Download presentation
Presentation is loading. Please wait.

1
Syphilis

2
Bacteriology of Syphilis
-Spiral shaped spirochete (Treponema pallidum) -gram negative, but does not have lipopolysaccharide (LPS) -helical, thin (0.1 to 0.2 um), and long -flagella are inserted into the periplasm and give it motility -sensitive to drying, chemicals, and heat (as low as 42 degrees celsius)
 -gram negative, but does not have lipopolysaccharide (LPS) -helical, thin (0.1 to 0.2 um), and long. -flagella are inserted into the periplasm and give it motility. -sensitive to drying, chemicals, and heat (as low as 42 degrees celsius)")
3
Epidemiology of syphilis
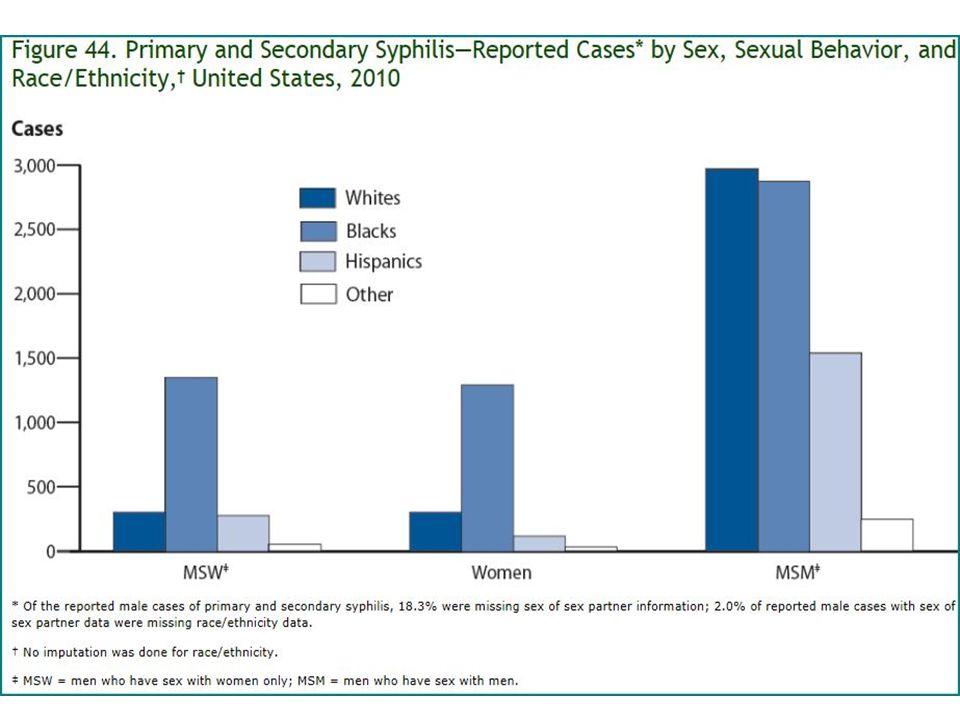
How common? 3rd most common STD 2006: > 36,000 cases of syphilis Incidence of 1° & 2° syphilis highest in women aged and men aged 35-39 2008: 63% of 1° & 2° syphilis infections involved MSM : syphilis rates increased greatest among men & women y/o

6
More on Syphilis How do we spread it? Sexual contact: vaginal, oral, or anal Spreads P-to-P via direct contact with a sore Sore locations: external genitals, vagina, anus, rectum, lips, & mouth Also, congenital infxn via transplacental transmission Usually any time >20wks gestation Spirochetes are capable of crossing placenta The culprit? Treponema pallidum

7
In case you were wondering......
NOT transmitted through contact with: Toilet seats Doorknobs Swimming pools Hot tubs or bathtubs Shared clothing Eating utensils

8
Pathogenesis of Syphilis

9
Pathogenesis of Syphilis
9 Syphilis * Spirochete – Treponema pallidum Transmission Sexual contact Trans-placental if mom has it, will spread to baby in utero (congenital syphilis) Stages of Syphilis Primary - occurs when you are first infected (via break in mucosal membrane of genital tract) - painless ulcer is presentation (2-6 weeks & then will automatically resolve) - during this time after ulcer the spirochetes will get into blood & spread to target organs (Lymph nodes, joints, muscle, skin, liver, etc) **** change slide**** Secondary - occurs 6 wks to 6 mos after initial infection - begins w/ rash (erythematous maculopapular rash) – ON PALMS & SOLES!!! – TEEMING! - malaise & flu-like illness - Great imitator b/c so many organs are affected - Even if still not treated will resolve in weeks to months then have LOOOOONG period of latency Tertiary - If left untreated then 2/3 of pts will progress to tertiary syphilis - organism has induced chronic inflammatory response in all areas that it disseminated to results in inflammatory lesions called gummas destroy soft tissue & bone (can see in arteries {vasculitis}, skin, CNS) - can result in dementia & ataxia (if in spinal cord tabes dorsalis) Pathogenesis of Syphilis
 Stages of Syphilis. Primary. - occurs when you are first infected (via break in mucosal membrane of genital tract) - painless ulcer is presentation (2-6 weeks & then will automatically resolve) - during this time after ulcer the spirochetes will get into blood & spread to target organs (Lymph nodes, joints, muscle, skin, liver, etc) **** change slide**** Secondary. - occurs 6 wks to 6 mos after initial infection. - begins w/ rash (erythematous maculopapular rash) – ON PALMS & SOLES!!! – TEEMING! - malaise & flu-like illness. - Great imitator b/c so many organs are affected. - Even if still not treated will resolve in weeks to months then have LOOOOONG period of latency. Tertiary. - If left untreated then 2/3 of pts will progress to tertiary syphilis. - organism has induced chronic inflammatory response in all areas that it disseminated to results in inflammatory lesions called gummas destroy soft tissue & bone (can see in arteries {vasculitis}, skin, CNS) - can result in dementia & ataxia (if in spinal cord tabes dorsalis) Pathogenesis of Syphilis.")
10
Virulence Factors of Syphilis
1010 Inflammatory response causes the symptoms b/c we have not found ANY toxins NO LPS, but other lipoproteins are responsible for inducing inflammatory response Outer membrane proteins allow adherence… has gram-neg cell wall stx even though does not gram stain Coats self w/ fibronectin (extracellular matrix material) to avoid being detected by phagocytes, avoid opsonization & antibodies too! Hyaluronidase to spread breaks down connective tissue Motility & corkscrew shape also help w/ spread of disease Virulence Factors of Syphilis Induces inflammatory response Adherence via membrane proteins Coats itself with fibronectin Secretes hyaluronidase Motility & corkscrew shape
 to avoid being detected by phagocytes, avoid opsonization & antibodies too! Hyaluronidase to spread breaks down connective tissue. Motility & corkscrew shape also help w/ spread of disease. Virulence Factors of Syphilis. Induces inflammatory response. Adherence via membrane proteins. Coats itself with fibronectin. Secretes hyaluronidase. Motility & corkscrew shape.")
11
Clinical Manifestations- Syphillis
Primary Syphillis presents with a PAINLESS CHANCRE!

