Download presentation
Presentation is loading. Please wait.

1
Other Mental Health Issues that Impact Learning
Stephanie Eken, M.D. Child and Adolescent Psychiatrist David Causey, Ph.D. Clinical Child Psychologist Square One: Specialists in Child and Adolescent Development

2
Symptoms, Treatment, & Impact on Learning
Mood Disorders: Symptoms, Treatment, & Impact on Learning

4
Why Should We Care? Mood disorders are prevalent and recurrent
May impact school performance May present with physical symptoms Poor psychosocial outcomes High risk for suicide High risk for substance abuse

5
Epidemiology of Depressive Disorders
Preschool: <1% School-age: 1-2% Female-to-male ratio 1:1 Adolescence: 6% Female-to-male ratio 2:1 Cumulative incidence by 18 yrs: 20% Hospitalized children: 20% Hospitalized adolescents: 40%

6
Most common stressors leading to youth suicide in Kentucky
Fight with Parent 20% End of a relationship 12% Financial problems 10% Fight with a significant other 8% Recent move, social isolation 7% Legal problems % Family Problems % Academic problems 5% Substance abuse % Homosexuality % Recent abuse % Other stressors 15%

7
Etiology of Depression
Neurobiology Dysregulation of serotonin & norepinephrine in CNS Influence of sex hormones Personality Negative cognitive style Environmental factors Abuse & neglect Stressful life events Family dysfunction

8
Genetics Children with a depressed parent are 3 times more likely to have MDD Children at high genetic risk may be more sensitive to adverse environmental experiences

9
Depression in Children
Irritability (more common than depressed mood) Boredom (anhedonia) Somatic complaints Stomachaches & headaches most common Anxiety Indecision Temper tantrums & disruptive behavior
 Boredom (anhedonia) Somatic complaints. Stomachaches & headaches most common. Anxiety. Indecision. Temper tantrums & disruptive behavior.")
10
Depression in Adolescents
Irritable or sad mood More likely to report a sad/depressed mood Increased sleep and appetite Increased suicidal ideation & attempts Increased impairment of functioning Increased behavioral problems Decreased energy Rejection sensitivity

12
Psychosocial Risk Factors for Depression
Family problems Conflict, maltreatment, parental loss/separation, parental mental illness Comorbid psychiatric disorders ADHD, anxiety d/o’s, conduct d/o, substance abuse Recent adverse events School, relationships, loss of social support Personality traits Anger, dependence, difficulty regulating affect

13
Is he sad or depressed? Feeling sad or “blue”
Temporary period in which a child feels sad in response to a major stressor Children may have transient depressed mood states Adjustment disorders to stressors Depression is more severe, lasts longer and impacts functioning

14
Adjustment Disorder Behavioral or emotional response to a identifiable cause or stress Symptoms occur within three months of the stressor Symptoms cause marked distress

15
Adjustment Disorder Associated with: Anxiety
Mixed anxiety and depressed mood Disturbance of mood and conduct Disturbance of conduct

16
Impact on Learning May change sleep or eating patterns
Difficulty concentrating/focusing Social isolation School behavior – fighting, arguments Academic difficulties can lead to changes in mood Consider an educational evaluation if treatment for depression does not resolve learning issues

17
School-based Interventions
Acknowledge the student’s feelings Provide a place for students to regroup if they feel weepy or fatigued Allow the student to stop an activity and resume it later when calm Encourage positive self-talk and break tasks down

18
School-based Interventions
Irritable Mood Model appropriate responses to replace irritable responses Allow the student to take him/herself out of a situation (self-timeout) when irritability is starting to disrupt others May want to work independently Provide opportunities for the student to "fix" problems or inappropriate classroom behaviors Fatigue Provide class notes to the student Identify study partners who can support and assist with assignments Grade the student based on work completed or attempted (rather than work assigned)
 when irritability is starting to disrupt others. May want to work independently. Provide opportunities for the student to fix problems or inappropriate classroom behaviors. Fatigue. Provide class notes to the student. Identify study partners who can support and assist with assignments. Grade the student based on work completed or attempted (rather than work assigned)")
19
Bipolar Disorder Increasingly diagnosed in children Risk factors
Lifetime prevalence = 1% Risk factors Early onset depression Psychosis Mood lability Seasonal pattern Family history of BD

