Download presentation
Presentation is loading. Please wait.

1
Ovulation Induction Dr Elsamawal El Hakim
Head Department of Obstetrics & Gynaecology Subspecialist in Reproductive Medicine Sulaiman Al Habib Hospital- Al Qassim MSc, MRCOG, MD, DRH

2
Development in Reproductive Medicine
Move toward all biosynthetic gonadotrophins Increase treatment success rates Enhance safety of stimulation regimens Simplify treatment regimens

3
What is Ovulation Induction?

4
Background Ovulation induction is mainly to patients with anovulatory infertility Hypogonadotrophic hypogonadism Polycystic ovary syndrome (PCOS) Hyperprolactinaemia
 Hyperprolactinaemia.")
5
Hypogonadotrophic hypogonadism
Amenorrhoea BUT no withdrawal bleeding after treatment with progesterone Limited production of FSH and LH from the pituitary gland

6
Gonadotrophins Gonadotrophins used for ovulation induction in women are either urinary or recombinant products. Urinary derivatives (HMG) contain 75 IU FSH and 75 IU LH per ampoule Recombinant preparations contain either FSH or LH activity Treatment of such women with recombinant FSH (rFSH) alone stimulates follicular growth, but results in inadequate estrogen production
 contain 75 IU FSH and 75 IU LH per ampoule. Recombinant preparations contain either FSH or LH activity. Treatment of such women with recombinant FSH (rFSH) alone stimulates follicular growth, but results in inadequate estrogen production.")
8
Hypo- Hypo Ovulation induction aims at the selection of a single follicle that will be able to reach the pre-ovulatory size and rupture. At the same time, estradiol (E2) levels and endometrial thickness should be appropriate. The lowest effective dose should be used Treatment is individualized and monitored by serum E2 measurements and ultrasound scans of the ovaries. The starting dose of HMG is usually 150 IU/day given for ≥5 days
 levels and endometrial thickness should be appropriate. The lowest effective dose should be used. Treatment is individualized and monitored by serum E2 measurements and ultrasound scans of the ovaries. The starting dose of HMG is usually 150 IU/day given for ≥5 days.")
9
Hypo- Hypo The criteria for the administration of HCG include serum E2 concentrations ≤2000 pmol/l with one to two follicles >16 mm in diameter by ultrasound. The ovulatory dose of HCG is 5000– IU i.m. for the urinary and 250–500 µg s.c. for the recombinant preparation. Extra HCG is administered during the luteal, which decreases the incidence of luteal phase defects and increases the pregnancy rate significantly

10
Hypo-Hypo: Pregnancy Rate
A collection of published results in 14 studies from 1966 to 1984 showed considerable variation in the percentage of patients who conceived (16–78%) Cumulative pregnancy rates of 89% after six treatment cycles and 72% after seven ovulatory cycles have been reported in two small series of hypogonadotrophic women Incidence of severe ovarian hyperstimulation syndrome (OHSS) is very low (∼1%), Multiple pregnancy rate is high (up to 30%)
 Cumulative pregnancy rates of 89% after six treatment cycles and 72% after seven ovulatory cycles have been reported in two small series of hypogonadotrophic women. Incidence of severe ovarian hyperstimulation syndrome (OHSS) is very low (∼1%), Multiple pregnancy rate is high (up to 30%)")
11
Pulsatile GnRH Idiopathic hypogonadotrophic hypogonadism and weight loss-related amenorrhoea The infusion of GnRH is performed by way of a computerized minipump at pulse intervals of between 60 and 180 min Monitoring of treatment, serum progesterone measurements could verify normal luteal phase, while ultrasound scans of the ovaries can predict the risk of multiple pregnancy

12
Pulsatile GnRH Low rate of multiple pregnancy
No evidence that HCG is required Disadvantages include the need for the pump to be connected to the body all day for a considerable number of days, the necessity to refill the pump at frequent intervals and the possible reactions of the skin

