites and sensitizes the nociceptors that innervate the sheath surrounding the nerve and ganglion (ie: the nervi nervorum) poorly localized, deep, aching pain -inflammation of the nerve sheath and injury discharge from nociceptors may account for “pre-herpetic neuralgia” – pain and dysesthesia that precede the cutaneous rash SECOND Fibrosis in DRG, Nerve root, Peripheral Nerve UPON RESOLUTION OF ACUTE PROCESS AUTOPSY RESULTS: dorsal horn atrophy, cellular, axonal, and myelin loss with fibrosis in the sensory ganglion -BUT!! Seen in both pts w/ and w/o PHN
 peripheral nerve, (2) dorsal root, (3) DRG. MAY SEE: extension centrally into Spinal Cord and Leptomeninges. Replicating virus can cause damage within the spinal ganglion and peripheral nerve. DUE TO SEVERAL FACTORS! (1) direct neurolytic injury in heavily infected cell bodies and axons. (2) indirect damage 2o to inflammatory rxn – which is accompanied by intraneural and intraganglionic hemorrhage. DIRECT and INDIRECT injury injury discharges ~ short circuit -neuron can seal itself off proximally single axon can emit multiple injury discharges. -in some cases, if the damage to the axon is so severe, the primary afferent neuron can die. The escape of the herpes virus from the sensory nerve fibers into the skin and subcutaneous tissues MASSIVE INFLAMMATORY RESPONSE. actual tissue damage. The cutaneous inflammation and tissue damage give rise to pain in much the same way as an ordinary burn. Tissue damage DIRECTLY EXCITES NOCICEPTORS AND nociceptors become sensitized in the presence of inflammation. NOCICEPTOR SENSITIZATION: characterized by 3 acquired abnormalities. Spontaneous discharge (nociceptors are normally silent) a lowered activation threshold (they are excited by normally innocuous stimuli) exaggerated response to stimuli that exceed the NL pain threshold. CLINICALLY these abnormalities cause ongoing/spontaneous pain, ALLODYNIA, HYPERALGESIA. The inflammatory response that excites and sensitizes the nociceptors that innervate the sheath surrounding the nerve and ganglion (ie: the nervi nervorum) poorly localized, deep, aching pain. -inflammation of the nerve sheath and injury discharge from nociceptors may account for pre-herpetic neuralgia – pain and dysesthesia that precede the cutaneous rash. SECOND Fibrosis in DRG, Nerve root, Peripheral Nerve UPON RESOLUTION OF ACUTE PROCESS. AUTOPSY RESULTS: dorsal horn atrophy, cellular, axonal, and myelin loss with fibrosis in the sensory ganglion. -BUT!! Seen in both pts w/ and w/o PHN.")
12
Zoster Pathogenesis Pain of Acute Herpetic Neuralgia
(1) Inflammation 2o to Movement of Virus (2) Hyperexcitability of Dorsal Horn Neurons Spontaneous Activity Exaggerated Responses Allodynia, Hyperalgesia Interneuron Spread PAIN of ACUTE HERPETIC NEURALGIA -2o to inflammation from movement of viral particles from sensory nerves to the skin and subcutaneous tissues -activity of 1o afferent neurons that respond to tissue damage sensitization to further input spontaneous activity maintain pain in absence of ongoing tissue damage Activity transmitted to the spinal cord by unmyelinaed C-fiber nociceptors state of central hyperexcitability in spinal dorsal horn neurons -hyperexcitable spinal neurons may be spontaneously active AND have exaggerated responses to all input -central hyperexcitability is accompanied by ALLODYNIA, HYPERALGESIA from a large area of skin surrounding the site of injury -probably spreads via INTERNEURONS PAIN is 2o to: (1) injury discharges – ABNL, (2) nociceptor responses to inflamed nervi nervorum – NL 12
 Inflammation 2o to Movement of Virus. (2) Hyperexcitability of Dorsal Horn Neurons. Spontaneous Activity. Exaggerated Responses. Allodynia, Hyperalgesia. Interneuron Spread. PAIN of ACUTE HERPETIC NEURALGIA. -2o to inflammation from movement of viral particles from sensory nerves to the skin and subcutaneous tissues. -activity of 1o afferent neurons that respond to tissue damage. sensitization to further input. spontaneous activity. maintain pain in absence of ongoing tissue damage. Activity transmitted to the spinal cord by unmyelinaed C-fiber nociceptors state of central hyperexcitability in spinal dorsal horn neurons. -hyperexcitable spinal neurons may be spontaneously active AND have exaggerated responses to all input. -central hyperexcitability is accompanied by ALLODYNIA, HYPERALGESIA from a large area of skin surrounding the site of injury. -probably spreads via INTERNEURONS. PAIN is 2o to: (1) injury discharges – ABNL, (2) nociceptor responses to inflamed nervi nervorum – NL. 12.")
13
Intercostal Nerve Histology
Normal Post-Zoster Pathologic section demonstrates “FIBER DISSOCIATION” = Preferential loss of large diameter nerve fibers which are replaced by fibrous tissue = relative preservation and proliferation of small diameter nerve fibers With preferential loss of large fast conducting fibers and proliferation of small, slow conducting fibers, There is a LOSS OF INHIBITION slow fibers hyperesthesia

14
Zoster Pathogenesis – Reactivation
DRG and Dorsal Horn Intense Inflammation Hemorrhagic Necrosis of Nerve Cells Neuronal Loss Fibrosis Following reactivation of VZV, DRG shows intense inflammation, accompanied by hemorrhagic necrosis of nerve cells Ganglion undergoes eventual neuronal loss and subsequent fibrosis Dermatomal distribution of the vesicular rash of zoster corresponds to the sensory fields of many infected neurons w/i a specific ganglion

15
Zoster Pathogenesis Neurotransmitters: Therapeutic Implications
Substance P Transmission Serotonin, NE Inhibition Therapeutic Implications Studies No Difference Side to Side SUBSTANCE P has been implicated in transmission of pain signals SEROTONIN and NOREPINEPHRINE thought to play a role in INHIBITION of pain signals Studies of affected dorsal horn from a pt w/ PHN – NO DIFFERENCE IN LEVELS OF NTs FROM SIDE TO SIDE