20
Bipolar Disorder Increasingly diagnosed in children Genetics
If untreated, children/adolescents are at risk for substance abuse, school failure, accidents, incarceration and suicide

21
Bipolar Disorder Neurobiology Genetics Environmental factors
Neurotransmitters Neuroimaging shows subtle differences in frontal lobe and amygdala volume Genetics One parent with BD = 25% risk Environmental factors May potentiate genetic predisposition Stressors Low maternal warmth

23
Bipolar Disorder in Children
Mood may shift rapidly Minute-to-minute Day-to-day May present as chronic irritability or explosiveness with no discernible pattern or periods of wellness Different from depression by the presence of mania 20% of depressed children will go on to develop bipolar disorder

24
Mania in children Excessive irritability Excessively giddy or silly
Aggressive behaviors Extended, rageful tantrums Physically aggressive Restless or persistently active Age-inappropriate sexual interests Grandiosity

25
How does it impact school?
Fluctuations in cognitive abilities Impaired ability to plan, organize, concentrate and use abstract reasoning Heightened sensitivity to perceived criticisms Hostility or defiance with little provocation Emotions disproportionate to situation

26
School-based Interventions
Develop a simple explanation that the student and staff can use with peers and teachers Accommodate tardiness Allow the student to complete schoolwork or tests in a less stimulating environment Seat the student where the teacher can monitor, but not where the student is the focal "center of attention" Limit homework to a feasible amount during manic periods Allow the student to have homebound instruction during manic periods Allow children to discreetly and frequently accommodate needs caused by medication side effects

27
Treatment for Mood Disorders
Psychological interventions Individual therapy (CBT) Parent guidance sessions School-based counseling Biological interventions Medications Side effects may impact learning or behavior when starting medication
 Parent guidance sessions. School-based counseling. Biological interventions. Medications. Side effects may impact learning or behavior when starting medication.")
28
Childhood Anxiety Disorders

29
Anxiety Disorders Medical condition that causes people to feel persistently, uncontrollably worried over an extended period of time Limit children’s ability to engage in a variety of activities

30
Epidemiology of Anxiety Disorders
Most common emotional/behavioral disorder in childhood Incidence 10-15% of children/adolescents Female-to-male ratio Equal in preadolescent children Females are increasingly represented in adolescent years

31
Etiology of Anxiety Genetics Biologic Psychological
Central Nervous System (brain) Abnormal neurotransmitter functioning Serotonin, norepinephrine, GABA receptors Psychological Internal and external stressors overwhelm coping abilities
 Abnormal neurotransmitter functioning. Serotonin, norepinephrine, GABA receptors. Psychological. Internal and external stressors overwhelm coping abilities.")
32
Fear Alarm and agitation
Caused by expectation or realization of danger A state of dread or apprehension Webster’s II Dictionary, Third Ed.

33
Fear Immediate alarm reaction Basic, normal emotion
Essential to alert to imminent danger Focuses attention Prepare to respond: Flight or Fight Pounding heart, rapid breathing, muscle tension, sweating Consolidate experience to memory To learn appropriate response

34
Anxiety Apprehension of danger and dread Accompanied by
Restlessness Tension Rapid heart rate Shortness of breath Unattached to a clearly identifiable stimulus

35
When is anxiety pathologic?
Intensity of anxiety Out of proportion to threat Frequency of anxiety Increase in fear reaction and cannot be “reasoned away” Content of anxiety Seemingly innocuous situation or stimulus

36
Children with Anxiety Disorders
Risk for developing other types of anxiety disorders/or psychiatric disorders Comorbid psychiatric disorders Young children with GAD can also suffer from separation anxiety Depression can accompany the feeling of generalized anxiety Increased risk for adjustment difficulties in adulthood

37
Generalized Anxiety Disorder
Worry, worry, and more worry About – family, friends, health of others, natural disasters, school performance, etc. Somatic concerns Headaches, feeling shaky, sweating Not easily reassured May throw tantrums related to anxiety Poor concentration and attention May present for ADHD work-up

38
Separation Anxiety Excessive anxiety focused on separating from home or parent figure Most commonly diagnosed in prepubertal children More common in 5-7 and year olds with transition into elementary and middle school Typically occurs following a significant change or major life event

