Download presentation
Presentation is loading. Please wait.

1
Principles Dental Public Health Oral Health Needs Assessment
دکتر سید ابراهیم جباری فر( (Dr. jabarifar تاریخ : 1389 / 2010 دانشیار دانشگاه علوم پزشکی اصفهان بخش دندانپزشکی جامعه نگر

2
Needs assessment • As a general rule, establishing the effectiveness of an intervention must be the most important step. • Most challenging of all is the task of apportioning relative priority to different services and recipients. Cost effectiveness must be taken into consideration

3
How is dental need usually assessed?
The most commonly used type of need assessment in oral health care planning is normative or professionally defined need. • However, despite its usefulness and extensive use, normative need is not free from limitations.

4
Needs assessment The purpose of needs assessment in health care IS to assess unmet health and health care needs in a systematic manner and to gather the information required to bring about change beneficial to the health of the population.

6
Planning health services:
The role of treatment needs assessment • Conversion of individual items into units of treatment Calculation of time and cost required. Calculation of relative costs to using dental teams of different types of dental personnel.

7
Need for health care Need can be defined as ability to benefit in some way from health care. The ability of a population to benefit from health care depends on two things: "The number of individuals affected, i.e. the incidence and prevalence of the condition under question. " The effectiveness of health services available to deal with it.

8
Shortcomings of normative measures
Lack of objectivity and reliability. Ignores consumer rights. Lack of consideration of health behaviours and compliance. Unrealistic paradoxical approach takes little account of limited resources.

9
Bradshaws concepts of need
Normative need: a state of oral health considered as in need for intervention by a practitioner. A professional dentist's assessment of need. For example, how many cavities, need for denture, need for orthodontics? • Perceived need: an individual's own assessment of their dental state. Their want for better oral health. • Expressed need or demand: those perceived needs that individuals convert into demand by seeking the assistance of a practitioner.

10
General ways needs and dental health are assessed
Dental public Health Dental Health Curative / Preventive Screening Education Resources Expensive Extractions Fillings Scaling Orthodontics Prosthetics Normative Preventive Curative Utilisation 5 A’s 3 C’s Function Normality No pain Aesthetics No 5 D’s 5Ds Felt

11
Shortcomings of normative measures Serious conceptual limitations
"Clinical measures tell us nothing about the functioning of the oral cavity or the person as a whole" (Locker 1989). "Clinical indices are essential for measuring oral disease; the problem arises when these indices are used as measures of health and treatment need" (Sheiham et al. 1982).
. Clinical indices are essential for measuring oral disease; the problem arises when these indices are used as measures of health and treatment need (Sheiham et al. 1982).")
12
Concepts of need There is frequently a large difference between normative need and perceived need: • In dentate older individuals, the treatment need was 85% less when using the socio-dental approach (perceived needs) as compared with normative assessment. • In edentulous subjects estimated treatment need dropped by about 40% when subjects were assessed using the socio-dental approach (perceived needs).
 as compared with normative assessment. • In edentulous subjects estimated treatment need dropped by about 40% when subjects were assessed using the socio-dental approach (perceived needs).")
13
A framework of questions to ask when assessing health needs
What is the size and nature of the problem? What are the current services? What do patients want? What are the most appropriate and effective (clinical and cost) solutions? What are the resource implications? What are the outcomes to evaluate change and the criteria to audit success?
 solutions What are the resource implications What are the outcomes to evaluate change and the criteria to audit success")
14
Need • Health care needs are those that can benefit from health care (health education, disease prevention, diagnosis, treatment, rehabilitation, terminal care). • Health needs incorporates the wider social and environmental determinants of health, such as deprivation, housing, diet, education, employment. This wider definition allows us to look beyond the confines of the medical model based on health services, to the wider influences on health.
. • Health needs incorporates the wider social and environmental determinants of health, such as deprivation, housing, diet, education, employment. This wider definition allows us to look beyond the confines of the medical model based on health services, to the wider influences on health.")
15
Need • Health needs assessment should not just be a method of measuring ill health, as this assumes that something can be done to tackle it. • Incorporating the concept of a capacity to benefit introduces the importance of effectiveness of health interventions, and attempts to make explicit what benefits are being pursued.

