Download presentation
Presentation is loading. Please wait.

1
Demystifying the Past And Planning for the Future
Wisdom Tooth Wisdom Demystifying the Past And Planning for the Future Ted Fields, DDS, PhD

2
Part I: To Remove or Not to Remove
Course Outline Part I: To Remove or Not to Remove 1. Development 2. Wisdom teeth as an asset 3. Wisdom teeth as a liability 4. Alternatives to removal 5. Timing of removal

3
Part II: Treatment Approach
Course Outline Part II: Treatment Approach Assessing the difficulty of removal Patient counseling and preparation Anesthesia Instrumentation Technique

4
Management of Infected Teeth
Course Outline Part III: Management of Infected Teeth

5
Part IV: It Ain’t Over Till It’s Over
Course Outline Part IV: It Ain’t Over Till It’s Over Complications Post-operative care Documentation

6
The Difficulty in Understanding 3rd Molars
European third molar surgery is much different than that in the U.S. Lingual fracture technique Different instrumentation Different economic influences on dental care

7
The Difficulty in Understanding 3rd Molars
2. Many research papers of the past 20 years set out to prove or disprove old ideas – many of which themselves are outdated. Will the 3rd molar erupt? Is there enough arch length for eruption? Does removal of the 3rd molar compromise the 2nd molar?

8
The Difficulty in Understanding 3rd Molars
Much of the developmental literature is written from an orthodontic viewpoint. There is an outcome bias towards younger individuals (what is the result in a 16-yr-old?) The 3rd molar is judged in relation to orthodontic needs, rather than the patient’s overall needs.
 The 3rd molar is judged in relation to orthodontic needs, rather than the patient’s overall needs.")
9
The Difficulty in Understanding 3rd Molars
4. Many changes in technology have been totally neglected. Implants Electric handpieces Antibiotics Hemostatic agents Bone augmentation materials

10
The Difficulty in Understanding 3rd Molars
The topic is not covered in any depth in most dental schools. Knowing when it is in the patient’s best interest to remove 3rd molars is a judgment that requires detailed knowledge of the risks and benefits associated with tooth retention and with tooth removal.

11
Development

12
Initial calcification
Occurs as early as 7yrs, more typically age 9.

13
Crown Mineralization Usually completed by age 12 to 14.

14
Root Formation Usually half-formed by age 16.

15
Root Completion Fully formed roots with open apices are usually present by age 18.

16
Eruption Most teeth that will erupt are erupted by age 20.
95% of all teeth that will erupt are erupted by age 24. A limited number of third molars appear to erupt, at least to some degree, in young adults.

17
Predicting Eruption – Who Cares?
Does it matter if a wisdom tooth erupts? Does it matter when a wisdom tooth erupts?

18
The Key Issue Does it affect the Risk:Benefit Ratio?

19
Evaluating Risk:Benefit

20
Evaluating Risk:Benefit
Since “Risk of retention” and “Benefit of removal” are essentially the same concept, these terms may be combined. Since “Benefit of retention” essentially = 0, the equation may be simplified:

21
Evaluating Risk:Benefit
You must consider 2 separate assets of each risk and each benefit: Magnitude of risk or benefit Probability of risk or benefit

22
Magnitude Is it major or minor? Does it require hospitalization?
Is it permanent? Does it affect your daily routine? If so, for how long?

23
Probability The most overlooked aspect of most consultations.
Fortunately most real bad outcomes are real uncommon What is the likelihood of certain problems? How much does treatment alter this likelihood?

24
The Difficulty of Accurate Risk:Benefit Assessment
The literature is not very complete or very helpful. Complication rates vary widely. Different people view these complications very differently (complication doesn’t always equal perception of the complication) Ogden GR, Bissias E, Ruta DA, Ogston S: Quality of life following third molar removal: a patient versus professional perspective. Br Dent J 1998;185:
 Ogden GR, Bissias E, Ruta DA, Ogston S: Quality of life following third molar removal: a patient versus professional perspective. Br Dent J 1998;185:")
25
The Difficulty of Accurate Risk:Benefit Assessment
2. The wide variety of different complications and the wide range in the incidences of each potential complication result in a complex body of data to assimilate.