16
Zoster – Cell Mediated Immunity
Cell-Mediated Immune Responses Control Viral Latency Limit Potential for Re-activation ↓ Skin Reactivity to VZV by 40 yo Severely ↓ by 60 yo ↑ Rates of Herpes Zoster In: Older Individuals Lymphoproliferative Malignancies BUT No ↑ Rates of Zoster or Protracted Varicella In: Children w/ Hypogammaglobulinemia CELL-MEDIATED IMMUNITY -Critical for controlling latency and limiting the potential for reactivation -Skin Test Reactivity: -lymphocyte stimulation responses to VZV Ag – waning skin reactivity by 40 yo and severely diminished cellular immunity to VZV by 60 yo -BUT virus specific humeral immunity was retained (IE: Immunoglobulins) -Uniform decline in VZV-specific cell-mediated immunity documented in older individuals, and pts w/ lymphoproliferative malignancies -Children with hypogammaglobulinemia (IE: decreased HUMERAL IMMUNITY) do NOT have severely protracted, fulminant primary varicella infxn or ↑ rates of Zoster -ABOVE indicate that a decline in CELL-MEDIATED IMMUNITY (NOT HUMERAL IMMUNITY) is directly linked to reactivated VZV syndromes
 -Uniform decline in VZV-specific cell-mediated immunity documented in older individuals, and pts w/ lymphoproliferative malignancies. -Children with hypogammaglobulinemia (IE: decreased HUMERAL IMMUNITY) do NOT have severely protracted, fulminant primary varicella infxn or ↑ rates of Zoster. -ABOVE indicate that a decline in CELL-MEDIATED IMMUNITY (NOT HUMERAL IMMUNITY) is directly linked to reactivated VZV syndromes.")
18
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
19
Zoster Epidemiology Cumulative Lifetime Incidence Older Age Groups
10-20% of Population Older Age Groups 30% > 55 yo Incidence ↑ w/Age 1 per 1000 in Pts < 20 yo 5-10X Greater in Pts > 80 yo ***Highest Incidence after 6th decade*** ♂ = ♀ Older age groups account for the highest incidence of zoster – LIKELY 2o to decline in Cell-Mediated Immunity

20
Zoster Epidemiology Immunocompromised at ↑↑↑ Risk
Age Disease Chemotherapy Several Times More Common in Pts w/ Ca, HIV, Transplant Recipients Incidence ↑ w/ Impairment of Immune System – Especially with Cell-Mediated Immunity Decline!! Zoster preferentially affects immunosuppressed populations – ESPECIALLY HIV-infected pts and transplant recipients Incidence ↑ with ↓ CD4 Count

21
Zoster Epidemiology

22
Zoster Epidemiology

23
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
24
Zoster – Natural History and Infectivity

25
Zoster – Natural History
75% have Prodromal Pain Grouped Vesicles or Bullae w/in 3-4 days Crusting in 7-10 Days No Longer Infectious Scarring, Hypo- or Hyperpigmentation Recurrence is Rare ~75% have prodromal pain in the dermatome where the rash appears Grouped vesicles or bullae – evolve into pustular or occasionally hemorrhagic lesion w/i 3-4 days Immunocompetent hosts – crusting in 7-10 days – NO LONGER INFECTIOUS Scarring and hypo- or hyperpigmentation may persist long after acute rash has resolved Recurrence in immunocompetent host is RARE

26
Zoster Rash

27
Zoster – Natural History
PAIN – Most Common Sx Deep, “Burning”, “Throbbing”, “Stabbing” Dermatomal Thoracic, CN V, Cervical – Most Common Zoster Keratitis, Zoster Ophthalmicus (CN V1) Systemic Sx – Rare (<20%) Most Cases – Self-Limited BUT: Can Interfere w/ Sleep, Appetite, Sexual Fnxn Psychosocial Dysfunction Pain is most common sx of zoster – can precede rash by days to weeks Prodromal pain can be constant or intermittent Can be confused w/ other etiologies (ie: angina, cholecystitis, renal colic) depending on the involved dermatome Generally limited to 1 dermatome in NL hosts BUT can occasionally involve 2-3 neighboring dermatomes Occasionally can have scattered vesicles located a distance away from the involved dermatome – when small amts of VZV are released from infected ganglion into bloodstream Thoracic and Lumbar are most common dermatomes involved but can have a more serious infection – ZOSTER KERATITIS or ZOSTER OPHTHALMICUS 2o to involvement of ophthalmic branch of CN V – can be sight-threatening <20% of pts have significant systemic sx – ie: HA, fever, malaise, fatigue
 Systemic Sx – Rare (<20%) Most Cases – Self-Limited BUT: Can Interfere w/ Sleep, Appetite, Sexual Fnxn. Psychosocial Dysfunction. Pain is most common sx of zoster – can precede rash by days to weeks. Prodromal pain can be constant or intermittent. Can be confused w/ other etiologies (ie: angina, cholecystitis, renal colic) depending on the involved dermatome. Generally limited to 1 dermatome in NL hosts BUT can occasionally involve 2-3 neighboring dermatomes. Occasionally can have scattered vesicles located a distance away from the involved dermatome – when small amts of VZV are released from infected ganglion into bloodstream. Thoracic and Lumbar are most common dermatomes involved but can have a more serious infection – ZOSTER KERATITIS or ZOSTER OPHTHALMICUS 2o to involvement of ophthalmic branch of CN V – can be sight-threatening. <20% of pts have significant systemic sx – ie: HA, fever, malaise, fatigue.")
28
Zoster Dermatomal Distribution

29
Zoster – Infectivity Immunocompetent Host Via:
Direct Contact w/ Lesion Contact Precautions Recommended in Hosp. Pts Until Lesions Crust VZV Naïve Pts Exposed to Zoster At Risk to Develop 1o Varicella NOT Zoster Localized Herpes Zoster in an immunocompetent host is ONLY CONTAGIOUS from direct contact with open lesions CONTACT PRECAUTIONS are not recommended for localized Zoster in the community but are instituted for hospitalized pts

30
Zoster – Infectivity Immunocompromised Pt w/ Either:
(1) Disseminated HZ (2) Local HZ in Pt at Risk for Dissemination Hospitalized, Strict Isolation Rx ~ Varicella (in which Airborne Spread is Possible)
 Disseminated HZ. (2) Local HZ in Pt at Risk for Dissemination. Hospitalized, Strict Isolation. Rx ~ Varicella (in which Airborne Spread is Possible)")
31
Herpes Zoster

