Download presentation
Presentation is loading. Please wait.

1
SUTURELESS VAGINAL HYSTERECTOMY AN UPDATE…
By MOUNIR M. F. El-HAO , PROF OF OB & GYN.AIN SHAMS UNIVERSITY , CAIRO , EGYPT..

2
Sutureless Vaginal Hysterectomy.
The need for CHANGE ? Patient,s BENEFIT or surgeon’s EGO ? Better technique ? Better results ?

3
This technology depends on:
INTRODUCTION This technology depends on: Mechanical energy or pressure & electrical energy remodelling of the vessel tissue creating collagen seal out of native vessel protein (denature collagen and elastin in vessel wall). Levy B. & Emery L. (2003): Randomized Trial of Suture versus Electrosurgical Bipolar Vessel Sealing in Vaginal Hysterectomy. ACOG; 102(1):
. Levy B. & Emery L. (2003): Randomized Trial of Suture versus Electrosurgical Bipolar Vessel Sealing in Vaginal Hysterectomy. ACOG; 102(1):")
4
Rates Australia 40% USA 36% Italy 15.5% France 5.8%

5
Types Abdominal Vaginal LAVH LH TLH CISH MISH

6
INTRODUCTION A Cochrane review on the surgical approach to hysterectomy for benign gynaecological disease, published in 2006, concluded that : Vaginal hysterectomy should be performed in preference to abdominal hysterectomy, where possible. Johnson N.; Barlow D.; Lethaby A., et al. (2005): Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database of Systematic Reviews, Issue 2: CD
: Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database of Systematic Reviews, Issue 2: CD")
7
Route Abdominal 75% Vaginal 25%

8
The extent of laparotomy and vaginal surgery should be based on the
Surgeon Preference (Indication) Experience with abdominal and vaginal surgery
 Experience. with abdominal and vaginal surgery.")
9
vaginal hysterectomy Despite fastest and least expensive it is used in only 23% of the hysterectomies performed in the United States

10
INTRODUCTION Traditionally, many surgeons have avoided vaginal hysterectomy or used it only in carefully selected patients . WHY Kives S.L.; Levy B.S.; Levine R.L., et al. (2003): for the American Association of Gynaecologic Laparoscopists. Laparoscopic-assisted vaginal hysterectomy: J Am Assoc Gynaecol Laparosc: 10:135-8.
: for the American Association of Gynaecologic Laparoscopists. Laparoscopic-assisted vaginal hysterectomy: J Am Assoc Gynaecol Laparosc: 10:")
11
HAEMOSTASIS. Achieving hemostasis is fundamental in all surgical approaches. clips, staples, sutures, ultrasonic, and monopolar or bipolar coagulation.

12
EBVS electrosurgical bipolar vessel sealing
Seals vessels from 1 to 7 mm in diameter, Precise amount of bipolar energy and pressure to fuse collagen and elastin within the vessel walls. withstand a minimum of three times normal systolic pressure. Space requirements are less for EBVS

13
SEALING. Sealing is achieved with minimal sticking and charring.
Thermal spread to adjacent tissues is approximately 0.5 to 2 mm. The result is permanent.

14
In a study comparing the electrosurgical bipolar vessel sealing (EBVS) system to ultrasonic coagulation, bipolar coagulation, surgical clips, and sutures, the electrosurgical bipolar vessel sealing (EBVS) system created seals that (were stronger than the other energy-based ligation methods and comparable in strength with that of mechanical ligation techniques. )
 system created seals that (were stronger than the other energy-based ligation methods and comparable in strength with that of mechanical ligation techniques. )")
15
AIM OF THE WORK To assess the safety and efficacy of using the electrosurgical bipolar vessel sealing (EBVS) system for securing the pedicles during vaginal hysterectomy in comparison with the conventional method of securing the pedicles by suture ligation & does it permit the expansion of the spectrum of vaginal hysterectomy indications.
 system for securing the pedicles during vaginal hysterectomy in comparison with the conventional method of securing the pedicles by suture ligation & does it permit the expansion of the spectrum of vaginal hysterectomy indications.")
16
STUDY TEAM. MOUNIR FAWZY ELHAO, PROF KHALED IBRAHIM , A PROF.
IHAB SERAG, TUTOR. MOHAMMA ELLEITHY, A.TUTOR.