12
Painless Chancre of Syphillis
Photo:

13
Clinical Manifestations- Syphillis
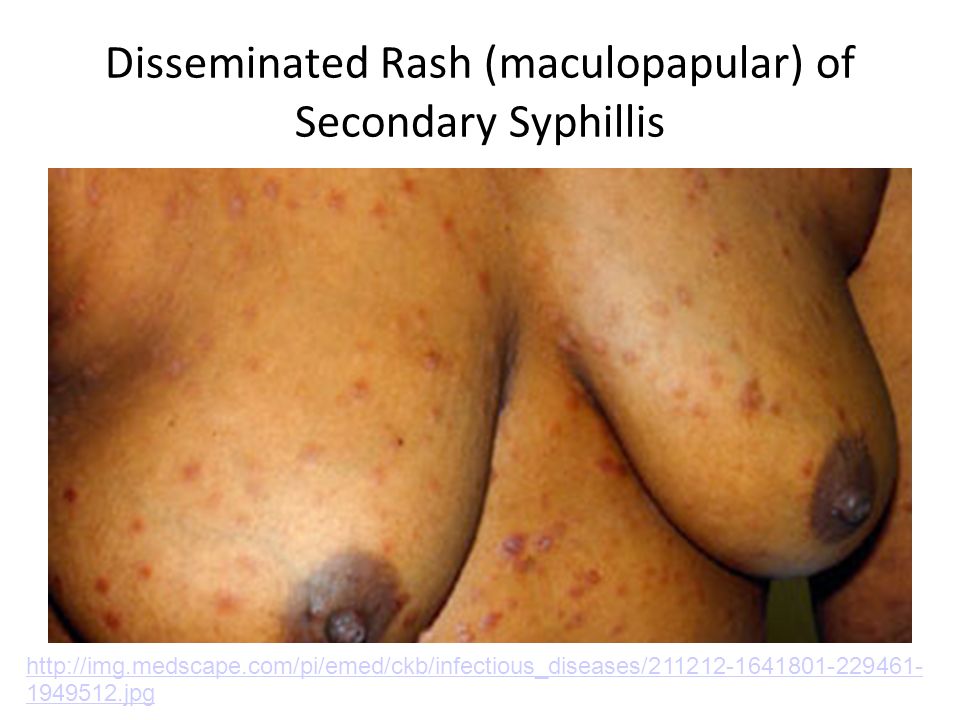
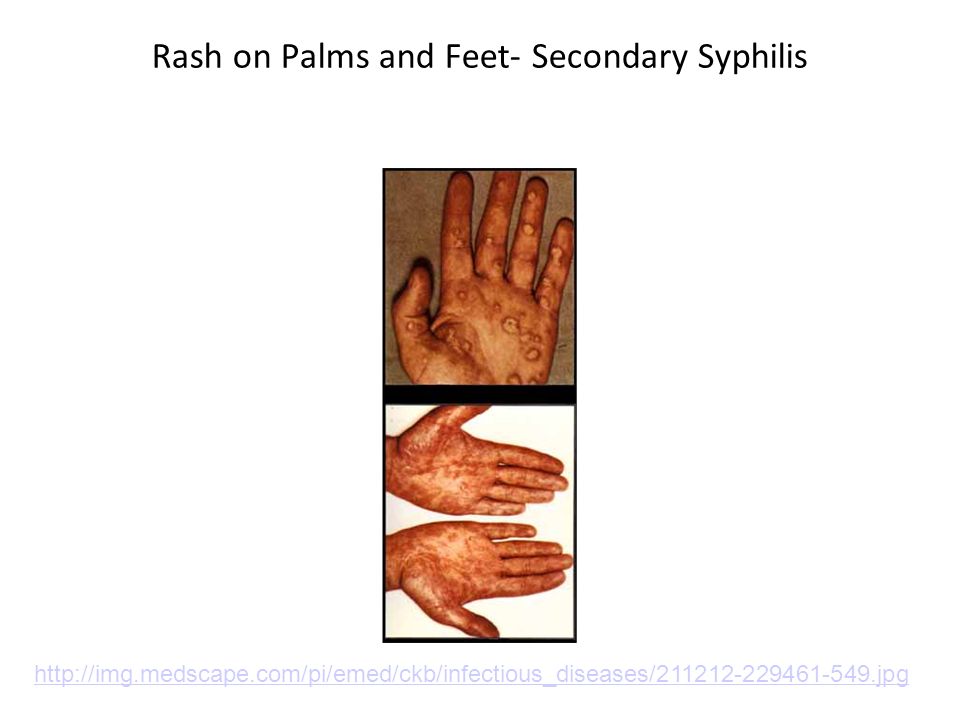
Secondary Syphilis Presents with Disseminated Disease with constitutional symptoms, maculopapular rash (that includes the PALMS and SOLES), condylomata lata. Many treponemes are present in the condylomata lata of Secondary Syphilis (Treponemes and may be visualized through DARKFIELD MICROSCOPY. “Teeming with spirochetes!” Remember: “Secondary Syphillis = Systemic” Question: What other Disease presents with rash that includes the hands and feet? Answer: RMSF caused by R. rickettsii
, condylomata lata. Many treponemes are present in the condylomata lata of Secondary Syphilis (Treponemes and may be visualized through DARKFIELD MICROSCOPY. Teeming with spirochetes! Remember: Secondary Syphillis = Systemic Question: What other Disease presents with rash that includes the hands and feet Answer: RMSF caused by R. rickettsii.")
14
Secondary Syphillis- Disseminated Disease