39
Separation Anxiety Expression varies with age
Prepubescent children (5-8 years) Clinging/shadowing behavior Nightmares Fear of loss of loved ones School refusal
 Clinging/shadowing behavior. Nightmares. Fear of loss of loved ones. School refusal.")
40
Separation Anxiety Preadolescent (9-12 years)
Emotional distress of separation Staying away from home overnight Adolescents (13-16 years) Somatic difficulties School refusal
 Somatic difficulties. School refusal.")
41
Social Phobia Excessive fear in social situations where child is exposed to unfamiliar people/evaluation by others Excessively self conscious/shy Tremendous concern about social failure/embarrassment/humiliation

42
Social Phobia Exposure causes significant anxiety/panic
Fear excessive and unreasonable Avoidance or endurance with extreme distress Interference in functioning

43
Selective Mutism Children either talk minimally or not at all in certain settings or situations that are part of their daily lives (e.g., school) Reflects underlying problems with anxiety Often inadvertently reinforced by other individuals (i.e., parents, friends) in the child’s daily life (e.g., speaking for the child, permitting the use of nonverbal communication, etc.). Considered an extreme form of social phobia
 in the child’s daily life (e.g., speaking for the child, permitting the use of nonverbal communication, etc.). Considered an extreme form of social phobia.")
44
Panic Attacks Sudden, discrete episodes of intense fear
Intense desire to escape Feeling of doom Activation of autonomic nervous system Fight or flight Duration minutes

45
Panic Disorder Recurrent panic attacks
Inter-episode worry about having a panic attack Worry about implications and consequences Changes in behavior More common in adolescents

46
Anxiety at School Frequent self-doubt and criticism
Seeking constant reassurance from the teacher Difficulty transitioning between home and school Avoidance of academic and peer activities Poor concentration

47
School-based interventions
Accommodate late arrivals Shorter school days to transition children with separation anxiety Allow extra time for transitions Provide alternative activities for children with somatic complaints Have a “safe” place if child develops increased anxiety or panic attacks Have an anti-worry plan

48
Components of a Simple Anti-Worry Plan
*What am I worried or afraid about? *How worried Am I? 2 Not at all A little worried A lot *How do we know that things will be OK? *What can I do to help myself not worry so much? *Is this something that I should worry about?

49
Defiance & Aggression

50
Defiance When is defiant behavior not really defiance to an authority figure….Never When is defiant behavior a result of something other than a defiant attitude?...When it’s a coping response to an underlying vulnerability, frustration, or disappointment (“solution” versus problem)
")
51
Two Types of Aggression
Proactive Aggression – aggression that is more organized and less impulsive, not necessarily emotional driven, and may be goal oriented. Reactive Aggression – more impulsive and resulting from overwhelming affect; quickly reaches threshold for inability to cope with the demands of the situation.

52
Cognitive Distortions in Angry Youth
Appraisal of internal arousal Cue Utilization Attributions Social Perceptions (self and others) Generating problem-solving solutions Considering Consequences Implementing Solutions Situational Appraisals
 Generating problem-solving solutions. Considering Consequences. Implementing Solutions. Situational Appraisals.")
53
Adult Issues That May Escalate an Anger Outburst
The adult’s mood at that moment Feelings of helplessness in managing difficult situations Expectations (or judgments) about the youth are already determined and influence the adult’s response to the current situation. Not being well prepared for managing the situations.
 about the youth are already determined and influence the adult’s response to the current situation. Not being well prepared for managing the situations.")
54
Quick to anticipate a conflict Quick to raise voice or yell
Specific adult behaviors that may increase the likelihood of an anger outburst Too quick to say “no” Quick to anticipate a conflict Quick to raise voice or yell Interpret behavior as intentional Don’t set limits when necessary Too strict with limits-can’t follow through Coercive Process

55
Situational Factors (Possible Anger Triggers):
“Antecedents” refers to those factors that precede and trigger a conflict or anger outburst. “Situation Specificity” refers to specific situations that are likely to raise frustration levels, lower coping thresholds, and make the youngster more vulnerable to the impact of an antecedent.