32
Herpes Zoster

33
Herpes Zoster

34
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
35
Zoster Complications POSTHERPETIC NEURALGIA Ocular Neurologic
***Most Common*** (10-15%) Ocular Neurologic Motor Neuropathies – 2nd most common (2-3%) CN palsies Meningitis Myelitis Encephalitis Bacterial Superinfection Ramsey-Hunt Syndrome PHN – ~10-15% of pts w/ zoster will develop PHN -pts > 60 yo = 50% of cases -defined as persistence of sensory sx (pain, numbness, dysesthesias, allodynia) in affected dermatome for >30 days after rash onset -pain is 2o to injury of the peripheral nerves and altered CNS processing -RISK FACTORS: ↑ age, immunosuppression (HIV, transplant, connective tissue d/o’s) Occasionally zoster reactivation affects motor neurons in spinal cord and brain stem motor neuropathies -MOTOR NEUROPATHIES ARE NEXT MOST COMMON NEUROLOGIC COMPLICATION OF ZOSTER -segmental motor paresis develops in ~3% of pts w/ zoster -motor impairment occurs w/ pain and sensory ABNL in dermatomal distribution of rash -thought to be 2o to spread of VZV from DRG to anterior root/horn -onset coincides w/ development of pain and cutaneous eruption in dermatomal distribution -muscle atrophy may result -~75% have gradual recovery of motor strength -~25% have residual motor deficit **** PTS WHO DEVELOP PERIPHERAL MOTOR NEUROPATHY HAVE ↑ INCIDENCE OF UNDERLYING MALIGNANCY!!! -3-fold ↑ of underlying occult malignancy in pts who develop motor paresis in assoc w/ cutaneous zoster CN palsies – Predominantly partial or complete CN III palsies, then CN IV palsies, then Cn VI palsies, then BILATERAL palsies ~1/3 of pts w/ ophthalmological evidence of CN palsies had NO SX OTHER CN PALSIES include: (1) optic neuritis (may permanent visual loss) (2) facial paresis (RAMSEY HUNT SYNDROME) – peripheral facial palsy, hearing loss, vertigo or tinnitus Zoster is not always limited to a spinal nerve distribution but may also extend centrally meningeal inflammation and clinical meningitis -subclinical meningeal irritation (seen by CSF PLEOCYTOSIS) seen in 40-50% of cases TRANSVERSE MYELITIS – usually involves thoracic dermatomes -days to weeks following the initial onset of rash -present w/ unilateral motor and posterior column dysfnxn which evolves into paraplegia -freq complication in HIV pts -involves direct spread of VZV from DRG into spinal cord ENCEPHALITIS – typically presents w/ acute delirium within days of vesicular eruption but may occur prior to rash or up to 6 months after rash -majority of cases are in immunosuppressed pts -major risk factors include: -cranial or cervical dermatomal involvement, 2+ prior episodes of zoster, disseminated zoster, impaired cell-mediated immunity Major otologic complication of Zoster reactivation = Ramsey-Hunt Syndrome -linked to reactivation of latent VZV within geniculate ganglion with subsequent spread to CN VIII -TRIAD = (1) ipsilateral facial paralysis, (2) ear pain, (3) vesicles in auditory canal and auricle - taste perception, hearing (tinnitus, hyperacusis), lacrimation may also be affected -POLYCRANIAL NEUROPATHY freq. involving CN V, IX, X -Vertigo freq reported -Facial Paralysis is more severe than BELLS PALSY 2o to HSV – ↑ rates of late neural denervation, ↓ probability of complete recovery ↑ age was associated with PHN, bacterial superinfxn of the skin, ocular complications, and motor neuropathy Pts w/ 1 or more complications had more frequent co-morbidities (ie: DM, Ca, HIV, transplant recipient)
 Ocular. Neurologic. Motor Neuropathies – 2nd most common (2-3%) CN palsies. Meningitis. Myelitis. Encephalitis. Bacterial Superinfection. Ramsey-Hunt Syndrome. PHN – ~10-15% of pts w/ zoster will develop PHN. -pts > 60 yo = 50% of cases. -defined as persistence of sensory sx (pain, numbness, dysesthesias, allodynia) in affected dermatome for >30 days after rash onset. -pain is 2o to injury of the peripheral nerves and altered CNS processing. -RISK FACTORS: ↑ age, immunosuppression (HIV, transplant, connective tissue d/o’s) Occasionally zoster reactivation affects motor neurons in spinal cord and brain stem motor neuropathies. -MOTOR NEUROPATHIES ARE NEXT MOST COMMON NEUROLOGIC COMPLICATION OF ZOSTER. -segmental motor paresis develops in ~3% of pts w/ zoster. -motor impairment occurs w/ pain and sensory ABNL in dermatomal distribution of rash. -thought to be 2o to spread of VZV from DRG to anterior root/horn. -onset coincides w/ development of pain and cutaneous eruption in dermatomal distribution. -muscle atrophy may result. -~75% have gradual recovery of motor strength. -~25% have residual motor deficit. **** PTS WHO DEVELOP PERIPHERAL MOTOR NEUROPATHY HAVE ↑ INCIDENCE OF UNDERLYING MALIGNANCY!!! -3-fold ↑ of underlying occult malignancy in pts who develop motor paresis in assoc w/ cutaneous zoster. CN palsies – Predominantly partial or complete CN III palsies, then CN IV palsies, then Cn VI palsies, then BILATERAL palsies. ~1/3 of pts w/ ophthalmological evidence of CN palsies had NO SX. OTHER CN PALSIES include: (1) optic neuritis (may permanent visual loss) (2) facial paresis (RAMSEY HUNT SYNDROME) – peripheral facial palsy, hearing loss, vertigo or tinnitus. Zoster is not always limited to a spinal nerve distribution but may also extend centrally meningeal inflammation and clinical meningitis. -subclinical meningeal irritation (seen by CSF PLEOCYTOSIS) seen in 40-50% of cases. TRANSVERSE MYELITIS – usually involves thoracic dermatomes. -days to weeks following the initial onset of rash. -present w/ unilateral motor and posterior column dysfnxn which evolves into paraplegia. -freq complication in HIV pts. -involves direct spread of VZV from DRG into spinal cord. ENCEPHALITIS – typically presents w/ acute delirium within days of vesicular eruption but may occur prior to rash or up to 6 months after rash. -majority of cases are in immunosuppressed pts. -major risk factors include: -cranial or cervical dermatomal involvement, 2+ prior episodes of zoster, disseminated zoster, impaired cell-mediated immunity. Major otologic complication of Zoster reactivation = Ramsey-Hunt Syndrome. -linked to reactivation of latent VZV within geniculate ganglion with subsequent spread to CN VIII. -TRIAD = (1) ipsilateral facial paralysis, (2) ear pain, (3) vesicles in auditory canal and auricle. - taste perception, hearing (tinnitus, hyperacusis), lacrimation may also be affected. -POLYCRANIAL NEUROPATHY freq. involving CN V, IX, X. -Vertigo freq reported. -Facial Paralysis is more severe than BELLS PALSY 2o to HSV – ↑ rates of late neural denervation, ↓ probability of complete recovery. ↑ age was associated with PHN, bacterial superinfxn of the skin, ocular complications, and motor neuropathy. Pts w/ 1 or more complications had more frequent co-morbidities (ie: DM, Ca, HIV, transplant recipient)")
36
Zoster Ophthalmicus

37
Zoster – Motor Paresis

38
Zoster – Motor Paresis

39
Zoster – Motor Paresis

40
Zoster – Bacterial Superinfection

41
Ramsey-Hunt Syndrome

42
Zoster Complications – Immunosuppressed
Includes: HIV-infected pts Transplant Recipients Hematologic Malignancies ↑↑↑ Risk for Severe Complications Cutaneous Dissemination Visceral Involvement Pneumonitis, Hepatitis, Pancreatitis, Meningo-encephalitis