17
These new technologies also reduce the risk of adverse reactions:
Vessels sealed using autologous tissues are unlikely to have adverse responses to foreign materials, such as sutures, staples, or clips. Finally, the reduction in needle use reduces the potential for injury during vessel ligation. Although in skilled hands vaginal hysterectomy may be performed using standard techniques even in difficult patients, the electrosurgical bipolar vessel sealer technology should permit the less experienced vaginal surgeon an opportunity to expand the indications for vaginal hysterectomy

18
Setting: The study was carried out in Ain-shams University maternity Hospital. Study group: Women admitted for vaginal hysterectomy for benign disease. Type of the study: Prospective randomized Double blind controlled study.

19
Population: Includes 100 patients undergoing vaginal hysterectomy [divided into 4 groups]: Group L1: vaginal hysterectomy using electrosurgical bipolar vessel sealing system (EBVS) for securing the pedicles in the patients with the traditional indications for vaginal hysterectomy. Group S1: vaginal hysterectomy using traditional suturing for securing the pedicles in the patients with the traditional indications for vaginal hysterectomy. Group L2: vaginal hysterectomy using electrosurgical bipolar vessel sealing system (EBVS) for securing the pedicles in the challenging (difficult) vaginal hysterectomies. Group S2: vaginal hysterectomy using traditional suturing for securing the pedicles in the challenging (difficult) vaginal hysterectomies.
![Population: Includes 100 patients undergoing vaginal hysterectomy [divided into 4 groups]:](http://slideplayer.com/slide/234253/1/images/19/Population%3A+Includes+100+patients+undergoing+vaginal+hysterectomy+%5Bdivided+into+4+groups%5D%3A.jpg "Group L1: vaginal hysterectomy using electrosurgical bipolar vessel sealing system (EBVS) for securing the pedicles in the patients with the traditional indications for vaginal hysterectomy. Group S1: vaginal hysterectomy using traditional suturing for securing the pedicles in the patients with the traditional indications for vaginal hysterectomy. Group L2: vaginal hysterectomy using electrosurgical bipolar vessel sealing system (EBVS) for securing the pedicles in the challenging (difficult) vaginal hysterectomies. Group S2: vaginal hysterectomy using traditional suturing for securing the pedicles in the challenging (difficult) vaginal hysterectomies.")
20
Inclusion criteria for L1 & S1 groups:
1st or 2nd degree uterine descent. Uterine size < 10 weeks. Benign pathology. Multigravid patients. Vaginal canal should be ample. The posterior & lateral vaginal fornices should be wide and deep. Subpubic angles > 90°.

22
Inclusion criteria for L2 & S2 groups:
Benign pathology. No uterine descent. Vaginal canal should be adequate. The posterior & lateral vaginal fornices should be adequate. Subpubic angles = 70-90°. Uterine size weeks or previous uterine operation [caesarean section-myomectomy-surgery involving the tubes or the ovaries].

23
Then each patient in the study will be tested for the following endpoints
Operative time Operative blood loss Hospital stay. Any postoperative complications including: 1ry haemorrhage. 2ry haemorrhage. Postoperative infection and febrile morbidity. The need for readmission. The need for laparotomy

24
PILOT STUDY ON SVH. Started december 2004.
Patient fit for vaginal hysterectomy allocated sequentially randomised and blindly into two groups. Comparing the efficacy of bipolar vessel sealing technique with routine vaginal hysterectomy.

26
Results

27
PATIENTS Sample size Sample size 103 Women admitted for vaginal hysterectomy for benign disease were chosen according to calculations that indicated a sample size of 50 subjects in each treatment arm would have 80% power with 95% confidence to detect a 20% difference between procedure times with electrosurgical bipolar vessel sealer versus suture ligature.