15
Disseminated Rash (maculopapular) of Secondary Syphillis
16
Rash on Palms and Feet- Secondary Syphilis
17
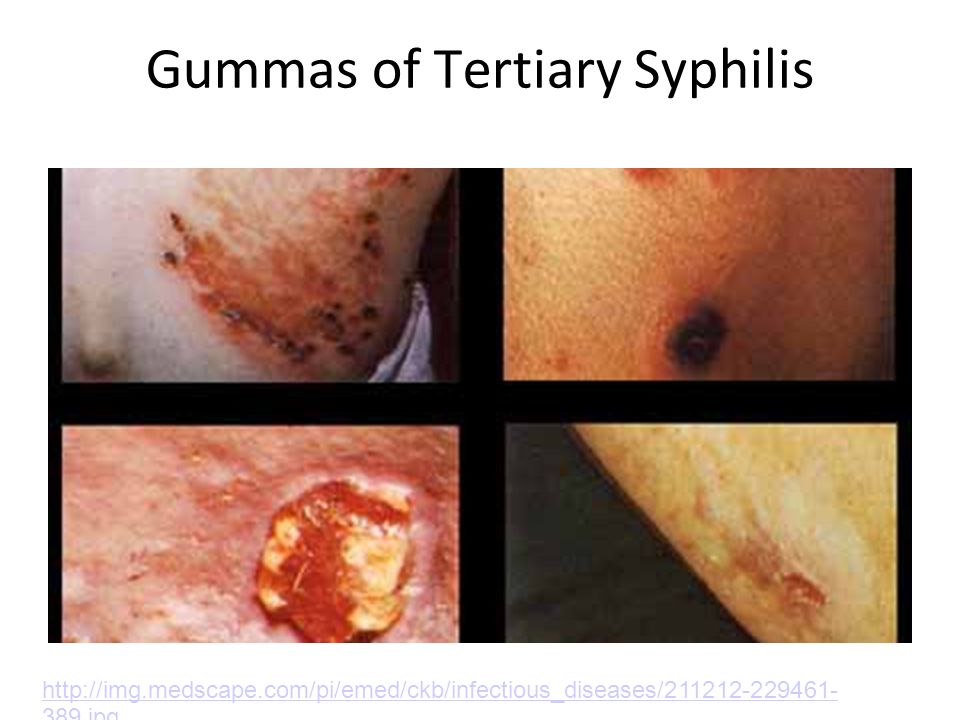
Tertiary Syphillis Gummas (chronic granulomas), aortitis (vasa vasorum destruction), neurosyphilis (tabes dorsalis), Argyll Robertson pupil. NEUROSYPHILLIS has many manifestations Signs: broad-based ataxia, positive Romberg, Charcot joint, stroke without hypertension.

18
Gummas of Tertiary Syphilis
19
Argyll Robertson Pupil- Associated with Tertiary Syphilis.
Argyll Robertson is the pupil that constricts with accommodation, but is not reactive to light. aka “Prostitute’s pupil- it accommodates but does not react.” Pupils accommodate to close objects by constricting, but do not constrict when exposed to light.

20
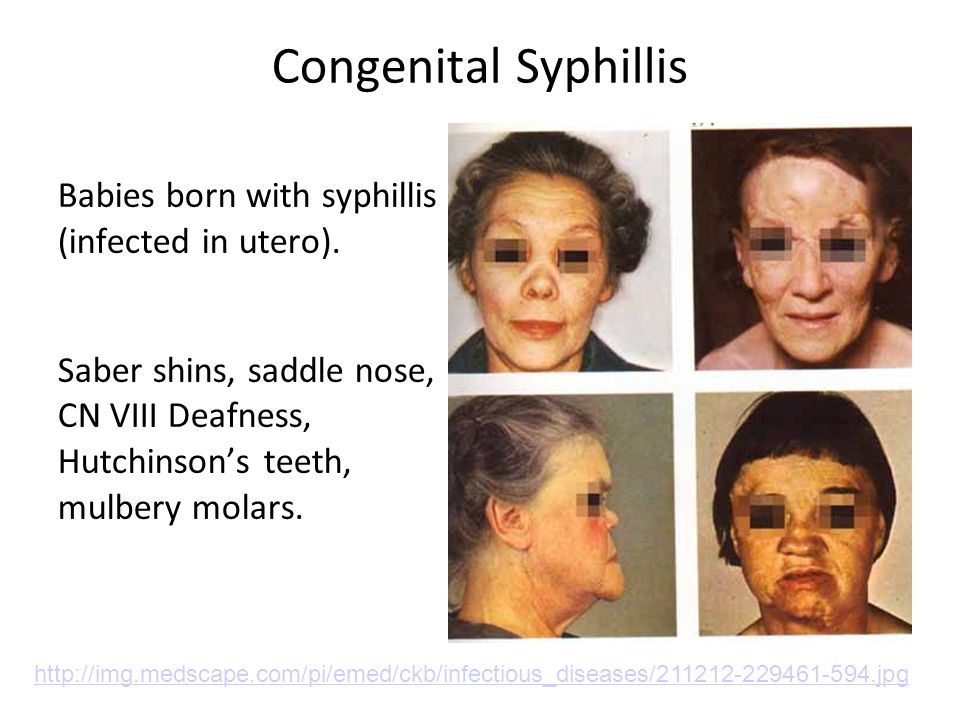
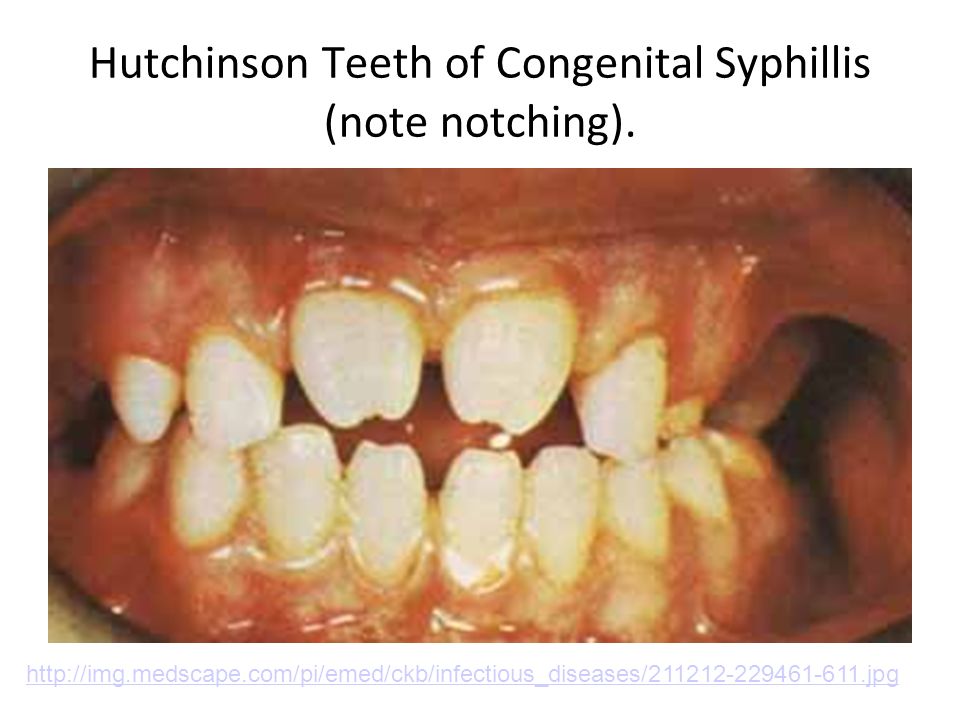
Congenital Syphillis Babies born with syphillis (infected in utero). Saber shins, saddle nose, CN VIII Deafness, Hutchinson’s teeth, mulbery molars.
21
Hutchinson Teeth of Congenital Syphillis (note notching).
22
Diagnosis Will not grow in culture
Microscopy of exudates to look for organisms Darkfield Direct fluorescent antibody staining