43
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
44
Uncomplicated Herpes Zoster Treatment
Antiviral Therapy Goals: (1) Promote Rapid Healing (2) ↓ Severity and Duration of Pain (3) ↓ Incidence and Severity of PHN Prompt Use of Anti-Virals ↓ Duration of Pain by ½ ↓ Overall Incidence of PHN Goals of antiviral Rx = (1) promote rapid healing of skin lesions, (2) lessen severity and duration of pain assoc w/ acute neuritis, (3) reduce the incidence or severity of PHN Prompt use of antiviral Rx appears to ↓ duration of pain by ~ ½ and reduce overall incidence of PHN!
 Promote Rapid Healing. (2) ↓ Severity and Duration of Pain. (3) ↓ Incidence and Severity of PHN. Prompt Use of Anti-Virals. ↓ Duration of Pain by ½. ↓ Overall Incidence of PHN. Goals of antiviral Rx = (1) promote rapid healing of skin lesions, (2) lessen severity and duration of pain assoc w/ acute neuritis, (3) reduce the incidence or severity of PHN. Prompt use of antiviral Rx appears to ↓ duration of pain by ~ ½ and reduce overall incidence of PHN!")
45
Acyclovir Oral Acyclovir 800 mg 5X/day Within 48-72 Hrs of Rash Onset
Excellent Safety Profile Mainstay of Rx BUT: Poor Bioavailability Frequent Dosing Within Hrs of Rash Onset Accelerates Resolution of Pain (Esp. in Pts > 50 yo) 1 Meta-Analysis – Sig. ↓ in PHN at 6 months by 46% Archives of Internal Medicine Vol 157 Apr 28, 1997, pp ACV has an excellent safety profile but is only moderately effective against VZV in vitro ACV has been the mainstay of Rx but (1) poor bioavailability, (2) frequent dosing prompted design of newer antiviral agents w/ improved pharmacokinetics (VALACYCLOVIR, FAMCICLOVIR) ACV used within Hrs of onset of rash (1) resolution of pain associated with acute neuritis – ESPECIALLY in pts > 50 yo (2) significant reduction in incidence of PHN at 6 months by 46%!!
 1 Meta-Analysis – Sig. ↓ in PHN at 6 months by 46% Archives of Internal Medicine Vol 157 Apr 28, 1997, pp ACV has an excellent safety profile but is only moderately effective against VZV in vitro. ACV has been the mainstay of Rx but (1) poor bioavailability, (2) frequent dosing. prompted design of newer antiviral agents w/ improved pharmacokinetics (VALACYCLOVIR, FAMCICLOVIR) ACV used within Hrs of onset of rash (1) resolution of pain associated with acute neuritis – ESPECIALLY in pts > 50 yo. (2) significant reduction in incidence of PHN at 6 months by 46%!!")
46
Acyclovir with Corticosteroids
Rx of Uncomplicated Acute HZ Study: ACV 800 mg po 5X/day X 21 days + Prednisone X 21 days ACV + Placebo Prednisone + Placebo 2 Placebos ACV + Prednisone: Less Time to Crusting, Healing, Sleep, Return to Prior Activity Faster Resolution Acute Neuralgia Earlier D/C of Analgesics Drawbacks ACV with corticosteroids has been used in an attempt to: (1) improved QOL (2) improve time to healing of lesions (3) ↓ incidence of PHN 1 study compared ACV + Prednisone vs variations of the 2 study end points were at 1 month and 6 months (1) ACV + Pred significantly accelerated times to total crusting, total healing (2) 2X as likely to return to uninterrupted sleep (3) 3X as likely to return to 100% of prior activity and discontinue analgesics DRAWBACKS – Benefits considered modest – Adverse effects more frequently reported in steroid recipients compared with ACV alone!! OF NOTE!! No studies involving STEROID THERAPY has found an effect on INCIDENCE or DURATION of PHN!!!
 improved QOL. (2) improve time to healing of lesions. (3) ↓ incidence of PHN. 1 study compared ACV + Prednisone vs variations of the 2 study end points were at 1 month and 6 months. (1) ACV + Pred significantly accelerated times to total crusting, total healing. (2) 2X as likely to return to uninterrupted sleep. (3) 3X as likely to return to 100% of prior activity and discontinue analgesics. DRAWBACKS – Benefits considered modest – Adverse effects more frequently reported in steroid recipients compared with ACV alone!! OF NOTE!! No studies involving STEROID THERAPY has found an effect on INCIDENCE or DURATION of PHN!!!")
47
Valacyclovir Valacyclovir 1000 mg po tid X 7-14 days vs. ACV
Accelerated Resolution of Pain 38 days vs. 51 days ↓ Duration of PHN Similar Adverse Events Valacyclovir is WELL ABSORBED from GI tract, rapidly converted to ACV 3-5-fold ↑ in ACV bioavailability Study in immunocompetent pts w/ herpes zoster > 50 yo – COMPARED w/ ACV 800 mg po 5X/day X 7 days (1) significantly accelerated resolution of zoster-associated pain compared w/ ACV (38 days vs 51 days) (2) significantly reduced duration of PHN (3) similar adverse events
 significantly accelerated resolution of zoster-associated pain compared w/ ACV (38 days vs 51 days) (2) significantly reduced duration of PHN. (3) similar adverse events.")
48
Anti-Viral Recommendations
Initiate w/in 72 hrs Esp. in Pts > 50 yo In Pts < 50 yo, Consider Risk Factors for Developing PHN Valacyclovir 1000 mg po tid X 7 days More Rapid Resolution Acute Neuritis Shorter Duration of PHN Lower Pill Burden Improved Compliance BUT ↑ $$$ Higher Cost than ACV RECOMMENDATIONS: Antiviral therapy should be initiated within 72 hours of the onset of rash IN PTS > 50 yo to MAXIMIZE POTENTIAL BENEFITS OF RX In pts < 50 yo, CONSIDER INDIVIDUAL CASES – CONSIDER risk factors for PHN!! Ie: severity of acute pain and rash, hx/o prodromal pain RECOMMEND Valacyclovir for 3 reasons (1) more rapid resolution of acute neuritis vs ACV (2) shorter duration of PHN vs. ACV (3) lower pill burden than ACV better compliance BUT!!! Is more expensive – if cost is an issue, may consider ACV 800 mg po 5X/day X 7-10 days
 more rapid resolution of acute neuritis vs ACV. (2) shorter duration of PHN vs. ACV. (3) lower pill burden than ACV better compliance. BUT!!! Is more expensive – if cost is an issue, may consider ACV 800 mg po 5X/day X 7-10 days.")
49
Anti-Viral Recommendations
Steroids Have Only Been Studied w/ ACV Moderate Acceleration of Healing and Resolution of Pain No Effect on PHN ↑ Adverse Effects w/ Steroids May ↑ Risk of Bacterial Superinfection Recommend Prednisone 40 mg Taper over 7-10 days ONLY in Pts: (1) w/ Severe Sx at Onset (2) w/o Specific Contraindication Last Dose Should Coincide w/ End of Anti-Viral Rx STEROIDS have only been studied with ACV – uncertain whether they would be more effective with Valacyclovir -things to consider – moderate acceleration of healing and resolution of pain associated with acute neuritis BUT!! No effect on development of PHN AND ↑ adverse side effects are reported with steroids!! AND may ↑ risk of bacterial superinfection!! Prednisone only in pts w/ severe symptoms at initial presentation, and pts w/o specific contraindication to steroid use Last dose should coincide with end of antiviral therapy!! OR continuing steroid Rx after antiviral drugs have been discontinued could promote viral replication viremia!!
 w/ Severe Sx at Onset. (2) w/o Specific Contraindication. Last Dose Should Coincide w/ End of Anti-Viral Rx. STEROIDS have only been studied with ACV – uncertain whether they would be more effective with Valacyclovir. -things to consider – moderate acceleration of healing and resolution of pain associated with acute neuritis. BUT!! No effect on development of PHN AND ↑ adverse side effects are reported with steroids!! AND may ↑ risk of bacterial superinfection!! Prednisone only in pts w/ severe symptoms at initial presentation, and pts w/o specific contraindication to steroid use. Last dose should coincide with end of antiviral therapy!! OR continuing steroid Rx after antiviral drugs have been discontinued could promote viral replication viremia!!")
50
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
51
Zoster – Prevention Major Precipitant for Zoster Reactivation?
Decline in Cell-Mediated Immunity! Elderly Population Immunosuppressed Pts Subclinical VZV Infection Enhanced VZV Cell-Mediated Immunity! Prevention in Immunosuppressed Hosts? ACV – ↓ Re-Activation in Hematopoietic Cell Transplant Recipients A decline in cell-mediated immunity – seen in elderly pts, immunosuppressed pts – is regarded as the major precipitant for inducing Zoster reactivation SUBCLINICAL VZV Infection – occurs periodically w/ exposure to virus ↑ Cell-Mediated Immunity responses limit spread of VZV prevents cutaneous VZV replication!! OCCURS IN: Immunosuppressed pts w/ asymptomatic varicella viremia Immunocompetent immune adults w/ household exposures to children with primary varicella GET A BOOST OR ENHANCED CELL MEDIATED IMMUNITY!!! Prevention in Immunosuppressed Hosts Study showed that ACV was effective in reducing VZV reactivation in hematopoietic cell transplant recipients ACV prophylaxis was well-tolerated VZV occurred most frequently in pts who required continued systemic immunosuppression!! So pts requiring ongoing or intensive immunosuppression in post-transplant period may benefit from cont. duration of ACV prophylaxis to prevent reactivation