28
haemostatic technique
Patients groups GROUP L= L 1+ L2 ELECTROSURGICAL BIPOLAR VESSEL SEALING (EBVS) GROUP S= S 1+ S2 TRADITIONAL SUTURE LIGATURE
 GROUP S= S 1+ S2. TRADITIONAL SUTURE LIGATURE.")
29
the number of gauzes

30
Complications were reported including:
METHODS Endpoints Complications were reported including: Need for blood transfusion. Urinary bladder injury. Need for laparotomy.

31
postoperative haemoglobin and haematocrit
METHODS postoperative haemoglobin and haematocrit Endpoints Measured 24 hours after the end of the procedure.

32
METHODS Statistical methods STATISTICAL METHODS Statistical analysis was done on a personal computer using the Statistical Package for Social Sciences version 12.0 (SPSS©v. 12.0, SPSS Inc., Chicago, IL).
.")
33
RESULTS & DISCUSSION

34
RESULTS EBVS Operative data OPERATIVE DATA In the current study, in about one third (33%) of the cases debulking techniques were required to complete the operation, salpingoophorectomy was done in 20 cases either unilateral or bilateral if needed according to the clinical situation.
 of the cases debulking techniques were required to complete the operation, salpingoophorectomy was done in 20 cases either unilateral or bilateral if needed according to the clinical situation.")
35
RESULTS EBVS Operative data Sometimes other gynaecological procedures like classical repair (CR), sacrospinous fixation (SSF), transobturator mesh (TOM) or transvaginal tape (TVT) were done after completing the vaginal hysterectomy for associated gynaecological indications.
, sacrospinous fixation (SSF), transobturator mesh (TOM) or transvaginal tape (TVT) were done after completing the vaginal hysterectomy for associated gynaecological indications.")
37
Group L compared with Group S
RESULTS Operative data TABLE 2 Group L compared with Group S Group L (n=50) Group S (n=53) P value Operative time (min) = median (range) Circumcision time 10 (5-20) 10 (5-20) 0.653 Pedicle dissection time 37.5 (10-115) 70 (30-135) < 0.001 Vault closure time 7.5 (5-15) 0.280 Total operative time 52.5 (25-125) 90 (50-240) Intraoperative blood loss (ml) = median (range) 230 (40-690) 360 ( ) Postoperative haemoglobin (gm/dl) = mean (SD) 9.9(1.6) 9.3(1.4) 0.033 Postoperative haematocrit (%)= mean (SD) 32 (4.8) 28.9 (4.3) < Data are median (range) or mean (SD). P < 0.05 denotes statistical significance.
 Group S. (n=53) P value. Operative time (min) = median (range) Circumcision time. 10 (5-20) 10 (5-20) Pedicle dissection time (10-115) 70 (30-135) < Vault closure time. 7.5 (5-15) Total operative time (25-125) 90 (50-240) Intraoperative blood loss (ml) = median (range) 230. (40-690) 360. ( ) Postoperative haemoglobin (gm/dl) = mean (SD) 9.9(1.6) 9.3(1.4) Postoperative haematocrit (%)= mean (SD) 32 (4.8) 28.9 (4.3) < Data are median (range) or mean (SD). P < 0.05 denotes statistical significance.")