56
Specific student issues that may increase the likelihood of an anger outburst
Experiencing frustration and worry – interpret anger The occurrence of a real or perceived threat and/or adverse event Being teased, bumped in the hallway, threatened by another youth, etc. Obstacles to getting or doing what they want or expect Not feeling heard or understood Denied requests – don’t like to hear “no” Feeling unimportant and insignificant – such as being left out of something Some injustice occurs – e.g., the youth gets into trouble for something they didn’t do or didn’t initiate.

57
Other “High Risk” Situations
Medications wear off Blamed unjustly Academic frustration Embarrassed over a grade Picked on *Angry from home (“Carry Over”)
")
58
Purpose / Process in good anger control plans
Better self-regulation Effective use of language “Interactive Coping” – working with the student while maintaining authority “Firm Flexibility” – adult must be firm, clear, and consistent while ALSO being flexible, supportive, and collaborative with the student when appropriate.

59
Things to consider, explore, or examine when developing an anger plan
Clarification of the concerns or problems What’s behind the anger (feelings, issues) Ideal alternative attitudes and behaviors Benefits to them of positive behaviors and attitudes Costs to them of negative attitudes and behaviors High risk situations, antecedents (people, places, times, etc.)
 Ideal alternative attitudes and behaviors. Benefits to them of positive behaviors and attitudes. Costs to them of negative attitudes and behaviors. High risk situations, antecedents (people, places, times, etc.)")
60
Things to consider, explore, or examine when developing an anger plan
Things that can be done to prevent frustration when entering a high risk situation Things that can be done when frustration is present and/or escalating (i.e., 3-7) Calm down actions or de-escalation strategies that can and can’t be done Ways the adult can help with high-risk times Reinforcements and consequences if any Regular time to review how things are going Discussion of problem possibilities Completion of problem-solving sheet
 Calm down actions or de-escalation strategies that can and can’t be done. Ways the adult can help with high-risk times. Reinforcements and consequences if any. Regular time to review how things are going. Discussion of problem possibilities. Completion of problem-solving sheet.")
61
Mistakes adults sometimes make
Setting too many goals at one time Setting goals that are too lofty; it is sometimes better to begin with smaller more attainable goals, than to start with the obvious problem that needs to be eliminated. Measuring success by an absence of the problem, rather than recognizing a reduction in the problem. Scrapping a plan because “its not working”. Assuming the plan isn’t working because the youngster isn’t trying or doesn’t care about doing better.

62
Key Parts to a Problem-Solving Plan
“High risk” situations Feelings when this happens Angry thoughts that worsen my anger: What to do: Identify the problem Use good self talk Coping strategies What others can do to help Evaluate the process or how it could turn out

63
Positive Attention Things
PATs

64
Treatment of Mood & Anxiety Disorders

65
Talking with Parents Need to involved parents when the student experiences significant academic, social or emotional difficulties that interfere with learning Develop a shared understanding of child/adolescent Ask parents if they see concerning emotional or behavioral problems at home Parents may have effective strategies they use at home that can be implemented in the classroom

66
When to refer for further evaluation
Impact on learning Effecting social interactions Safety concerns Suicidal statements Threats toward others Concern for abuse/neglect Typical interventions do not work

67
Choosing Initial Treatment
Psychotherapy Individual Family – parental educations Psychopharmacologic Intervention Patients unable to participate in therapy due to severity of symptoms Comorbidity with other psychiatric illnesses Symptoms that do not respond to therapy

68
Goals of Treatment Safety Build alliance & instill hope
Clarify diagnosis Assess comorbidity (substance abuse, medical illness, other psych d/o’s) Assess motivation for treatment Availability of resources (e.g., partial hospital, day tx programs, outpt. tx)
 Assess motivation for treatment. Availability of resources (e.g., partial hospital, day tx programs, outpt. tx)")
69
Treatment Treatment is multimodal
Pharmacotherapy alone not effective due to psychosocial context of illness Address family, school, peer issues Psychotherapy for mild to moderate mood disorders (CBT, IPT, family therapy, psychodynamic) Consider medications
 Consider medications.")
70
Medications Depression/Anxiety Bipolar Disorder/Mood dysregulation
Antidepressants SSRIs Atypical antidepressants TCAs Bipolar Disorder/Mood dysregulation Mood stabilizers