52
Varicella Vaccine Concerns
(1) ↑ Risk of Vaccine-Assoc. Zoster Esp. in Immunocompromised Children (2) ↑ Zoster in General Population ↓ Circulation Wild-Type Virus ↓ in Cell-Mediated Immunity Neither Concern Has Been Proven Correct Varicella vaccine is composed of the Oka strain of live, attenuated VZV – high seronegative conversion rate Concerns that vaccination increased vaccine-associated zoster (esp in immunocompromised children) and increased zoster in the general population (2o to decreased circulation of wild-type virus and decline in T cell immunity)
 ↑ Risk of Vaccine-Assoc. Zoster. Esp. in Immunocompromised Children. (2) ↑ Zoster in General Population. ↓ Circulation Wild-Type Virus. ↓ in Cell-Mediated Immunity. Neither Concern Has Been Proven Correct. Varicella vaccine is composed of the Oka strain of live, attenuated VZV – high seronegative conversion rate. Concerns that vaccination increased vaccine-associated zoster (esp in immunocompromised children) and increased zoster in the general population (2o to decreased circulation of wild-type virus and decline in T cell immunity)")
53
Varicella Vaccine in Older Adults
2 Clinical Trials in Older Pts (55-87 yo) ↑ CMI to VZV after Immunization ↑ Freq. of VZV-Specific T-cells 1 in 68,000 1 in 40,000 Similar ratio to yo!
 ↑ CMI to VZV after Immunization. ↑ Freq. of VZV-Specific T-cells. 1 in 68,000 1 in 40,000. Similar ratio to yo!")
54
Zoster Vaccine Randomized, Double-Blind Placebo-Controlled Trial
38,546 Pts, 60 yo or Older Goal: Determine if Vaccine Would: ↓ Incidence and Severity of Zoster and PHN Results: (1) ↓ Incidence of Zoster by 51% (2) ↓ Incidence of PHN by 67% (3) Those Who Developed Zoster: Sig. Shorter Duration of Pain and Discomfort New England Journal of Medicine June 2, 2005, Vol 352 No 22, pp
 ↓ Incidence of Zoster by 51% (2) ↓ Incidence of PHN by 67% (3) Those Who Developed Zoster: Sig. Shorter Duration of Pain and Discomfort. New England Journal of Medicine June 2, 2005, Vol 352 No 22, pp")
55
Zoster Vaccine

56
Zoster Vaccine Do Not Use In: NOT Advised In:
Pregnant ♀ Pts w/ hx/o Anaphylactic Rxn to Gelatin or Neomycin NOT Advised In: Pts w/ 1o or Acquired Immunodeficiencies AIDS Leukemia Lymphoma Malignancies of Bone Marrow or Lymphatic System Pts on Immunosuppressive Therapies NOT for Rx of Zoster or PHN

57
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
58
Post-Herpetic Neuralgia
Acute Herpetic Neuralgia Pain Preceding or Accompanying Rash Up to 30 Days from Onset Subacute Herpetic Neuralgia Pain Persisting Beyond Healing of Rash Resolves w/in 4 mos of Onset Post-Herpetic Neuralgia Pain Persisting Beyond 4 mos from Initial Onset of Rash

59
Post-Herpetic Neuralgia – Epidemiology
Incidence ↑ w/ Advanced Age Rare in Children Pts < 60 yo – Risk is < 2% PHN is rare in children In adults < 60 yo, risk of PHN is estimated to be < 2% 1 study: 334 pts from yo, PHN = 6.9% 308 pts >= 70 , PHN = 18.5%!!

60
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
61
PHN Risk Factors Older Age Greater Acute Pain Greater Rash Severity
Assoc w/ ↑ Severity and Persistence of Sx Greater Acute Pain Greater Rash Severity ♀ Sex Presence of a Prodrome Risk is NOT ↑ in Immunocompromised Individuals

62
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
63
PHN – Clinical Manifestations
Pain Acute Zoster – Sharp, Stabbing PHN – Burning Allodynia > 90% of pts Anesthesia Deficits of Thermal, Tactile, Pinprick, Vibration Beyond Dermatomal Margins Pain associated with ACUTE ZOSTER = described as sharp, stabbing Pain associated with PHN = burning pain >90% of pts will also have allodynia = pain evoked by normally nonpainful stimuli (ie: Light Touch) Pts w/ PHN also have areas of ANESTHESIA (to thermal, tactile, pinprick and vibration sense) within affected dermatomes SENSORY DEFICITS may extend beyond dermatomal margins ALLODYNIA = most prominent in areas of RELATIVELY PRESERVED SENSATION SPONTANEOUS PAIN = most predominant within area of LOST OR IMPAIRED SENSATION
 Pts w/ PHN also have areas of ANESTHESIA (to thermal, tactile, pinprick and vibration sense) within affected dermatomes. SENSORY DEFICITS may extend beyond dermatomal margins. ALLODYNIA = most prominent in areas of RELATIVELY PRESERVED SENSATION. SPONTANEOUS PAIN = most predominant within area of LOST OR IMPAIRED SENSATION.")
64
PHN (1) Allodynia (2) Cutaneous Scarring
(3) ↓ Sensation to Pinprick, Cold, Touch
 ↓ Sensation to Pinprick, Cold, Touch.")
65
PHN