23
Diagnosis Serology To detect antibodies to cardiolipin (nonspecific)
VDRL- (Venereal Disease Research Laboratory Test) RPR- (Rapid Plasma Reagin) Test Then test for treponemal antibodies FTA-ABS (fluorescent treponemal antibody absorption) MHA-TP- (microhemagglutination assay for treponema)
 RPR- (Rapid Plasma Reagin) Test. Then test for treponemal antibodies. FTA-ABS (fluorescent treponemal antibody absorption) MHA-TP- (microhemagglutination assay for treponema)")
24
Treatment DOC is Penicillin G Can also use Ceftriaxone
If allergic to penicillin, can use Erythromycin or Doxycycline Follow up at 3, 6, and 12 months with VDRL or RPR

25
Chlamydia

26
Bacteriology of Chlamydia
-Obligate intracellular gram-negative bacteria -pleomorphic and non-motile -small in size (0.25 to 0.8 um in diameter), and have small chromosomes (1 – 1.2 megabases) -”Energy Parasites”: Auxotropic for amino acids, and use host cell’s ATP -Cell wall is unusual in that it lacks muramic acid -Cannot be cultured in nutrient broth media or on agar plates
, and have small chromosomes (1 – 1.2 megabases) - Energy Parasites : Auxotropic for amino acids, and use host cell’s ATP. -Cell wall is unusual in that it lacks muramic acid. -Cannot be cultured in nutrient broth media or on agar plates.")
27
Epidemiology of Chlamydia
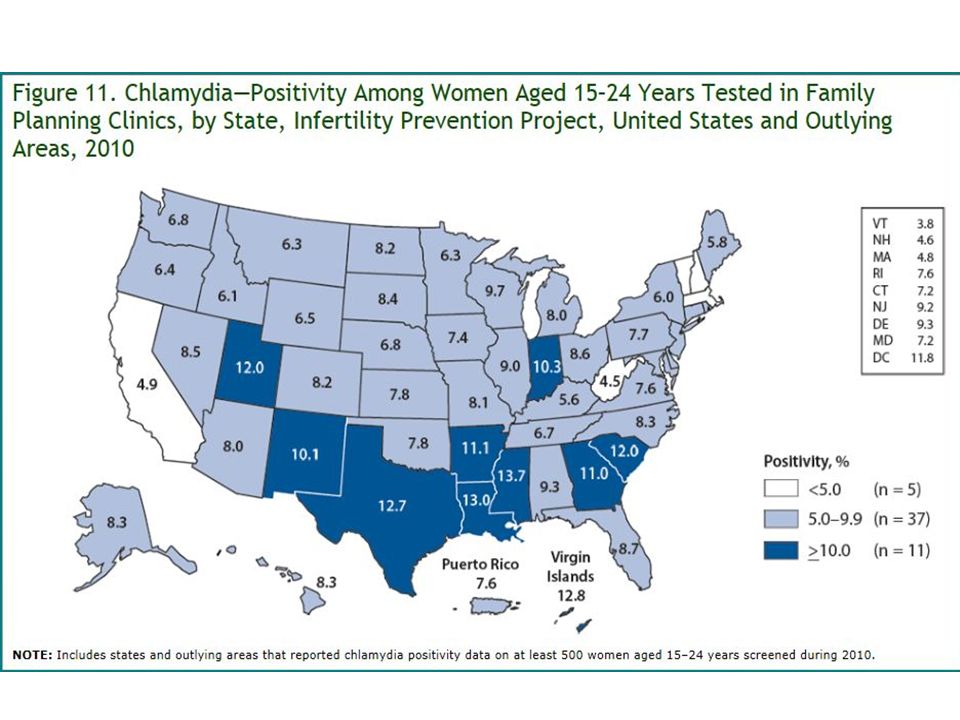
How common? #1 reported STD in U.S. Highest infxn rates in Native & African Americans 2010: 1,307,893 reported infxns from 50 states Many unreported cases d/t lack of sxs in many individuals An estimated 2.8 million infxns occur in U.S. per year Worldwide, an estimated 90 million new cases each year Esp high infxn risk for sexually active teen girls d/t immaturity of cervix being more susceptible to infxn