13
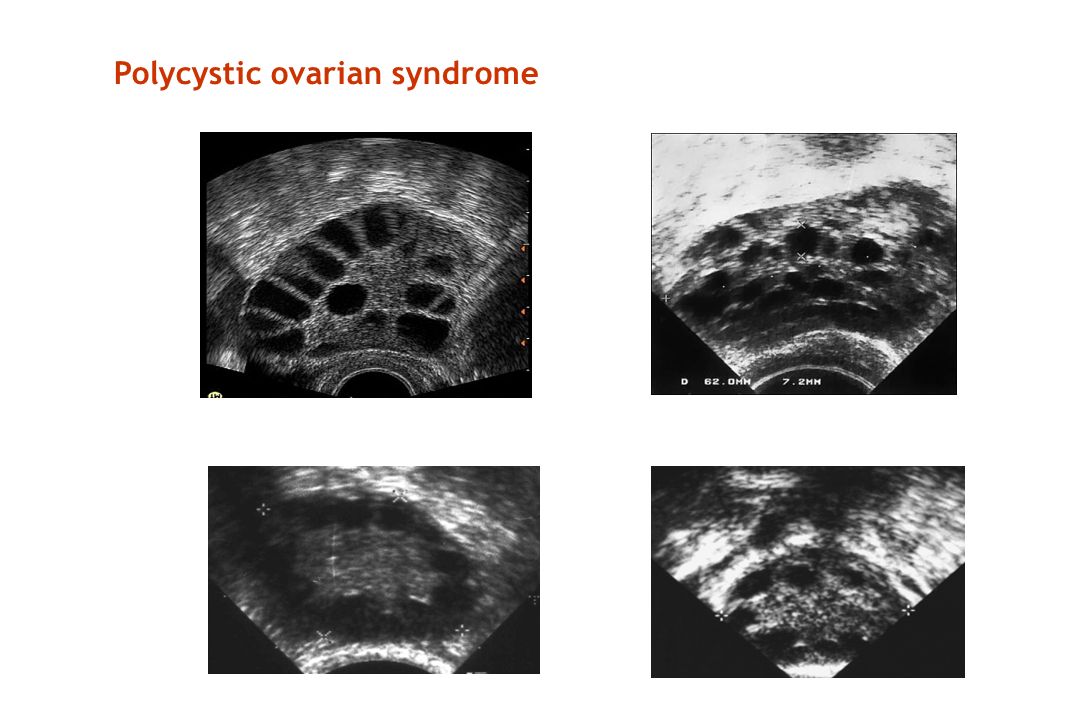
PCOS In patients with PCOS, ovulation is induced either with the use of pharmaceutical compounds, or the application of other methods, such as weight loss and exercise, or laparoscopic ovarian drilling.

14
Polycystic ovarian syndrome
14 14
16
Antiestrogens The two main antiestrogens used for ovulation induction are clomiphene citrate and tamoxifen Clomiphene, by blocking the negative feedback effect of E2, stimulates the secretion of gonadotrophins from the pituitary gland Clomiphene is given for 5 days (D2-D6) The recommended starting dose is 50 mg/day, up to a maximum dose of 150 mg/day
 The recommended starting dose is 50 mg/day, up to a maximum dose of 150 mg/day.")
17
Clomophine Citrate induces ovulation at a high rate (70–90%) and, although the pregnancy rate is lower (30–40%) Multiple pregnancy rate is ∼6–8%, mainly twins OHSS is a rare event About 10–30% of the patients will be ‘clomiphene resistant’

18
Gonadotrophins Second line treatment for ovulation induction in PCOS
‘low-dose step-up’ protocol, which involves a starting FSH dose of 75 IU/day given for 7–14 days Unless a follicle ≥12 mm is seen in the ovaries, the dose is increased by 37.5 IU/day at weekly intervals up to a maximum dose of 225 IU/day HCG is injected when the leading follicle is ≥18 mm in diameter with no more than one other follicle >14 mm

19
Gonadotrophins- Other Protocols
‘step-down’ protocol, starting dose of 150 IU/day until a follicle ≥10 mm is seen by ultrasound. The dose is then decreased by 37.5 IU/day and further to 75 IU/day 3 days later and is kept constant until the day of HCG administration Very low incidence of OHSS (1.4%) and a multiple pregnancy rate of only 5.7% with step up Modified step down, and modified step- up protocols
 and a multiple pregnancy rate of only 5.7% with step up. Modified step down, and modified step- up protocols.")
20
GnRH agonists Ovulation and pregnancy rates using the GnRH agonists in FSH-treated cycles in PCOS were encouraging, subsequent studies demonstrated an increased risk of OHSS GnRH agonists are not recommended as a treatment of choice for ovulation induction in PCOS

21
GnRH antagonists The use of GnRH antagonists in combination with gonadotrophins for ovulation induction in PCOS has until now been very successful Less incidence of OHSS

22
Gonadotropin-releasing hormone agonists versus antagonists
GnRH antagonists are more effective, safe and a well tolerated alternative to agonists for assisted reproduction cycles in PCOS patients GnRH antagonists are associated with a reduction in the incidence of OHSS in PCOS patients J Obstet Gynaecol Res Jun;36(3):605-10
:")
23
Complications of Ovulation Induction
OHSS Multiple Pregnancy

24
OHSS: Prevention Withholding hCG administration Reduced dose of hCG
Administration of native GnRH or GnRH-a Administration of rec-LH Freeze the embryos

25
Increase blood volume within 15 min
Human Albumin Administration of 50 g Half-life 14 days Luteal Phase Increase blood volume within 15 min > 800 mL

26
Ovulation Induction: Multiple Birth
Unacceptable high. Triplet and higher order is a major medical problem. Twins are also a medical problem. Can only be overcome by carefull management of O.I. and reducing number of embryos transferred.