66
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
67
PHN – Pathogenesis Theories
(1) Sensitized Nociceptors “ABC syndrome” (2) “Sensitization-like” Characteristics (3) Neuroma Formation (4) Central Hypersensitivity ~ “Trickle” Current (5) ABNL “Epileptiform” Activity in Spinal Neurons MULTIDETERMINATE! Therapeutic Implications It is possible that sensitized nociceptors fail to return to NL after inflammation subsides -has been referred to as the “ABC syndrome” = “angry, backfiring C-nociceptors” -hallmark of this syndrome = vasodilatation 2o to release of neuropeptides (ie: Substance P) from active C-fiber nociceptors -can see skin warming -Those nociceptors that survive damage to the nerve that they travel in may acquire ABNL “sensitization-like” characteristics (not continuously sensitized) -ABNL sensitivity to NE, sympathetic efferent activity, or plasma catecholamines spontaneous and stimulus-evoked pain sensations -may be why PHN responds to transdermal ASA and Lidocaine Regenerating primary afferent fibers that survive may form NEUROMAS when attempting to reacquire their original peripheral targets 2o to extensive fibrosis within the nerve ABNL nociceptor-evoked central hypersensitivity: ongoing nociceptor discharge dynamically maintains central hyperexcitable state ~ “trickle” current maintaining charge on a battery ABNL epileptiform activity in spinal neurons may be 2o to: (1) death of primary afferent neurons degeneration of intraspinal terminal arbors deprives spinal neurons of synapses ABNL epileptiform activity – UNSURE WHETHER SHINGLES HAS THE SAME EFFECT – SPECULATIVE (2) glial scarring and death of intrinsic spinal neurons 2o to inflammation and spread of virus through the spinal cord atrophy of spinal gray matter epileptiform activity in remaining spinal neurons ALTHOUGH THE EXACT PATHOGENESIS OF PHN IS NOT CERTAIN – IT IS LIKELY MULTIDETERMINATE! AND it has 2 Principal therapeutic implications! (1) treat acute pain of shingles aggressively – especially in older pt who is prone to develop PHN -may ↓ the initiation phase of nociceptor-evoked central hypersensitivity and ↓ probability of ABNL central processing (2) consideration should be given to a 2-pronged Rx strategy aimed at CENTRAL and PERIPHERAL pain mechanisms ie: topical lidocaine AND tricyclic antidepressant
 Sensitized Nociceptors. ABC syndrome (2) Sensitization-like Characteristics. (3) Neuroma Formation. (4) Central Hypersensitivity. ~ Trickle Current. (5) ABNL Epileptiform Activity in Spinal Neurons. MULTIDETERMINATE! Therapeutic Implications. It is possible that sensitized nociceptors fail to return to NL after inflammation subsides. -has been referred to as the ABC syndrome = angry, backfiring C-nociceptors -hallmark of this syndrome = vasodilatation 2o to release of neuropeptides (ie: Substance P) from active C-fiber nociceptors. -can see skin warming. -Those nociceptors that survive damage to the nerve that they travel in may acquire ABNL sensitization-like characteristics (not continuously sensitized) -ABNL sensitivity to NE, sympathetic efferent activity, or plasma catecholamines. spontaneous and stimulus-evoked pain sensations. -may be why PHN responds to transdermal ASA and Lidocaine. Regenerating primary afferent fibers that survive may form NEUROMAS when attempting to reacquire their original peripheral targets 2o to extensive fibrosis within the nerve. ABNL nociceptor-evoked central hypersensitivity: ongoing nociceptor discharge dynamically maintains central hyperexcitable state ~ trickle current maintaining charge on a battery. ABNL epileptiform activity in spinal neurons may be 2o to: (1) death of primary afferent neurons degeneration of intraspinal terminal arbors deprives spinal neurons of synapses ABNL epileptiform activity – UNSURE WHETHER SHINGLES HAS THE SAME EFFECT – SPECULATIVE. (2) glial scarring and death of intrinsic spinal neurons 2o to inflammation and spread of virus through the spinal cord atrophy of spinal gray matter epileptiform activity in remaining spinal neurons. ALTHOUGH THE EXACT PATHOGENESIS OF PHN IS NOT CERTAIN – IT IS LIKELY MULTIDETERMINATE! AND it has 2 Principal therapeutic implications! (1) treat acute pain of shingles aggressively – especially in older pt who is prone to develop PHN. -may ↓ the initiation phase of nociceptor-evoked central hypersensitivity and ↓ probability of ABNL central processing. (2) consideration should be given to a 2-pronged Rx strategy aimed at CENTRAL and PERIPHERAL pain mechanisms. ie: topical lidocaine AND tricyclic antidepressant.")
68
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
69
Prevention of PHN (1) Rx of Acute Zoster (2) Vaccine OR:
Very Early Rx w/ Preventive Pain Medicines ie: TCAs, Anticonvulsants Epidural Steroid Injections w/ Anesthetics No Benefit Recommendation: Low-dose TCA w/in 2 days Rash Onset, X 90 days Gabapentin (If Limited By S/E) PREVENTION OF PHN = (1) Rx of acute zoster OR (2) vaccine to ↓ incidence of acute zoster or PHN STUDY SHOWED: pts over age of 60 yo – treated with AMITRIPTYLINE within 48 HRS of onset of rash PRIMARY OUTCOME = Pain at 6 months REDUCED BY ½ in pts treated with AMITRIPTYLINE Some countries use ESI w/ local anesthetic to Rx acute zoster but there is NO BENEFIT in PREVENTION OF PHN!! RECOMMEND: low-dose tricyclic antidepressant (ie: amitriptyline 25 mg or nortriptyline 25 mg) within 2 days of onset of rash – continue for 90 days IF pt is ELDERLY and does not tolerate side effects of tricyclic (ie: orthostatic hypotension, anticholinergic) CONSIDER GABAPENTIN 1800 mg po daily X 90 days ONLY PROVEN IN ANIMAL MODEL TO PREVENT PHN!!
 PREVENTION OF PHN = (1) Rx of acute zoster OR (2) vaccine to ↓ incidence of acute zoster or PHN. STUDY SHOWED: pts over age of 60 yo – treated with AMITRIPTYLINE within 48 HRS of onset of rash. PRIMARY OUTCOME = Pain at 6 months. REDUCED BY ½ in pts treated with AMITRIPTYLINE. Some countries use ESI w/ local anesthetic to Rx acute zoster but there is NO BENEFIT in PREVENTION OF PHN!! RECOMMEND: low-dose tricyclic antidepressant (ie: amitriptyline 25 mg or nortriptyline 25 mg) within 2 days of onset of rash – continue for 90 days. IF pt is ELDERLY and does not tolerate side effects of tricyclic (ie: orthostatic hypotension, anticholinergic) CONSIDER GABAPENTIN 1800 mg po daily X 90 days. ONLY PROVEN IN ANIMAL MODEL TO PREVENT PHN!!")
70
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
71
Treatment of PHN Antidepressants Analgesics Capsaicin
Topical Lidocaine Anticonvulsants Intrathecal Corticosteroids NMDA Receptor Antagonists Cryotherapy Surgery

73
PHN – Tricyclic Antidepressants
Effective for PHN Mainstay of Rx Inhibit Re-uptake of NE and Serotonin ↑ Inhibition of Nociceptive Signals Study Amitriptyline vs. Lorazepam vs. Placebo Sig. More Effective for Moderate Pain Relief Sig. Correlation Btwn: Serum Amitriptyline levels & Degree of Pain Relief Tricyclics are effective for PHN and are thought of as the mainstay of therapy INHIBIT reuptake of NE and Serotonin in the CNS increased inhibition of nociceptive signals from the periphery Significantly more effective in providing moderate pain relief than Lorazepam or Placebo in a small study Significant correlation between serum amitriptyline levels and degree of pain relief!!