28
Epidemiology Cont'd How do I get it? Vaginal, oral, or anal sex
Also transmitted during childbirth More sexual partners = higher risk Urethra = most common site for infxn in both men & women Chlamydia trachomatis = MCC of acute urethral syndrome in women & MCC of nonspecific urethritis (NSU) in men The leading preventable cause of infertility worldwide N. gonorrhoeae coexists in 45% of cases
 in men. The leading preventable cause of infertility worldwide. N. gonorrhoeae coexists in 45% of cases.")
31
Do NOT gram stain & do not grow on agar or liquid media
Obligate intracellular bacteria b/c they require host cell ATP to replicate Do NOT gram stain & do not grow on agar or liquid media Similar in stx to gram neg even though they don’t gram stain (have outer membrane & LPS) Life Cycle Consists of 2 forms: Elementary bodies metabolically IN-active form… infectious! These are released from infected cell to infect new cell Reticulate bodies metabolically ACTIVE… NOT infectious Develop from EB and grow inside cell after hrs they change back to EB & infect new cell Process of Infection EB attaches & enters cell via endocytosis in vesicle RB form from EB & continue to replicate via binary fission RBs tranform back to EB once done replicating & evetually cell will lyse releasing EBs which are able to infect a new cell & start the process over again **** change slide**** NOTE: In presence of IFN-gamma from Th1 cells (cell-mediated immunity) chlamydia will “shut down” growth (PERSISTENT STATE) causing immune system to think infection is gone once IFN-gamma decreases then chlamydia will resume replication & growth leading to chronic infection 3131
 Life Cycle. Consists of 2 forms: Elementary bodies metabolically IN-active form… infectious! These are released from infected cell to infect new cell. Reticulate bodies metabolically ACTIVE… NOT infectious. Develop from EB and grow inside cell after hrs they change back to EB & infect new cell. Process of Infection. EB attaches & enters cell via endocytosis in vesicle. RB form from EB & continue to replicate via binary fission. RBs tranform back to EB once done replicating & evetually cell will lyse releasing EBs which are able to infect a new cell & start the process over again. **** change slide**** NOTE: In presence of IFN-gamma from Th1 cells (cell-mediated immunity) chlamydia will shut down growth (PERSISTENT STATE) causing immune system to think infection is gone once IFN-gamma decreases then chlamydia will resume replication & growth leading to chronic infection")
32
Pathogenesis of Chlamydia
3232 Obligate intracellular bacteria b/c they require host cell ATP to replicate Do NOT gram stain & do not grow on agar or liquid media Similar in stx to gram neg even though they don’t gram stain (have outer membrane & LPS) Life Cycle Consists of 2 forms: Elementary bodies metabolically IN-active form… infectious! These are released from infected cell to infect new cell Reticulate bodies metabolically ACTIVE… NOT infectious Develop from EB and grow inside cell after hrs they change back to EB & infect new cell Process of Infection EB attaches & enters cell via endocytosis in vesicle RB form from EB & continue to replicate via binary fission RBs tranform back to EB once done replicating & evetually cell will lyse releasing EBs which are able to infect a new cell & start the process over again NOTE: In presence of IFN-gamma from Th1 cells (cell-mediated immunity) chlamydia will “shut down” growth (PERSISTENT STATE) causing immune system to think infection is gone once IFN-gamma decreases then chlamydia will resume replication & growth leading to chronic infection (continual inflammation can cause tissue remodeling & scarring) IFN-gamma upregulates enzyme that degrades tryptophan… tryptophan is required for chlamydia (needs it from host cell) since chalmydia doesn’t have it, it will pause it’s growth Pathogenesis of Chlamydia
 Life Cycle. Consists of 2 forms: Elementary bodies metabolically IN-active form… infectious! These are released from infected cell to infect new cell. Reticulate bodies metabolically ACTIVE… NOT infectious. Develop from EB and grow inside cell after hrs they change back to EB & infect new cell. Process of Infection. EB attaches & enters cell via endocytosis in vesicle. RB form from EB & continue to replicate via binary fission. RBs tranform back to EB once done replicating & evetually cell will lyse releasing EBs which are able to infect a new cell & start the process over again. NOTE: In presence of IFN-gamma from Th1 cells (cell-mediated immunity) chlamydia will shut down growth (PERSISTENT STATE) causing immune system to think infection is gone once IFN-gamma decreases then chlamydia will resume replication & growth leading to chronic infection (continual inflammation can cause tissue remodeling & scarring) IFN-gamma upregulates enzyme that degrades tryptophan… tryptophan is required for chlamydia (needs it from host cell) since chalmydia doesn’t have it, it will pause it’s growth. Pathogenesis of Chlamydia.")
33
Virulence Factors of Chlamydia
3333 Intracellular organism Able to avoid antibodies & NTs etc (hides in the cell)… but it is suceptible to cytotoxic T cells or NK cells (to stop this it is able to downregulate MHC class I expression decreases ability of cytotoxic T cells to kill it (decreased antigen presentation to CD8 cells), but likely increases NK ability (NK cells kill cells that are missing the “self-marker” MHC-I molecules) LPS VERY Inflammatory NTs can’t do anything b/c intracellular (cervicitis & urethritis) Secretion of IL-1 (increase NTs & lymphocytes & cause fever) & IL-8 (inflammatory mediator) Prevents fusion of endosome w/ lysosome (allows for safe haven for replication of RBs) Nutrient up-take Needs ATP & nutrients to get into endosome Inserts molecules into endosome that allow for transport of nutrients & ATP into endosome for bacteria use Type 3 secretion system molecular “syringe” put together by chlamydia that sticks thru endosome membrane, it’s able to inject things back INTO cytosol… likely something that inhibits apoptosis to allow growth of RBs & creation of more EBs to infect more cells Virulence Factors of Chlamydia Intracellular organism Downregulates MHC-I LPS Prevent fusion of endosome with lysosome Able to go into a persistent state Nutrient up-take Type 3 secretion system
… but it is suceptible to cytotoxic T cells or NK cells (to stop this it is able to downregulate MHC class I expression decreases ability of cytotoxic T cells to kill it (decreased antigen presentation to CD8 cells), but likely increases NK ability (NK cells kill cells that are missing the self-marker MHC-I molecules) LPS. VERY Inflammatory NTs can’t do anything b/c intracellular (cervicitis & urethritis) Secretion of IL-1 (increase NTs & lymphocytes & cause fever) & IL-8 (inflammatory mediator) Prevents fusion of endosome w/ lysosome (allows for safe haven for replication of RBs) Nutrient up-take. Needs ATP & nutrients to get into endosome. Inserts molecules into endosome that allow for transport of nutrients & ATP into endosome for bacteria use. Type 3 secretion system molecular syringe put together by chlamydia that sticks thru endosome membrane, it’s able to inject things back INTO cytosol… likely something that inhibits apoptosis to allow growth of RBs & creation of more EBs to infect more cells. Virulence Factors of Chlamydia. Intracellular organism. Downregulates MHC-I. LPS. Prevent fusion of endosome with lysosome. Able to go into a persistent state. Nutrient up-take. Type 3 secretion system.")
34
Chlamydia manifestations
Chalamydia trachomatis causes reactive arthritis, conjunctivitis, nongonoccocal urethritis, and pelvic inflammatory disease (PID).
.")
35
Chlamydia in men Urethritis Painful urination Burning sensation upon urination Discharge from penis Red, inflamed urethra Chlamydia is picked up easier in men because it is more noticeable.

36
Chlamydia manifestations in Women
&

37
Diagnosis and Treatment
Doesn’t gram stain well but can gram stain urethral discharge to rule out gonorrhea Fluorescent stained smear Positive leukocyte esterase test on first-void urine NAAT Treatment- Azithromycin (single dose) or Doxycycline (costs less, twice daily for 1 week)
 or Doxycycline (costs less, twice daily for 1 week)")
38
Neisseria Gonorrhea

39
Bacteriology for N. Gonorrhea
-a facultative intracellular gram-negative diplococci, -humans are the only reservoir -Ferment glucose, but do not ferment maltose -No polysaccharide capsule -produce IgA proteases

40
Epidemiology of Gonorrhea
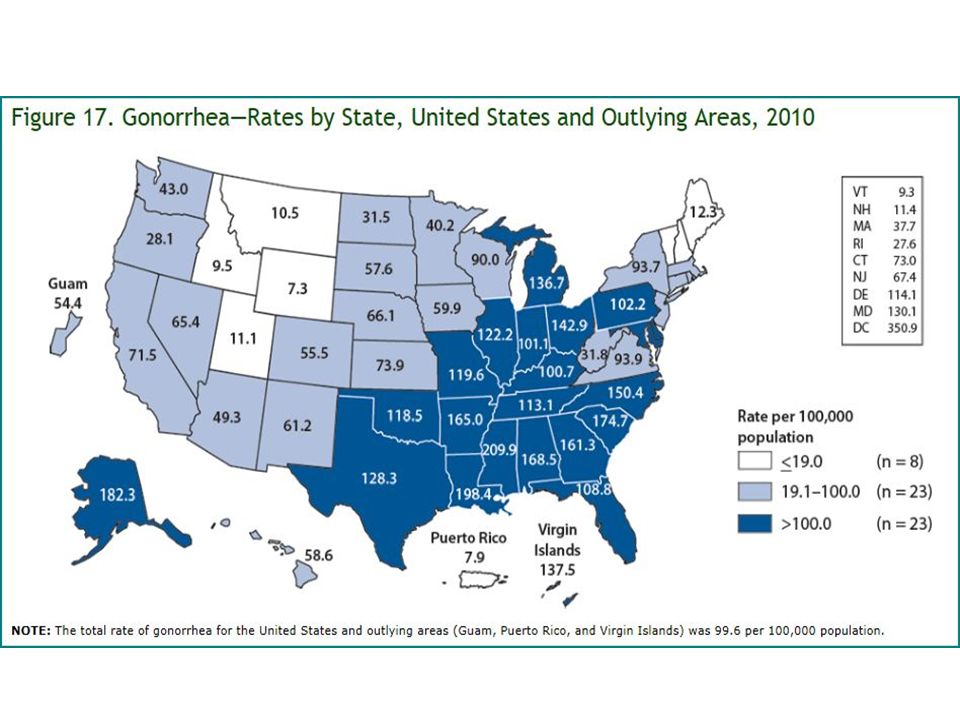
How common? 2nd most common venereal disease 2009: 301,174 reported cases However, in U.S., it's estimated that >700,000 new infxns occur each year Highest rates in sexually active teens, young adults, MSM, Hispanics & AAs Worldwide, an estimated 62 million new cases each year W/highest rates in sub-Saharan Africa, southeast Asia, the Caribbean, & Latin America