71
Antidepressants Mechanism of Action Indications
Modulation of neurotransmitters Increase serotonin at 5-HT receptor Atypical antidepressants may modulate serotonin, norepinephrine and dopamine Indications Depression (unipolar/bipolar) Anxiety disorders Obsessive Compulsive Disorder Panic Disorder PTSD Bulimia Nervosa
 Anxiety disorders. Obsessive Compulsive Disorder. Panic Disorder. PTSD. Bulimia Nervosa.")
72
SSRIs No evidence that one SSRI is superior to another
First-line medication for depressive and anxiety disorders No evidence that one SSRI is superior to another SSRIs take 4-6 weeks to determine efficacy of dose Fewer side effects than older antidepressants

73
SSRIs FDA approved in children & adolescents
Fluoxetine Depression (age 8 and over) OCD (age 7 and over) Sertraline (Zoloft) – OCD (age 6 & over) Fluvoxamine (Luvox) – OCD (age 8 & over) Significant portion of psychiatric medications are prescribed “off-label” for use in pediatric population Off label use Paroxetine (Paxil) Citalopram (Celexa) Escitalopram (Lexapro)
 OCD (age 7 and over) Sertraline (Zoloft) – OCD (age 6 & over) Fluvoxamine (Luvox) – OCD (age 8 & over) Significant portion of psychiatric medications are prescribed off-label for use in pediatric population. Off label use. Paroxetine (Paxil) Citalopram (Celexa) Escitalopram (Lexapro)")
75
SSRI Side Effects that May Impact Learning
Common Gastrointestinal – dyspepsia, diarrhea CNS – headache, anxiety, insomnia Increased sweating Uncommon Akasthisia (inner feeling of restlessness) Agitation Mania (may occur in children with BD) May need to add additional agent to manage side effects
 Agitation. Mania (may occur in children with BD) May need to add additional agent to manage side effects.")
77
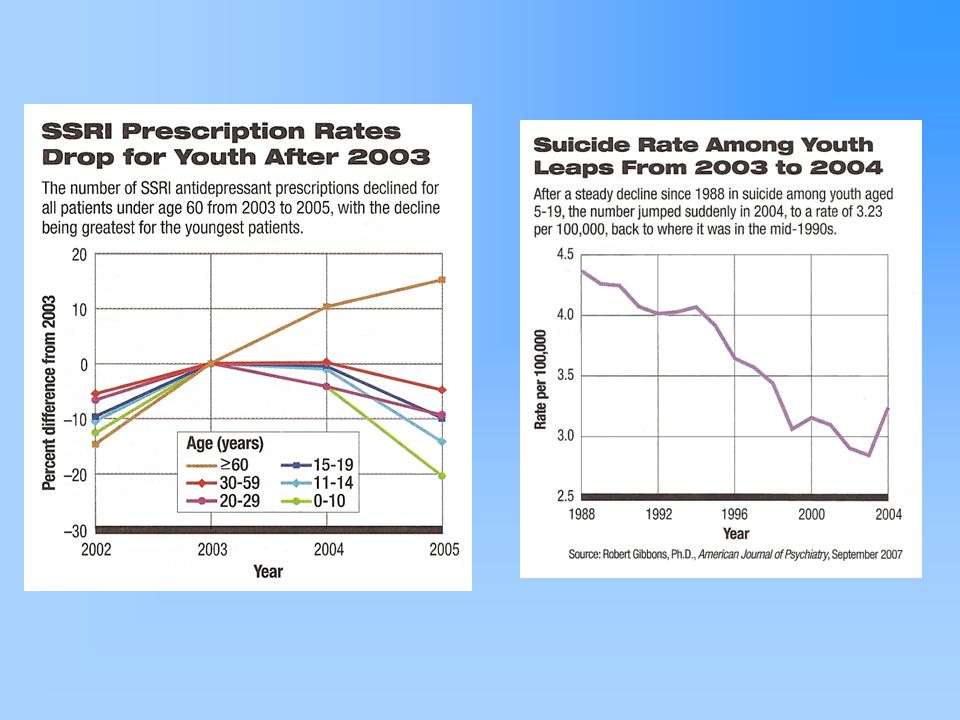
Antidepressant Black Box
The most serious warning possible on drug packaging in the USA To apply to ALL antidepressants for children and adolescents < 25 yrs old Explicit about the increased risk of suicide especially during the early phase of tx No completed suicides in studies reviewed Review of studies showed increased suicidal thoughts (2% to 4%) through adverse event reporting
 through adverse event reporting.")
78
Antidepressant Black Box
Children and adolescents must be monitored closely School officials should notify parent if student’s work reflects suicidal themes