74
PHN – Tricyclic Antidepressants
Sig. Side Effects Esp. Sedation, Dry Mouth, Orthostatic Hypotension Nortriptyline vs. Amitriptyline Nortriptyline Better Tolerated but Similar Analgesic Action May be a Lag of Up To 3 Weeks Neurology (51) October 1998 pp Side Effects (especially Anticholinergic side effects like Dry mouth, sedation, orthostatic hypotension) limit pt acceptance of TCAs Nortriptyline BETTER TOLERATED BUT similar analgesic action as Amitriptyline May be a lag of UP TO 3 WEEKS before you see a reduction in pain!!
 October 1998 pp Side Effects (especially Anticholinergic side effects like Dry mouth, sedation, orthostatic hypotension) limit pt acceptance of TCAs. Nortriptyline BETTER TOLERATED BUT similar analgesic action as Amitriptyline. May be a lag of UP TO 3 WEEKS before you see a reduction in pain!!")
75
PHN – Analgesics ASA, NSAIDs – Limited Value Opioids Conclusions:
Randomized, Double-Blind, Placebo-Controlled, Crossover Opioid vs. Tricyclic vs. Placebo – 8 weeks each Conclusions: Opioids and TCAs Better than Placebo Trend toward Opioids but Not Statistically Sig. No Appreciable Effect on Cognition Noted w/ Opioids Tramadol More Effective than Placebo Neurology (59) October 2002, pp ; Pain 104 (2003) pp ASA and NSAIDS are of LIMITED VALUE in pts w/ Zoster or PHN OPIOIDS: study with either morphine (91 mg) or methadone (15 mg), and nortriptyline (89 mg) or desipramine (63 mg) TREND toward preference for OPIOIDS but not statistically significant
 October 2002, pp ; Pain 104 (2003) pp ASA and NSAIDS are of LIMITED VALUE in pts w/ Zoster or PHN. OPIOIDS: study with either morphine (91 mg) or methadone (15 mg), and nortriptyline (89 mg) or desipramine (63 mg) TREND toward preference for OPIOIDS but not statistically significant.")
76
PHN – Capsaicin Alkaloid Derivative from Seeds of Plants
(1) Enhances Substance P Release from C-fibers (2) Prevents Re-accumulation of Substance P Capsaicin is thought to produce analgesia by enhancing the release of NOCIGENIC PEPTIDE SUBSTANCE P FROM C-FIBERS THEN PREVENTS REACCUMULATION!!
 Enhances Substance P Release from C-fibers. (2) Prevents Re-accumulation of Substance P. Capsaicin is thought to produce analgesia by enhancing the release of NOCIGENIC PEPTIDE SUBSTANCE P FROM C-FIBERS. THEN PREVENTS REACCUMULATION!!")
77
PHN – Capsaicin Topical Application Appears to be Effective for PHN
Burning, Stinging, Erythema Intolerable in ~ 1/3 of Pts Appears to be Effective for PHN Moderate Relief when Applied QID 21% ↓ in Pain Score (vs. 6% w/ placebo) True Blinding is Impossible Pain 33 (1988) pp
 True Blinding is Impossible. Pain 33 (1988) pp")
78
PHN – Topical Lidocaine
Meta-analysis (2007) 2 Small Trials Pain Relief Modestly Greater than Placebo Recommendations: Insufficient Evidence to Recommend as 1st Line Agent May be Useful as Adjunctive Rx Cochrane Database for Systemic Reviews. 4,2007
 2 Small Trials. Pain Relief Modestly Greater than Placebo. Recommendations: Insufficient Evidence to Recommend as 1st Line Agent. May be Useful as Adjunctive Rx. Cochrane Database for Systemic Reviews. 4,2007.")
79
PHN – Anticonvulsants Esp. Useful in Lancinating Component of Pain
ie: CN V Neuralgia Commonly Used Anticonvulsants Phenytoin Carbamazepine Gabapentin Pregabalin

80
PHN – Gabapentin 2 Studies 1o Outcome 2o Outcome Side Effects
Statistically Sig. ↓ in Pain Score vs. Placebo 2o Outcome ↓ Sleep Interference Improved Mood, QOL Side Effects Somnolence, Dizziness **Most Common** Peripheral Edema, Infection Pain 94 (2001) pp ; JAMA December 2, 1998 Vol 280, No 21, pp 1st study – TOTAL DOSE 3600 mg/day 2nd study – TOTAL DOSE 1800 to 2400 mg/day OVERALL – WELL TOLERATED SIDE EFFECTS were more common in GABAPENTIN GROUP!!
 pp ; JAMA December 2, 1998 Vol 280, No 21, pp st study – TOTAL DOSE 3600 mg/day. 2nd study – TOTAL DOSE 1800 to 2400 mg/day. OVERALL – WELL TOLERATED. SIDE EFFECTS were more common in GABAPENTIN GROUP!!")
81
PHN – Pregabalin Structural Analog of GABA (~Gabapentin) Results:
Improvement in Sleep, ↓ in Pain 150 mg to 600 mg po QD Side Effects Dizziness, Somnolence, Dry Mouth Peripheral Edema, Weight Gain Schedule V Controlled Substance – Euphoria If d/c Taper Over 1 wk 2o to Withdrawal Sx Pain 109 (2004) pp 26-35; Neurology 60, April 2003, pp
 pp 26-35; Neurology 60, April 2003, pp")
82
PHN – Intrathecal Steroids
Study of 277 pts w/ intractable PHN for 1 yr+ Intrathecal Methylprednisolone + Lidocaine 1X/wk X 4 wks Intrathecal Lidocaine 1x/wk X 4 wks No Rx Regional Anesthesia and Pain Medicine, Vol 24, No 4, July-August 1999, pp

83
PHN – Intrathecal Steroids
Results: (1) >90% of pts in Steroid Group Had: Good/Excellent Pain Relief at 4 wks, 1 yr, 2 yrs (vs. 6% in Lidocaine Group, 4% in No Rx Group) (2) Allodynia – ↓ by > 70% in Steroid Group (Lidocaine – ↓ by 25%) (3) ↓ Need for Diclofenac in Steroid Group Potential for Serious Neurologic Side Effects Adhesive Arachnoiditis Meningitis Regional Anesthesia and Pain Medicine, Vol 24, No 4, July-August 1999, pp
 >90% of pts in Steroid Group Had: Good/Excellent Pain Relief at 4 wks, 1 yr, 2 yrs. (vs. 6% in Lidocaine Group, 4% in No Rx Group) (2) Allodynia – ↓ by > 70% in Steroid Group. (Lidocaine – ↓ by 25%) (3) ↓ Need for Diclofenac in Steroid Group. Potential for Serious Neurologic Side Effects. Adhesive Arachnoiditis. Meningitis. Regional Anesthesia and Pain Medicine, Vol 24, No 4, July-August 1999, pp")
84
PHN – NMDA Receptor Antagonists
Animal Data Excitatory AA NTs – Role in Maintenance of Chronic Pain NMDA Antagonists Relieve Neuropathic Pain IV Ketamine Modest Pain Relief At Doses Sedation, Dysphoria, Dissociative Episodes Dextromethorphan No Better than Placebo in PHN S/E – Ataxia, Sedation Neurology 48, May 1997, pp Animal data suggests that excitatory AA neurotransmitters play a role in the maintenance of chronic pain