41
More Gonorrhea Epidemiology
How are we spreading it? Contact w/infected penis, vagina, mouth, or anus Pregnant female can transmit infxn to baby during delivery as well Bacteria multiplies easily in warm, moist areas Urethra = MC site for gonococcal infxn in both men & women N. gonorrhoeae = MCC of septic arthritis in urban populations Can lead to disseminated gonococcemia More common in young women d/t C6-C9 deficiency

44
Pathogenesis of N. Gonorrhea
4444 Sexual contact = exposure to bacteria (gram negative diplococci) N. Gonorrhea adheres to columnar epithelial cells of genital tract via pili & opa proteins (these also play a role in getting the bacteria nutrients), opa specifically helps facilitate mvmt across the cell epithelial cell will endocytose bacteria (bacteria itself induces this to get to replication location) & transport them across the cell where they are then exocytosed and replicate on the basement membrane outside of the cell replication causes activation of acute inflammatory response When they are taken up by macrophage, porin prevents the fusion of lysosome w/ phagosome thereby allowing survival of bacteria…. Now that its living in macrophages it causes release of TNF… TNF causes damage to epithelial cells & you see invasion of neutrophils (lots of pus). Also LOS induces release of proteases & phospholipases killing of mucosal cells discharge N. Gonorrhea can survive inside of the phagolysosome (NT) no capsule but surface does repel NTs to an extent May also get into blood & disseminate to cause problems elsewhere in the body (joints, skin, meninges, etc) **** change slide **** Virulence factors = Pili Opa proteins Antigen variation (this is mutation of antigens expressed on cell surface)/antigen phase variation (coordinated change in gene expression which changes expression of proteins on surface) this is why we are subject to recurrent infections Porins – take up nutrients, this is also how antibiotics are taken up may see mutation of porins & antibiotic resistance LOS – endotoxin Can secrete IgA protease to breakdown any IgA that we are trying to make to prevent repeat infection Pathogenesis of N. Gonorrhea
 N. Gonorrhea adheres to columnar epithelial cells of genital tract via pili & opa proteins (these also play a role in getting the bacteria nutrients), opa specifically helps facilitate mvmt across the cell epithelial cell will endocytose bacteria (bacteria itself induces this to get to replication location) & transport them across the cell where they are then exocytosed and replicate on the basement membrane outside of the cell replication causes activation of acute inflammatory response When they are taken up by macrophage, porin prevents the fusion of lysosome w/ phagosome thereby allowing survival of bacteria…. Now that its living in macrophages it causes release of TNF… TNF causes damage to epithelial cells & you see invasion of neutrophils (lots of pus). Also LOS induces release of proteases & phospholipases killing of mucosal cells discharge. N. Gonorrhea can survive inside of the phagolysosome (NT) no capsule but surface does repel NTs to an extent. May also get into blood & disseminate to cause problems elsewhere in the body (joints, skin, meninges, etc) **** change slide **** Virulence factors = Pili. Opa proteins. Antigen variation (this is mutation of antigens expressed on cell surface)/antigen phase variation (coordinated change in gene expression which changes expression of proteins on surface) this is why we are subject to recurrent infections. Porins – take up nutrients, this is also how antibiotics are taken up may see mutation of porins & antibiotic resistance. LOS – endotoxin. Can secrete IgA protease to breakdown any IgA that we are trying to make to prevent repeat infection. Pathogenesis of N. Gonorrhea.")
45
Virulence Factors of N. Gonorrhea
4545 Virulence factors = Pili Opa proteins Antigen variation (this is mutation of antigens expressed on cell surface)/antigen phase variation (coordinated change in gene expression which changes expression of proteins on surface) this is why we are subject to recurrent infections Porins – take up nutrients, this is also how antibiotics are taken up may see mutation of porins & antibiotic resistance LOS – endotoxin Can secrete IgA protease to breakdown any IgA that we are trying to make to prevent repeat infection Antibiotic Resistance Mutated Penicillin binding ptn Also seen w/ strep pneumo & MRSA Normally function via penicillin/B-lactam antibiotics binding to PBP & preventing construction of bacterial cell wall… but w/ mutation B-lactams cannot bind as effectively B-lactamases Lysis of B-lactam ring structure in penicillin antibiotics (& others w/ B-lactam ring stx Sulbactam & tazobactam are B-lactamase inhibitors Efflux pumps Ptn pump in membrane of bacteria that pumps antibiotics back out once they enter Mutation in DNA replicating enzymes (DNA gyrase and topoisomerase) Resistance to fluoroquinolones MOA of fluoros is to bind to DNA gyrase/topoisomerase & prevent replication but w/ mutation they can’t do their job Mutation of porins Antibiotic cannot penetrate into bacteria Virulence Factors of N. Gonorrhea Pili Opa proteins Antigen variation/antigen phase variation Porins LOS IgA protease
/antigen phase variation (coordinated change in gene expression which changes expression of proteins on surface) this is why we are subject to recurrent infections. Porins – take up nutrients, this is also how antibiotics are taken up may see mutation of porins & antibiotic resistance. LOS – endotoxin. Can secrete IgA protease to breakdown any IgA that we are trying to make to prevent repeat infection. Antibiotic Resistance. Mutated Penicillin binding ptn. Also seen w/ strep pneumo & MRSA. Normally function via penicillin/B-lactam antibiotics binding to PBP & preventing construction of bacterial cell wall… but w/ mutation B-lactams cannot bind as effectively. B-lactamases. Lysis of B-lactam ring structure in penicillin antibiotics (& others w/ B-lactam ring stx. Sulbactam & tazobactam are B-lactamase inhibitors. Efflux pumps. Ptn pump in membrane of bacteria that pumps antibiotics back out once they enter. Mutation in DNA replicating enzymes (DNA gyrase and topoisomerase) Resistance to fluoroquinolones. MOA of fluoros is to bind to DNA gyrase/topoisomerase & prevent replication but w/ mutation they can’t do their job. Mutation of porins. Antibiotic cannot penetrate into bacteria. Virulence Factors of N. Gonorrhea. Pili. Opa proteins. Antigen variation/antigen phase variation. Porins. LOS. IgA protease.")
46
Clinical Manifestations- N. gonorrhoeae
Causes The STD Gonorrhea aka “The Clap” Septic Arthritis Neonatal Conjunctivitis PID Fitz-Hugh-Curtis Syndrome