26
Risk:Benefit Are erupted 3rds more or less subject to disease?
Are erupted 3rds more or less beneficial?

27
Wisdom Teeth as an Asset

28
What Impacts Treatment?
Eruption into occlusion should not be the sole criterion of usefulness. The issue is not “can you save it” but “should you save it.”

29
Benefits of 3rds “Functional occlusion” – what is this?
Is it any different than just “occlusion”? Is all occlusion functional? Is all functional occlusion important? If so, is it all equally important? Without evaluating questions such as these, how can you determine the true benefit of 3rds?

30
Benefits of 3rds – Part II
Orthodontic repositioning to replace missing or grossly compromised 1st molars Transplantation – poor long-term survival With dental implants, these are rarely reasonable treatment alternatives.

31
Tooth Transplantation
Under ideal conditions, 27 oral surgeons transplanted 291 teeth: 5-yr survival rate: 76.2% 10-yr survival rate 59.6% Schwartz O, Bergman P, Klausen B: Resorption of autotransplanted teeth. A retrospective study of 291 transplantations over a period of 25 years. Int J Oral Surg 1985;14:

32
Conclusion 3rd molars provide no proven functional benefit and no obvious esthetic benefit. Rarely, they may provide a treatment option that, at best, is third-line treatment.

33
Wisdom Teeth as a Liability

34
What Impacts Treatment?
Failure of eruption should not be the sole criterion for removal. Successful eruption should not be the sole criterion for retention. Eruption is not always a “yes” or “no” proposition.

35
Problem #1 – Soft Tissue Even with adequate arch length and full eruption, 3rd molars are often surrounded by thin, unkeratinized, highly distensible lining mucosa of the buccal vestibule. Encourages pathogenic bacteria retention Poorly withstands hygiene measures

36
Problem #2 – Periodontal Compromise
Bone loss distal to the 2rd molar after removal of the 3rd molar is controversial, at best. Even with some loss of bone, the result is stable and cleansable – the goal of periodontal therapy.

37
Bone Loss Distal to the 2nd Molar
A reduction in pocket depth with no change in bone height on the distal of the 2nd molar. Szmyd and Hester Groves and Moore Grondahl and Lekholm

38
Bone Loss Distal to the 2nd Molar
Alveolar bone crest healing distal to the 2nd molar is enhanced in younger patients with incompletely developed 3rd molar roots. Ash, Costich, and Hayward Ziegler

39
Augmentation with Freeze-Dried Bone or Bone Substitutes
Why? There is no independent evidence of benefit Why graft a contaminated site? Why graft a site you can’t close primarily? Your goal is to maintain bone height on the distal of the 2nd molar without pocket formation, not to augment potential defects more posteriorly.

40
Augmentation: Conclusion
It won’t improve your outcome. It will undoubtedly increase your infection rate Why would you want to augment this area anyway?

41
Measuring Bone Height

46
Problem #2 – Periodontal Compromise
The role of pathogenic bacteria retention in 3rd molar pockets is unknown. How does this affect the rest of the dentition? Hygenic compromise of the 2nd molar can result in a difficult to restore situation if this tooth is lost.

51
How Do You Treat Missing 2nd Molars?
If the entire dentition is healthy and a mandibular 2nd molar needs extraction, what is the recommended treatment? Cantilevered abutment? Implant? Partial denture? Remove opposing tooth at same time? Nothing. Allow opposing tooth to supererupt.

52
The Missing 2nd Molar Dilemma
Your treatment plan for this scenario illustrates the value you place on 2nd molars. Most people will subconsciously do a cost:benefit analysis and conclude that restoration is not necessary.