85
PHN Treatment Recommendations
Tricyclic Antidepressants Amitriptyline Nortriptyline “Strong” Opioids Methadone Morphine Tramadol Anticonvulsants Pregabalin Gabapentin Topicals Lidocaine 5% Patch Capsaicin Intrathecal Methylprednisolone

86
PHN Treatment

87
Limitations to Rx of PHN

88
Overview (1)Herpes Zoster (2) PostHerpetic Neuralgia (3) EMG studies
Pathogenesis Epidemiology Natural History and Infectivity Complications Treatment Prevention (2) PostHerpetic Neuralgia Epidemiology Risk Factors Clinical Manifestations Pathogenesis Prevention Treatment (3) EMG studies
 PostHerpetic Neuralgia. Epidemiology. Risk Factors. Clinical Manifestations. Pathogenesis. Prevention. Treatment. (3) EMG studies.")
89
Herpes Zoster of Head and Limbs
158 Consecutive Cases, Head and Limbs Results: > ½ Sensory Axonal Neuropathy w/ NL or Only Slightly ↓ SNAP CV > 1/3 Motor Fiber Involvement 19% Clinically – Segmental Motor Paresis 17% Subclinical – by EMG 55% Improvement in Segmental Motor Paresis 2.5% Sensorimotor Axonal PN Severity of Peripheral Fiber Axonal Damage ↑ w/ Age Archives of Physical Medicine and Rehabilitation, Vol 83, September 2002, pp

90
Herpes Zoster of Head and Limbs

91
Electrophysiological Findings +/- PHN
23 Pts w/ PHN, 64 Pts w/o PHN All Pts had ↓ SNAP Amplitude Assoc w/ NL or Only Slightly ↓ CV No Correlation Btwn Severity of Axonopathy & PHN So – PHN Not 2o to Damage of Lg Diameter Sensory Fibers 10% had Segmental Paresis Additional 17% had EMG Evidence of Axonal Motor Damage No Sig. Diff. in EP Findings of Pts w/ or w/o PHN Electroencephalography an Clinical Neurophysiology 101 (1996) pp Electroencephalography and Clinical Neurophysiology, 101 (1996)
 pp Electroencephalography and Clinical Neurophysiology, 101 (1996)")
92
Electrophysiological Findings +/- PHN

93
Segmental Zoster Paresis of Limbs
Report of 3 Cases and Literature Review (1) PSW and Fibs in 40-50% of Cutaneous Zoster Subclinical Motor Involvement – Not Uncommon (2) Weakness Commonly Occurs w/in 2 wks of Rash (3) Proximal Weakness More Common Older Age May Be a Risk Factor (4) Motor Paresis – ↑ Freq. of Assoc w/ Malignant Dz NCS: ↓ SNAP and CMAP Amplitudes Antiviral Rx May Be Assoc w/ ↓ Incidence of HZ Paresis The Neurologist, Vol 13, Number 5, September 2007, pp
 PSW and Fibs in 40-50% of Cutaneous Zoster. Subclinical Motor Involvement – Not Uncommon. (2) Weakness Commonly Occurs w/in 2 wks of Rash. (3) Proximal Weakness More Common. Older Age May Be a Risk Factor. (4) Motor Paresis – ↑ Freq. of Assoc w/ Malignant Dz. NCS: ↓ SNAP and CMAP Amplitudes. Antiviral Rx May Be Assoc w/ ↓ Incidence of HZ Paresis. The Neurologist, Vol 13, Number 5, September 2007, pp")
94
Effects of Acyclovir Goal: Eval. Efficacy of ACV in:
↓ Incidence of: PHN, Motor Paresis, Peripheral Nerve Damage No Difference in Incidence of PHN ACV Group: Sig. ↓ in Clinically Evident Motor Paresis & ABNL EMGs Un-Rx Group: More Freq. ABNL in SNCS, MNCS, H-Reflex, Blink Reflex ACV May Be Assoc w/: ↓ Sensory Axonopathy, ↓ Motor Paresis BUT No Effect on PHN European Neurology, 1996;36:

95
Motor Involvement in Acute HZ
40 Pts w/ Acute HZ EMG ABNL in 53% – Fibs, PSWs In 62% EMG Findings were Subclinical Widespread ABNL Not Confined to Segment Invaded by Rash 7 Pts had Motor Paresis Muscle and Nerve, November 1997, pp

96
Conduction Block of VZV Neuropathy
Case Report: 64 yo ♀ w/ CML Acute HZ in R C6-C7 Dermatome Weakness in RUE – Not Confined to C6-C7 NCS: CB and CV Slowing in R Median Nerve in Forearm CB in R Radial Nerve Btwn Cubitus and Brachial Plexus EMG: Spontaneous Activity in R Triceps MRI: Extensive Lesions in Connective Tissue around FF Tendons & Muscles Along Median Nerve Improvement in CBs & MMT of APB w/ Prednisone Neurology, October 2003 (61) pp
 pp")
97
Conduction Block of VZV Neuropathy

98
Conduction Block in Forearm
29 yo ♂ w/ Left FA Numbness, Left Hand Weakness 9 Days After Onset Severe 1o Attack Varicella PE: (+) Weakness Left APB, OP, 1st/2nd Lumb L MCN nerve – Sensory Branch Hypesthesia No Atrophy, DTRs +2 MNCS: L Median (FA) – Partial CB (↓ CV, Absent F-wave) Elbow Mixed Median Nerve – ↓ on L (15.2 μV vs μV) SNCS: L Sensory Branch MCN – Absent, NL on R EMG: ↓ Interference Pattern L APB, (+) Fascics in APB J Neurol Neurosurg Psychiatry 2005;76:
 Weakness Left APB, OP, 1st/2nd Lumb. L MCN nerve – Sensory Branch Hypesthesia. No Atrophy, DTRs +2. MNCS: L Median (FA) – Partial CB (↓ CV, Absent F-wave) Elbow Mixed Median Nerve – ↓ on L (15.2 μV vs μV) SNCS: L Sensory Branch MCN – Absent, NL on R. EMG: ↓ Interference Pattern L APB, (+) Fascics in APB. J Neurol Neurosurg Psychiatry 2005;76:")
99
Conduction Block in Forearm
Explanation? (1) Median & Sensory MCN Share Cervical Roots → Lateral Cord (2) Close Anatomical Proximity in Arm 2o to Anatomical Variations Direct Spread of Virus Between Nerves (3) Indirect Spread from Purely Sensory MCN via Spinal Cord J Neurol Neurosurg Psychiatry 2005;76:
 Median & Sensory MCN Share Cervical Roots → Lateral Cord. (2) Close Anatomical Proximity in Arm 2o to Anatomical Variations. Direct Spread of Virus Between Nerves. (3) Indirect Spread from Purely Sensory MCN via Spinal Cord. J Neurol Neurosurg Psychiatry 2005;76:")
100
Thank You!

101
Thank You!

Similar presentations















 Robert C. Byrd Center for Rural Health Marshall University.>")