16
Need Need in health care is commonly defined as the capacity to benefit. • If health needs are to be identified then there should be an effective intervention available to meet these needs and improve health. There will be no benefit from an intervention that is not effective or there are no resources available to resource

17
Need Assessment of health needs is a systematic method of identifying unmet health and health care needs of a population, and making changes to meet these unmet needs. • It involves an epidemiological and qualitative approach to determining priorities, which incorporates clinical and cost-effectiveness and patients' perspectives. This approach must balance clinical, ethical, and economic considerations of need, that is what should be done, what can be done, and what can be afforded.

18
Need For individual practices and health professionals, health needs assessment provides the opportunity for: • describing the patterns of disease in the local population and the differences from district, regional, or national disease patterns; • learning more about the needs and priorities of their patients and the local population; • highlighting the areas of unmet needs and providing a clear set of objectives to work towards to meet these needs;

19
Need For individual practices and health professionals, health needs assessment provides the opportunity for: • deciding rationally how to use resources to improve their local population's health in the most effective and efficient way; • influencing policy, interagency collaboration, or research and development priorities; and • importantly it also provides a method of monitoring and promoting equity in the provision and use of health services and addressing health inequalities.

20
A measure of dental needs should include:
The wants of the individual. Wants are the individual's perceptions of their own dental care needs and depend on the oral health status of the individual, their perceptions of what is normal and what the possible benefits of treatment are, as well as on factors such as social class and education. A prescription of effective and acceptable treatments or cures and the skills required to carry out the care (division of labour).
.")
21
Quality of life: Background
• Today we are working with a concept which portrays health as a part of everyday living, an essential dimension of the quality of our lives. • Quality of life in this context implies the opportunity to make choices and to gain satisfaction from living. Health is thus envisaged as a resource which gives people the ability to manage and even to change their surroundings.

22
A measure of dental needs should include:
A clinical dimension based upon sound concepts of the life history of the diseases. A measure of impairment which incorporates functional measures to assess the impacts of the impairment. A measure of social dysfunction

23
Prevalence and incidence
Neither prevalence nor incidence necessarily equate with need but knowledge of these parameters is usually an essential starting point for the assessment of needs. Prevalence increases if incidence (or the rate of . relapse) increases. In health needs assessment it may be important to estimate both incidence and prevalence.
 increases. In health needs assessment it may be important to estimate both incidence and prevalence.")
24
Quality of life: Background
• The irony is that while so much of the challenge in health care is social - to enhance the capacity of individuals to perform desired roles and activities - the thrust of the health enterprise is substantially technologic and reductionist, treating complex socio-medical problems as if they are amenable to simple technical fixes

25
Sociodental indicators
• Sociodental indicators is the degree to which mouth disrupts various aspects of daily life. • Dental disorders does more than this. How does it impinge on some aspects such as self-esteem and embarrassment? • They provide information on the impact of oral disorders and the perceived need for dental care. • They are supplementary to the traditional clinical health measures.

26
Quality of life: Denfinitions
• "Quality of life is the degree to which a person enjoys the important possibilities of life" (Raphael et al. 1994). • "Health-Related Quality of Life (HRQoL) is a multifaceted concept that attempts to simultaneously assess how long and how well people live" (Guyatt et al. 1989).
. • Health-Related Quality of Life (HRQoL) is a multifaceted concept that attempts to simultaneously assess how long and how well people live (Guyatt et al. 1989).")
27
Need Different domains: Physical function Psychological function Social function

28
Sociodental indicators Chewing Capacity Index
• Ask them whether can chew 9 indicator foods. • Eating - avoid prepared foods. • Sleep and rest - disturbed. • Communication avoid smiling, difficulty in speaking. • Social interaction - embarrassment. • Avoid social contacts health/appearance. • Emotion behaviour - worry or concern. • Work loss.