47
Gonorrhea Clinical Manifestations
Burning and pain while urinating Increased urinary frequency or urgency Discharge from the penis (white, yellow, or green in color) Red or swollen opening of penis (urethra) Tender or swollen testicles Sore throat (gonococcal pharyngitis)
 Red or swollen opening of penis (urethra) Tender or swollen testicles Sore throat (gonococcal pharyngitis)")
48
Gonorrhea Clinical Manifestations

49
Fitz-Hugh-Curtis Syndrome
Fitz-Hugh-Curtis Syndrome is a complication of Pelvic Inflammatory Disease and can occur due to both Chlamydia and Gonorrhea Note “Violin-String” appearance of chronic adhesions/fibrosis

50
Diagnosis Nucleic acid amplification test (NAAT)- most sensitive
Culture on Thayer-Martin agar or chocolate agar Gram stain male urethral specimens-shows intracellular gram negative diplococci

51
Treatment Current Recommendations:
Ceftriaxone or Cefixime PLUS Azithromycin or Doxycycline (for chlamydia infection) Penicillin was the DOC but resistance to it and fluoroquinolones is growing Mutation of fluoroquinolone binding sites on bacterial DNA gyrase and topoisomerase Increased activity of efflux pumps or decreased membrane permeability
 Penicillin was the DOC but resistance to it and fluoroquinolones is growing. Mutation of fluoroquinolone binding sites on bacterial DNA gyrase and topoisomerase. Increased activity of efflux pumps or decreased membrane permeability.")
52
Review Questions

53
Q1: A 32y/o businessman comes into your office
Q1: A 32y/o businessman comes into your office. He was well until yesterday, when he admits he experienced dysuria accompanied by yellowish urethral discharge. He also admits that he had intercourse with a prostitute 5 nights ago. You perform a gram stain on a specimen of the discharge and see gram-negative diplococci within neutrophils. Given this characteristic finding, you know right away that the most likely cause of this infection is? A: Neisseria gonorrhoeae B. Proteus mirabilis C. Klebsiella pneumoniae D. Chlamydia trachomatis E. Treponema pallidum

54
Question 1 Explanation Answer: (A). Neisseriae are gram-negative, oxidase-positive cocci that resemble paired kidney beans. N. gonorrhoeae causes gonorrhea, neonatal conjunctivitis, & PID. Gonorrhea in men is characterized primarily by urethritis accompanied by dysuria and a purulent discharge. In women, infection is located primarily in the endocervix, causing a purulent vaginal discharge and intermenstrual bleeding (cervicitis). The most common complication in women is ascending infection into the uterine tubes, causing salpingitis/PID, which can result in sterility or ectopic pregnancy. Disseminated infections commonly manifest as arthritis, tenosynovitis, or pustules. In men, the finding of gram-negative diplococci within PMNs is sufficient for diagnosis. In women, the use of gram stain alone can be difficult to interpret, so cultures should be done additionally. T. pallidum is a spirochete, which is a thin-walled, flexible, spiral-shaped, motile rod. They are so thin that they are seen only by darkfield microscopy, silver impregnation, or immunofluorescence. Chlamydiae are obligate intracellular bacteria, and thus, the gram stain is not useful. In men, C. trachomatis is a common cause of NGU, which may progress to epididymitis, prostatitis, or proctitis. In women, cervicitis develops and may progress to PID or salpingitis. Source: Ex Master USMLE -style Question Bank
. Neisseriae are gram-negative, oxidase-positive cocci that resemble paired kidney beans. N. gonorrhoeae causes gonorrhea, neonatal conjunctivitis, & PID. Gonorrhea in men is characterized primarily by urethritis accompanied by dysuria and a purulent discharge. In women, infection is located primarily in the endocervix, causing a purulent vaginal discharge and intermenstrual bleeding (cervicitis). The most common complication in women is ascending infection into the uterine tubes, causing salpingitis/PID, which can result in sterility or ectopic pregnancy. Disseminated infections commonly manifest as arthritis, tenosynovitis, or pustules. In men, the finding of gram-negative diplococci within PMNs is sufficient for diagnosis. In women, the use of gram stain alone can be difficult to interpret, so cultures should be done additionally. T. pallidum is a spirochete, which is a thin-walled, flexible, spiral-shaped, motile rod. They are so thin that they are seen only by darkfield microscopy, silver impregnation, or immunofluorescence. Chlamydiae are obligate intracellular bacteria, and thus, the gram stain is not useful. In men, C. trachomatis is a common cause of NGU, which may progress to epididymitis, prostatitis, or proctitis. In women, cervicitis develops and may progress to PID or salpingitis. Source: Ex Master USMLE -style Question Bank.")
55
Q2: A 30-year-old, sexually active woman has had a mucopurulent vaginal discharge for 1 week. On pelvic examination, the cervix appears reddened around the os, but no erosions or mass lesions are present. A Pap smear shows numerous neutrophils, but no dysplastic cells. A cervical biopsy specimen shows marked follicular cervicitis. Which of the following infectious agents is most likely to produce these findings? A. Chlamydia trachomatis B. Candida albicans C. Gardnerella vaginalis D. HPV E. Neisseria gonorrhoeae F. Trichomonas vaginalis