53
Problem #3 – 3rd Molar Caries

54
Problem #3 – 3rd Molar Caries

58
Problem #4 – 2nd Molar Caries

65
Problem #5 - Infection Can turn an elective procedure into an urgent or emergent situation Unscheduled loss of work Increased pain and healing time Compromise of adjacent teeth Compromise of patient’s systemic health

66
Infection

67
Types of Infection Simple dental caries and periodontal disease
Pericoronitis Abscess Cellulitis Abscess extension into adjacent fascial spaces 5. Abscess spread to distant sites Recurrent infections Infections resistant to initial local and systemic treatment measures

68
Pericoronitis The most common cause of therapeutic 3rd molar removal.

69
Pericoronitis A failure of preventive measures
A failure of early recognition, or a failure to seek proper treatment A step along the pathway of infection Pericoronitis should be a warning sign that initiates immediate and aggressive treatment with careful observation.

70
Problem #6 - Resorption

71
Problem #7 - Supereruption

72
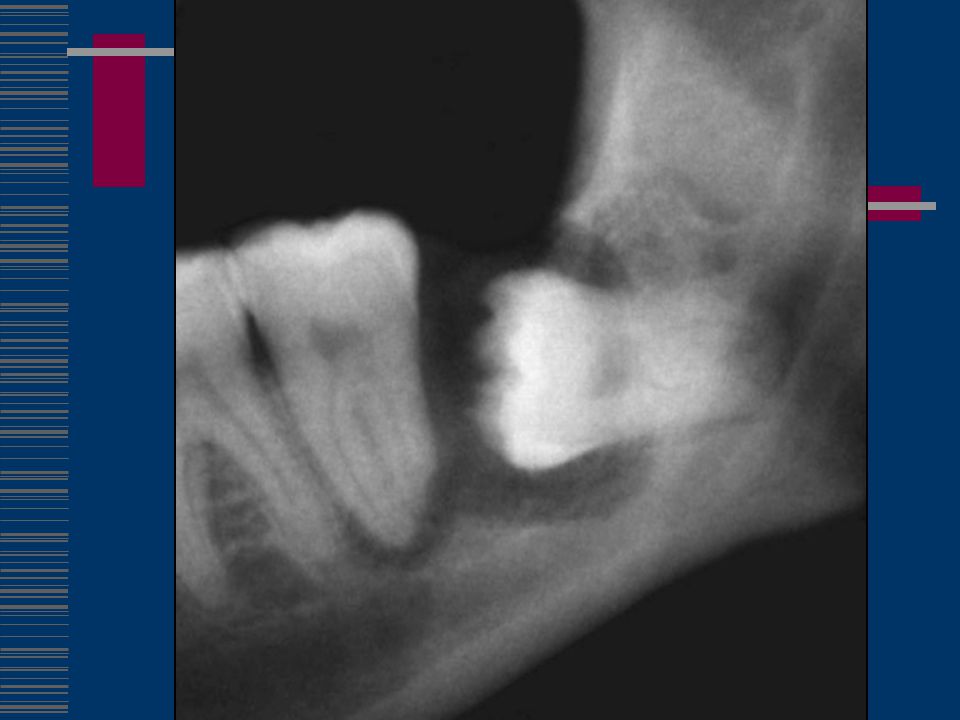
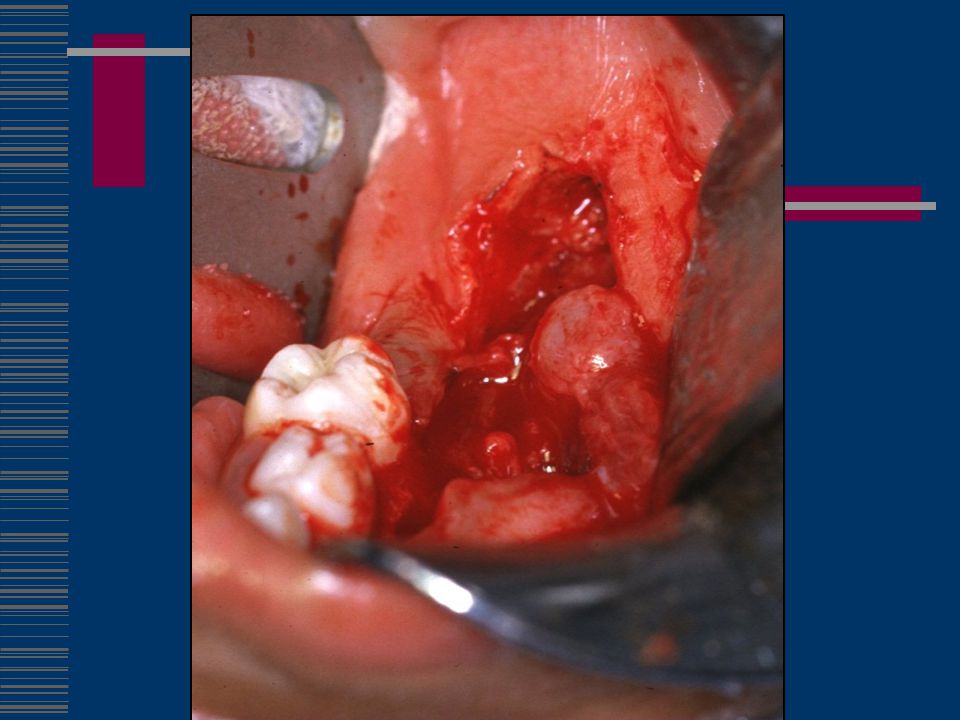
Problem #8 - Cysts Dentigerous Cyst