29
Need Different domains: Impairments- pathology Disability Disavantage Handicap Socio psychological dimensions

30
What are Oral Health-Related Quality of Life (OHRQoL) measures?
"Measures that add a dimension of social impact to the clinical indicators" (Cohen and Jago 1976). "Measures of the extent to which oral conditions disrupt normal role functioning" (Nikias et al. 1979).
. Measures of the extent to which oral conditions disrupt normal role functioning (Nikias et al. 1979).")
31
What are Oral Health-Related Quality of Life (OHRQoL) measures?
"Measures of the extent that health status and conditions disrupt normal social-role functioning and bring about major changes in behaviour, such as inability to work, attend school, undertake parental or household duties" (Locker 1989).
.")
32
Application of HRQoL measures
Measuring the efficiency or effectiveness of medical interventions. Assessing the quality of care Estimating the health needs of a population Improving clinical decisions Understanding the causes and consequences of differences in health.

33
The justification for the existence of the dental profession in Britain
• Second, loss of efficiency "the individual is hurt by the toothache he suffers, but the community is equally harmed by the loss of efficiency in the individual which toothache can cause". • Third, pemanent disability "while pain is the most obvious immediate consequence of dental disease, disability can also follow if the teeth of the young are neglected and have to be removed". Fourth, disfigurement "including the aesthetic and psychological results of irregular or broken teeth".

34
What are Oral Health-Related Quality of Life (OHRQoL) measures?
Subjective indicators that provide information on the impacts of oral disorders and conditions, and the perceived need for oral health care. OHRQoL measures are complementary to clinical measures.

35
The justification for the existence of the dental profession in Britain
In 1956 Lord McNair gave ample evidence that it was the alleviation of the negative effects of the mouth on daily performances that justified the existence of dentistry as a profession: • First, pain and distress "it is the prevention of this pain and the distress it causes that the justification for dentistry in this country is to be found. On this ground alone, therefore, dentistry stands out as removing one of the commonest occasions of misery and distress".

36
How should need be assessed?
"New approaches to patient assessment and intervention are needed to extend the traditional model", Mechanic (1995)
")
37
How should need be assessed?
Answer: use a sociodental approach. Key factors in socio-dental approach: 1. Clinical dental measures. 2. Oral Health-Related Quality of Life indicators. 3. Behavioural propensity. 4. Evidence-based interventions.