38
Group L1 compared with Group S1
RESULTS Operative data TABLE 3 Group L1 compared with Group S1 Group L1 (n=26) Group S1 (n=28) P value Operative time (min) = median (range) Circumcision time 10 (5-15) 10 (5-20) 0.306 Pedicle dissection time 30 (10-60) 60 (30-80) < 0.001 Vault closure time 5 (5-15) 0.867 Total operative time 50 (25-75) 75 (50-95) Intraoperative blood loss (ml) = median (range) 190 (40-690) 290 ( ) 0.453 Postoperative haemoglobin (gm/dl) = mean (SD) 10.1 (1.4) 9.7(1.3) 0.226 Postoperative haematocrit (%)= mean (SD) 32.8(5.0) 29.4 (4.3) 0.006 Data are median (range) or mean (SD). P < 0.05 denotes statistical significance.
 Group S1. (n=28) P value. Operative time (min) = median (range) Circumcision time. 10 (5-15) 10 (5-20) Pedicle dissection time. 30 (10-60) 60 (30-80) < Vault closure time. 5 (5-15) Total operative time. 50 (25-75) 75 (50-95) Intraoperative blood loss (ml) = median (range) 190. (40-690) 290. ( ) Postoperative haemoglobin (gm/dl) = mean (SD) 10.1 (1.4) 9.7(1.3) Postoperative haematocrit (%)= mean (SD) 32.8(5.0) 29.4 (4.3) Data are median (range) or mean (SD). P < 0.05 denotes statistical significance.")
39
Group L2 compared with Group S2
RESULTS Operative data TABLE 4 Group L2 compared with Group S2 Group L2 (n=24) Group S2 (n=25) P value Operative time (min)= median (range) Circumcision time 5 (5-20) 0.841 Pedicle dissect time 50 (20-115) 85 (50-135) < 0.001 Vault closure time 10 (5-15) 10 (5-20) 0.049 Total operative time 72.5 (30-125) 100 (65-240) Intraoperative blood loss (ml) = median (range) 270 ( ) 425 ( ) < 0.024 Postoperative haemoglobin (gm/dl) = mean (SD) 9.7(1.8) 8.8(1.4) 0.054 Postoperative haematocrit (%)= mean (SD) 31.2(4.4) 28.5 (4.3) 0.025 Data are mean (SD) or median (range). P < 0.05 denotes statistical significance.
 Group S2. (n=25) P value. Operative time (min)= median (range) Circumcision time. 5 (5-20) Pedicle dissect time. 50 (20-115) 85 (50-135) < Vault closure time. 10 (5-15) 10 (5-20) Total operative time (30-125) 100 (65-240) Intraoperative blood loss (ml) = median (range) 270. ( ) 425. ( ) < Postoperative haemoglobin (gm/dl) = mean (SD) 9.7(1.8) 8.8(1.4) Postoperative haematocrit (%)= mean (SD) 31.2(4.4) 28.5 (4.3) Data are mean (SD) or median (range). P < 0.05 denotes statistical significance.")
40
RESULTS EBVS Operative data the current study, the intraoperative blood loss was significantly lower in Groups L, and L2 than groups S, and S2 correspondingly, the role of EBVS in reducing the operative blood loss was more pronounced in the difficult cases [Groups L2].