80
Other Antidepressants
SNRIs Modulate serotonin and norepinephrine transmission Atypical Antidepressants May modulate serotonin, norepinephrine, and dopamine Can be used as single agent or as augmentation strategy with SSRI or other psychotropic Fewer studies in children & adolescents No FDA approved SNRIs in pediatric OCD

81
Side Effects SNRIs Atypical Antidepressants Venlafaxine (Effexor)
Elevated B/P - diastolic Duloxetine (Cymbalta) Blurred vision, mydriasis (dilated pupils – can affect vision) Atypical Antidepressants Mirtazapine (Remeron) Sedation Weight gain No sexual side effects
 Blurred vision, mydriasis (dilated pupils – can affect vision) Atypical Antidepressants. Mirtazapine (Remeron) Sedation. Weight gain. No sexual side effects.")
82
Mood Stabilizers Indications Mechanism of Action Early-onset bipolar
Anxiety OCD Explosive aggression Mechanism of Action Multiple Enhance GABA Block glutamate Second messengers

83
Mood Stabilizers Depakote Lithium Oxcarbazepine (Trileptal)
Gabapentin (Neurontin) Topirimate (Topamax) Migraine prophylaxis Psychiatric indications Mood stabilization Augmenting agent for treatment resistant OCD
 Topirimate (Topamax) Migraine prophylaxis. Psychiatric indications. Mood stabilization. Augmenting agent for treatment resistant OCD.")
84
Side Effects that may Impact School
Weight gain or loss Change in appetite Stomachaches Sedation Cognitive impairment Especially Topamax (processing speed)
")
85
Atypical Antipsychotics
Mechanism of action 5HT2A/D2 receptor antagonism Less TD and EPS symptoms than 1st generation Indications Psychosis/psychotic depression Mood stabilization – bipolar, mood dysregulation Aggressive behaviors – autism, MR, DD Augmenting agent for OCD Conduct problems Severe tic disorders

86
Atypical Antipsychotics
FDA approved Risperidone (Risperdal) Treatment of irritability associated with autism in children 5 years of age and older Schizophrenia (13 years and older) and bipolar disorder in children (10 years and older) Off label use Quetiapine (Seroquel) Aripiprazole (Abilify) Ziprasidone (Geodon) Olanzapine (Zyprexa) Paliperidone (Invega)
 Treatment of irritability associated with autism in children 5 years of age and older. Schizophrenia (13 years and older) and bipolar disorder in children (10 years and older) Off label use. Quetiapine (Seroquel) Aripiprazole (Abilify) Ziprasidone (Geodon) Olanzapine (Zyprexa) Paliperidone (Invega)")
87
Side Effects of Anti-psychotics
Weight gain Sedation Dyspepsia Impaired glucose tolerance Dyslipidemia – elevated cholesterol Hyperprolactinemia – gynecomastia, menstrual irregularities Long-term effects to CNS in children?

88
Serious Side Effects Acute Dystonia Extrapyramidal symptoms
Spastic contraction of discrete muscle groups Most common – neck, tongue, eyes Risk factors – young, male, medication initiation or dose increase Extrapyramidal symptoms Related to dopamine blockade in nigrostriatal pathway Akathisia & parkinsonism

89
School Role with Medication
Part of treatment team Observations of student during school invaluable Dispense medication Medication or side effects may impact behavior or learning Impact on parent attitude toward medication

90
Internet Resources American Academy of Child and Adolescent Psychiatry (aacap.org) “Facts for Families” handouts on many topics Latest news on hot topics ParentsMedGuide.org Question and answer material about depression, suicide and black box warning Links for parents and physicians Up-to-date, well-organized, English-Spanish

91
Internet Resources Massachusetts General Hospital School Psychiatry Program
92
Books One Mind at a Time by Mel Levine

Similar presentations





 Miscarriage Anxiety and depression Substance.>")






 Approach.>")