39
OHRQoL measures: use in dental services
Subject centred approach Focuses on health WHY Large population surveys (Population profile and needs assessment planing Evaluation of interventions services (outcomes measures) WHERE Needs assessment (OHRQoL measures in combination with clinical measures and behavioural factors but not for progressive life threatening conditions) HOW
 WHERE. Needs assessment (OHRQoL measures in combination with clinical measures and behavioural factors but not for progressive life threatening conditions) HOW.")
42
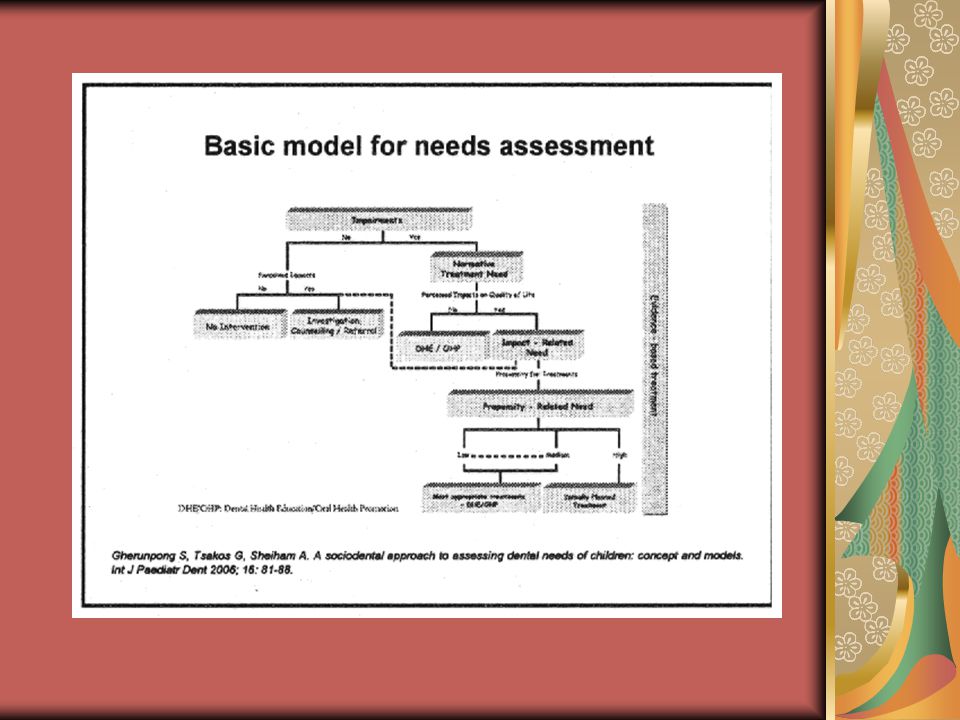
Example: malocclusions
Socio -dental needs Example: malocclusions Who has malocclusion? Normative Need (NN) Who should be treated first? Impact Related Need (IRN) Which types of treatment should be provided to those in need? (effectiveness + evidence) Propensity Related Need (PRN)
 Who should be treated first Impact Related Need (IRN) Which types of treatment should be provided to those in need (effectiveness + evidence) Propensity Related Need (PRN)")
43
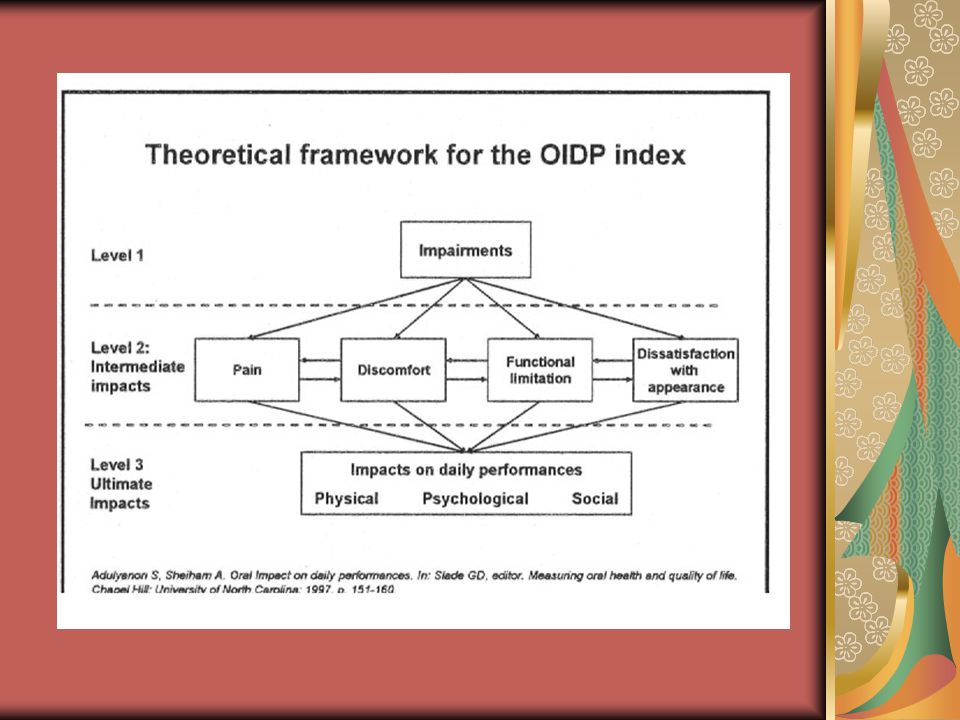
An Oral Health-Related Quality of Life index for needs assessment
The child version of the Oral Impacts on Daily Performances (Child-OIDP) assesses 8 items: Eating food Speaking clearly Cleaning mouth Relaxing, including sleeping Smiling, laughing and showing teeth without embarrassment Maintain usual emotional state without being initable Carrying out school work Enjoying contact with other people
 assesses 8 items: Eating food Speaking clearly Cleaning mouth. Relaxing, including sleeping. Smiling, laughing and showing teeth without embarrassment Maintain usual emotional state without being initable Carrying out school work. Enjoying contact with other people.")
45
Implications of the socio-dental treatment needs assessment
It will encourage a shift in emphasis away from the purely mechanical to the behavioural aspects of treatment It will support the development of a health-orientated model of care in preference to the model that dominates current dental services. It will promote the adoption of preventive behaviour by populations.