41
Conclusions

42
Patients who have indications for traditional vaginal hysterectomy do not need abdominal hysterectomy,or laparoscopic hysterectomy.

43
Post operative Pain. Deserves to be studied in a well controlled trial

44
WHY SVH? Good potentials. Easier. Quicker Bloodless. Less infection.
Less pain.

45
Intra operative. Time ,Bleeding and recovery are all shorter than average for other techniques.

46
Sutureless vaginal hysterectomy using electrosurgical bipolar vessel sealer is a good alternative to the use of sutures in routine vaginal hysterectomy.

47
When the competent surgeon is equipped with such devices, conversion of an abdominal hysterectomy to the vaginal route is both attainable and preferred.

48
RESULTS EBVS Operative data In the current study, the total operative time was significantly shorter in Groups L, L1 and L2 than groups S, S1 and S2 correspondingly and this shorting in the operative time resulted from shorting of the pedicle dissection time in Groups L, L1 and L2.

49
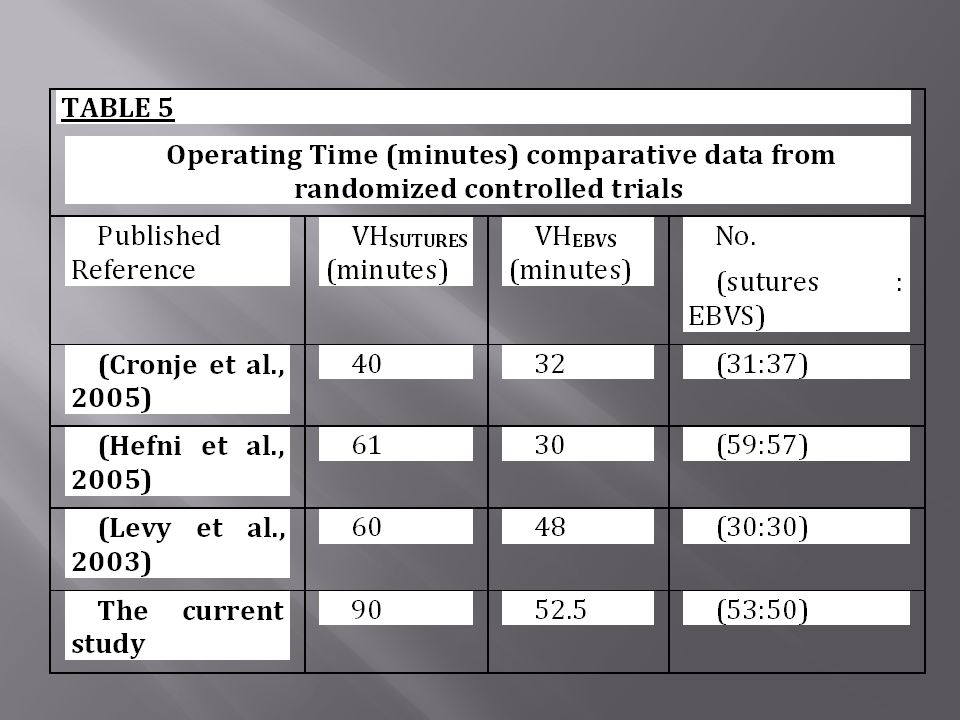
DISCUSSION EBVS Significant reductions in procedure time when using EBVS was found in the three RCTs. Levy B. & Emery L. (2003): Randomized Trial of Suture versus Electrosurgical Bipolar Vessel Sealing in Vaginal Hysterectomy. ACOG; 102(1): Cronje H.S. & de Coning E.C. (2005): Electrosurgical bipolar vessel sealing during vaginal hysterectomy. Int J Gynaecol Obstet; 91(3): Hefni M.A. (2005): Safety and efficacy of using the LigaSure vessel sealing system for securing the pedicles in vaginal hysterectomy: randomized controlled trial. BJOG 2005; 112(3):
: Randomized Trial of Suture versus Electrosurgical Bipolar Vessel Sealing in Vaginal Hysterectomy. ACOG; 102(1): Cronje H.S. & de Coning E.C. (2005): Electrosurgical bipolar vessel sealing during vaginal hysterectomy. Int J Gynaecol Obstet; 91(3): Hefni M.A. (2005): Safety and efficacy of using the LigaSure vessel sealing system for securing the pedicles in vaginal hysterectomy: randomized controlled trial. BJOG 2005; 112(3):")
50
RESULTS Postoperative data POSTOPERATIVE DATA There was no significant statistical difference between the comparison groups as regard the duration of hospital stay.

51
14 patients required hospitalization > 48 hours:
RESULTS EBVS Postoperative data 14 patients required hospitalization > 48 hours: 6 had some medical problems like diabetes mellitus or ischemic heart disease 8 had some complications related to the surgery like postoperative fever (4 patients) or major surgical complication (4 patients).
 or major surgical complication (4 patients).")
52
RESULTS Postoperative data There was no significant statistical difference between the comparison groups as regard the rate of occurrence of complications:

53
pain with EBVS could be related to:
Less manipulation, compression and traction. No foreign material; Tissue left distal to the suture or clip (including nerves) can necrose post-operatively and may cause pain and infection. Peirce S.C. & Crawford D.C. (2007): Centre for Evidence-based Purchasing; Purchasing and Supply Agency; Evidence review; Electrosurgical vessel sealing in vaginal hysterectomy. CEP November
 can necrose post-operatively and may cause pain and infection. Peirce S.C. & Crawford D.C. (2007): Centre for Evidence-based Purchasing; Purchasing and Supply Agency; Evidence review; Electrosurgical vessel sealing in vaginal hysterectomy. CEP November")
54
polypectomy Debulking techniques

55
coring Debulking techniques

56
morcellation Debulking techniques

57
Thank you for your attention.

Similar presentations







>")






 Mark K. Dodson, M.D. Professor Department of OB/Gyn Division of Gynecologic Oncology University of Utah.>")
,>")