56
Question 2 Explanation Answer: (A) The redness of the cervix, the inflammatory cells in the cervical discharge, and the biopsy findings indicate that the patient has cervicitis. Chlamydia trachomatis is the most common cause of cervicitis in sexually active women. Candidiasis, gonorrhea, and trichomoniasis also are common. Candidiasis often produces a scant, white, curdlike vaginal discharge; gonorrhea may have an associated urethritis; and Trichomonas may produce a profuse homogeneous, frothy, and adherent yellow or green vaginal discharge. Gardnerella is found in bacterial vaginosis, a common condition caused by overgrowth of bacteria. Gardnerella infection produces a moderate, homogeneous, low- viscosity, adherent vaginal discharge that is white or gray and has a characteristic “fishy” odor; “clue” cells are seen on a wet mount. Herpetic infections are more likely to manifest as clear vesicles on the skin in the perineal region. Infection with human papillomavirus is associated with condylomata, dysplasias, and carcinoma. Source: Robbins & Cotran Review of Pathology, 3rd ed, Ch.22- The Female Genital Tract
 The redness of the cervix, the inflammatory cells in the cervical discharge, and the biopsy findings indicate that the patient has cervicitis. Chlamydia trachomatis is the most common cause of cervicitis in sexually active women. Candidiasis, gonorrhea, and trichomoniasis also are common. Candidiasis often produces a scant, white, curdlike vaginal discharge; gonorrhea may have an associated urethritis; and Trichomonas may produce a profuse homogeneous, frothy, and adherent yellow or green vaginal discharge. Gardnerella is found in bacterial vaginosis, a common condition caused by overgrowth of bacteria. Gardnerella infection produces a moderate, homogeneous, low- viscosity, adherent vaginal discharge that is white or gray and has a characteristic fishy odor; clue cells are seen on a wet mount. Herpetic infections are more likely to manifest as clear vesicles on the skin in the perineal region. Infection with human papillomavirus is associated with condylomata, dysplasias, and carcinoma. Source: Robbins & Cotran Review of Pathology, 3rd ed, Ch.22- The Female Genital Tract.")
57
Q3: A 73-year-old man who has had progressive dementia for the past 6 years dies of bronchopneumonia. Autopsy shows that the thoracic aorta has a dilated root and arch, giving the intimal surface a “tree-bark” appearance. Microscopic examination of the aorta shows an obliterative endarteritis of the vasa vasorum. Which of the following laboratory findings is most likely to be recorded in this patient's medical history? A. High double-stranded DNA titer B. P-ANCA positive 1:1024 C. Sedimentation rate 105 mm/hr D. Ketonuria 4+ E. Antibodies against Treponema pallidum

58
Question 3 Explanation Answer: (E) This description is most suggestive of syphilitic aortitis, a complication of tertiary syphilis, with characteristic involvement of the thoracic aorta. Obliterative endarteritis is not a feature of other forms of vasculitis. High-titer doublestranded DNA antibodies are diagnostic of systemic lupus erythematosus, and a test result for P-ANCA is positive in various vasculitides, including microscopic polyangiitis. A high sedimentation rate is a nonspecific marker of inflammatory diseases. Ketonuria can occur in individuals with diabetic ketoacidosis. Source: Robbins & Cotran Review of Pathology, 3rd ed, Ch.11-Blood Vessels
 This description is most suggestive of syphilitic aortitis, a complication of tertiary syphilis, with characteristic involvement of the thoracic aorta. Obliterative endarteritis is not a feature of other forms of vasculitis. High-titer doublestranded DNA antibodies are diagnostic of systemic lupus erythematosus, and a test result for P-ANCA is positive in various vasculitides, including microscopic polyangiitis. A high sedimentation rate is a nonspecific marker of inflammatory diseases. Ketonuria can occur in individuals with diabetic ketoacidosis. Source: Robbins & Cotran Review of Pathology, 3rd ed, Ch.11-Blood Vessels.")
59
Q4: A sexually active, 26-year-old man has had pain on urination for the past 4 days. On physical examination, there are no lesions on the penis. He is afebrile. Urinalysis shows no blood, ketones, protein, or glucose. Microscopic examination of the urine shows few WBCs and no casts or crystals. What infectious agent is most likely to produce these findings? A. Chlamydia trachomatis B. Mycobacterium tuberculosis C. Herpes simplex virus D. Candida albicans E. Treponema pallidum

60
Question 4 Explanation Answer: (A) This patient has urethritis. The most common cause of nongonococcal urethritis in men is Chlamydia trachomatis. The condition is a nuisance; however, the behavior that led to the infection can place the patient at risk of other sexually transmitted diseases. Tuberculosis of the urinary tract is uncommon. Herpes simplex can produce painful vesicles on the skin. Candida infections typically occur in immunocompromised patients or in patients receiving long-term antibiotic therapy. A syphilitic chancre on the penis is an indicator of Treponema pallidum infection. Source: Robbins & Cotran Review of Pathology, 3rd ed, Ch.20- The Kidney
 This patient has urethritis. The most common cause of nongonococcal urethritis in men is Chlamydia trachomatis. The condition is a nuisance; however, the behavior that led to the infection can place the patient at risk of other sexually transmitted diseases. Tuberculosis of the urinary tract is uncommon. Herpes simplex can produce painful vesicles on the skin. Candida infections typically occur in immunocompromised patients or in patients receiving long-term antibiotic therapy. A syphilitic chancre on the penis is an indicator of Treponema pallidum infection. Source: Robbins & Cotran Review of Pathology, 3rd ed, Ch.20- The Kidney.")
61
Q5: A 20-year-old man who has multiple sexual partners and does not use barrier precautions comes to the physician complaining of a nontender ulcer on the penis that has been present for 1 week. On physical examination, the 0.6-cm lesion has a firm, erythematous base and sharply demarcated borders. The lesion is scraped, and darkfield examination is positive for spirochetes consistent with Treponema pallidum. Which of the following is most likely to be seen microscopically in the biopsy specimen? A. Granulomatous inflammation with suppuration B. Granulomatous inflammation with caseation C. Acute inflammation with abscess formation D. Perivascular inflammation with plasma cells E. Gummatous inflammation

62
Question 5 Explanation Answer: (D) Syphilitic chancres occur in the primary stage of syphilis and are characterized by lymphoplasmacytic infiltrates and by an obliterative endarteritis. Similar lesions also may appear with secondary syphilitic mucocutaneous lesions. Suppurative granulomas are typical of cat-scratch disease. Caseating granulomatous inflammation is more characteristic of tuberculosis or fungal infections. Acute inflammation with abscess formation is characteristic of bacterial infections such as gonorrhea. Gummatous inflammation can be seen in adults with tertiary syphilis or in congenital syphilis. Source: Robbins & Cotran Review of Pathology, 3rd ed, Ch.8- Infectious Diseases
 Syphilitic chancres occur in the primary stage of syphilis and are characterized by lymphoplasmacytic infiltrates and by an obliterative endarteritis. Similar lesions also may appear with secondary syphilitic mucocutaneous lesions. Suppurative granulomas are typical of cat-scratch disease. Caseating granulomatous inflammation is more characteristic of tuberculosis or fungal infections. Acute inflammation with abscess formation is characteristic of bacterial infections such as gonorrhea. Gummatous inflammation can be seen in adults with tertiary syphilis or in congenital syphilis. Source: Robbins & Cotran Review of Pathology, 3rd ed, Ch.8- Infectious Diseases.")
Similar presentations










 N. gonorrhoeae causes the sexually transmitted disease gonorrhoea. The gonococcus was first described by Neisser.>")



>")





; ch.16 Gonorrhea Chlamydia Syphilis.>")