73
Dentigerous Cyst

74
Supernumerary 4th Molar Dentigerous Cyst

76
Types of Cysts Follicular cyst (Dentigerous Cyst)
OKC (Odontogenic Keratocyst) Ameloblastoma (several varieties) Not all radiolucencies are cysts! - Lymphoma - Myeloma - Metastatic carcinoma
 Ameloblastoma (several varieties) Not all radiolucencies are cysts! - Lymphoma. - Myeloma. - Metastatic carcinoma.")
77
Without the radiolucency, would you have recommended removal?
Is the removal of this better or worse with the radiolucency?

78
When would you recommend removal of this 3rd molar?

80
Cysts – A Few Facts May be prevented by early removal – when normal dental follicle is still evident. The pericoronal pocket, or residual follicle, is responsible for most cystic pathology. All cystic tissues should be removed and biopsied.

81
Cysts Cysts themselves are not catastrophic – the problem is that we don’t know exactly what they are until they are histopathologically examined – which necessitates removal. All cysts result in bone loss. Some cysts recur more than others.

82
Treatment of Large Cysts
Aspirate first – rule out vascular lesions Consider decompression (only after biospy confirmed diagnosis) Consider marsupialization Consider bone grafting Consider possibility of mandible fracture Consider extensive followup
 Consider marsupialization. Consider bone grafting. Consider possibility of mandible fracture. Consider extensive followup.")
89
Problem #9 - Tumors Benign vs. malignant
Odontogenic vs. non-odontogenic Primary vs. secondary Each of these factors has important treatment implications.

90
Tumors

96
Problem #10 – Risk of Fracture

97
Immediate Pre-extraction

98
Immediate Post-extraction

99
3 Days Post-extraction

100
8 Days Post-extraction

101
Problem #11 - Fracture

102
Problem #12 - Orthodontics
Prevent loss of post-retention stability Allow distalization of 2nd molars These are controversial indications

103
Alternatives to Removal
Restoration Periodontal therapy Operculectomy Removal of another tooth No treatment

104
When is the best time for prophylactic removal?
Timing Removal of 3rds When is the best time for prophylactic removal?