27
Multiple Pregnancy: Complications
Maternal Fetal Miscarriages High Blood Pressure Operative delivery Haemorrage IUGR Congenital Anamolies Birth asphyxia Neonatal Death

28
Weight loss and exercise
Loss of weight in obese patients with PCOS improves substantially hyperandrogenaemia and insulin sensitivity, decreases LH concentrations and restores normal fertility Weight loss and exercise are inexpensive, they should be recommended as the first choice for the management of obese women with PCOS

29
Insulin sensitizers In the UK, the guidelines support the use of metformin in association with clomiphene in anovulatory infertility Reduce the risk of miscarriages, and gestational diabetes

30
Aromatase inhibitors Aromatase inhibitors suppress the biosynthesis of estrogen Reduce the negative feedback effect on the hypothalamic–pituitary system increased secretion of FSH that can lead to follicle selection and maturation Letrozole daily dose of 2.5 mg from days 3 to 7 of the menstrual cycle

31
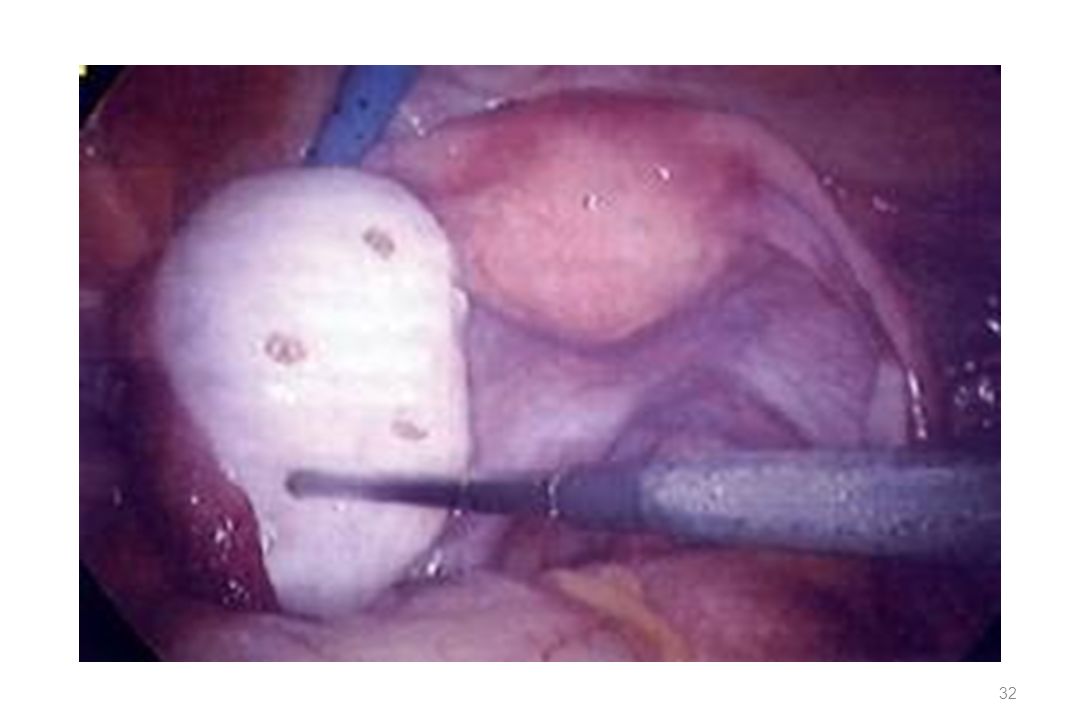
Laparoscopic ovarian drilling
Ovarian drilling is performed by using a pointed monopolar or bipolar electrode or with laser energy Restored ovulation in 92% of patients with a pregnancy rate of 69% Risks of laparoscopy and general anaesthesia, may be related to periadnexal adhesion formation in 19–43% of patients and theoretically to premature ovarian failure

33
Conclusions Many women with PCOS are anovulatory but not infertile
Most PCOS patients will conceive with minimal help if given enough time Ovulation induction Treatment is effective Age, duration of infertility are important factors to consider when offering treatment to anovulatory patients

Similar presentations
















 Is It Safe? Mustafa Uğur Zekai Tahir Burak Women’s Health Education and Research Hospital, Ankara, Turkey.>")

 is a disorder that causes menstrual and ovulation irregularities, androgen excess, and infertility.>")


 – Are We Wasting Women’s Time? Chima.>")