105
Age 7-11: Mandibular 3rds Germs are first visible during this time
They usually appear in a superficial location close to the alveolar crest After age 11, they are located deeper in the mandible

106
Age 7-11: Mandibular 3rds Very close to ridge crest. Minimal if any bone removal will be needed.

107
Age 7-11: Mandibular 3rds Mineralization is either not present or only mineralized cusps are evident Remove requires a flap and minimal, if any, bone removal Psychological factors and parental support should be carefully evaluated on a case by case basis

108
Age 7-11: Mandibular 3rds Close to, but not at, ridge crest. Some bone removal will be needed.

109
Age 7-11: Mandibular 3rds Bone removal will be necessary. Is it better to remove this 3rd molar or wait?

110
Age 7-11: Mandibular 3rds There has been less published about removal of thirds at this age than at other ages, so intervention at this time tends to be more controversial Much of the controversy has traditionally revolved around the difficulty in predicting eruption and arch length – probably not valid

111
Removing 3rd Molar Germs
Bjornland T, Haanaes HR, Lind PO, Zachrisson B: Removal of third molar tooth germs: study of complications. Int J Oral Maxillofac Surg 1987;16: Half as much postop pain medication was required One third quicker procedure Well-tolerated with local anesthesia

112
Age 7-11: Maxillary 3rds These teeth tend to be high in the maxilla
Their small size can make them difficult to locate Their size and location can increase the risk of injury to the developing 2nd molar Increased operating time and frustration Increased postop edema and discomfort

113
Age 7-11: Maxillary 3rds

114
Age 7-11: 3rd Molars

115
Age 7-11: 3rd Molars

116
Age 7-11: 3rd Molars

117
Age 7-11: Conclusion Lower 3rds are often very simple, upper 3rd are almost always very difficult and pose risk to the 2nd molars In older individuals, 90% of the morbidity is from removal of the lower 3rds Early removal may obviate the need for any sedation at any time Psychological evaluation is critical

118
Age 12 -14 Crown mineralization progresses
Distance of lower 3rds from ridge crest increases Lower 3rds become more difficult to remove Upper 3rds may still be quite difficult Psychologically, many patients may be less prepared at this age.

119
Age

120
Age

121
Age

122
Age 15-18 Root formation has begun and may progress to near completion. Most patients are psychologically accepting of surgery at this age. Most studies agree that complication rates are least in this age range.

123
Age 15-18

124
Age 15-18 The follicle allows for relatively easy removal once the tooth is accessed. No PDL is present – there is no attachment of the tooth to bone. The portion of the follicle deep to the forming roots acts as a safety zone between the tooth and the nerve.

125
Age 15-18 The periphery of the deepest mineralized tooth surface may be quite sharp, allowing laceration of the neurovascular bundle if it too is housed within the follicular space. The tooth may spin and be difficult to stabilize while sectioning and elevating.

126
Age 15-18

127
Age 15-18

128
Age 15-18

129
Age 19-22 Root development is not always complete during this period, making it still a favorable time for 3rd molar removal.

130
Age 22-35 Nearly all patients in this age group will have fully developed 3rd molar roots – this potential advantage is lost. The bone still has a good ratio of elastic collagen matrix to mineral content, usually simplifying removal and even more frequently improving most parameters of healing. Most of these patients are healthy.

131
Age 35-45 Most patients are still ASA I or II
The mineral content of the mandible increases during this time. Many 3rd molars must be removed during this time for therapeutic reasons.

132
Over Age 45 The complication rate is highest in this group.
The incidence of nerve injury is highest in this group – and recovery is the poorest. Even routine healing tends to be prolonged and associated with increased morbidity. Patient health may be compromised.

133
With Increasing Age Narrowing of PDL and pericoronal space
Thickening of cortical bone Increased risk of infection, bone loss, and other pathoses

134
Advantages of Early Removal
Wide pericoronal space Incomplete root development Straight roots Away from IAN Away from sinus Less risk of infection Less risk of fracture Patient more likely in good health Better chance for primary closure Smaller teeth require less bone removal

Similar presentations









































>")