46
An Oral Health-Related Quality of Life index for needs assessment
The child OIDP includes three levels of measurement: • Impairment - oral status and conditions. • "Intermediate" impacts (pain, discomfort, functional limitation and dissatisfaction with appearance). • Ultimate impacts (disability and handicap). The OIDP and child OIDP focus on ultimate impacts
. • Ultimate impacts (disability and handicap). The OIDP and child OIDP focus on ultimate impacts.")
47
A socio-dental approach using OHRQoL measures
A key consideration when using OHRQoL measures in needs assessment is attributing OHRQoL impacts to specific oral conditions. How do we know that the impact on eating is caused by a specific condition (e.g. caries or missing teeth and lack of contacts) and need type (e.g. restorative or periodontal unmet need)? Answer: Using condition··specific scores of the Condition-Specific OIDP index (CS-OIDP).
 and need type (e.g. restorative or periodontal unmet need) Answer: Using condition··specific scores of the Condition-Specific OIDP index (CS-OIDP).")
48
Implications of the socio-dental treatment needs assessment
4. It will guarantee the higher effectiveness of treatment and a greater degree of long-term success. 5.It will facilitate a better division of fabour in providing dental care and an improvement in the use of scarce resources.

49
The Oral Impacts on Daily Performances (OIDP index)
Both OIDP and Child-OIDP provide a final score that incorporates the measurements of both frequency and severity of the oral impacts affecting daily living. They allow for the calculation of Condition-Specific scores (CS-OIDP), thus identifying causes of impacts and assisting in treatment needs assessment by relating particUlar impacts to a particular dental condition. OIDP theoretical framework is based on the WHO framework modified for dentistry by Locker (1989).
, thus identifying causes of impacts and assisting in treatment needs assessment by relating particUlar impacts to a particular dental condition. OIDP theoretical framework is based on the WHO framework modified for dentistry by Locker (1989).")
50
Propensity Related Need
Behaviours included in score will differ for each dental condition. For example: For dental caries would include tooth brushing patterns, sugars consumption patterns and fluoride use. For periodontal treatment include tooth brushing patterns and smoking.

51
Can it work ? Does it work ? Is it worth it?
Efficacy is the extent to which an intervention does more good than harm under ideal conditions ("Can it work?") Effectiveness assesses whether an. intervention does more good than harm when provided under usual circumstances of healthcare practice ("Does it work in practice?") Efficiency measures the effect of the intervention in relation to the resources it consumes ("Is it worth it?")
 Effectiveness assesses whether an. intervention does more good than harm when provided under usual circumstances of healthcare practice ( Does it work in practice ) Efficiency measures the effect of the intervention in relation to the resources it consumes ( Is it worth it )")
52
Propensity Related Need
Propensity to health promoting behaviours: Tooth brushing patterns Sugars consumption patterns ./ Fluoride use Dental attendance patterns ./ Smoking Drinking Give a score for each behaviour and then add them up to give overall score.

53
Effectiveness of interventions
Evidence-based oral health care is at the heart of the socio-dental approach: Critical literature appraisal/Systematic reviews: Cochrane Oral Health Group . Clinical guidelines Managerial task: "stop starting non-effective interventions" and "start stopping non-effective interventions already used" (Muir Gray 1997).
.")
54
Health gain" can be achieved by reallocating resources as a result of identifying:
Non-recipients of beneficial health care intervention (that is, unmet need); Recipients of ineffective health care (and releasing the resources for unmet need); Recipients of inefficient health care (and releasing resources for unmet need); and Recipients of inappropriate health care (for whom the outcomes could be improved).
; Recipients of ineffective health care (and releasing the resources for unmet need); Recipients of inefficient health care (and releasing resources for unmet need); and. Recipients of inappropriate health care (for whom the outcomes could be improved).")
58
THE SOCIO DENTAL APPROACH
EXAMPLE OF USE OF THE SOCIO DENTAL APPROACH

59
An Oral Health-Related Quality of Life index for needs assessment
The type of oral condition determines the choices of needs assessment pathway: 1. Life-threatening conditions such as orai cancer or pre-cancerous lesions, fractures or jaw, and severe infectious. 2. Chronic progressive oral conditions such as active dentinal caries. 3. Non-progressing such as malocclusion, enamel deformities, missing teeth, gingivitis.

61
Objectives To assess and compare the estimates of orthodontic treatment needs of grade-6 primary school children using: • The Normative approach. • The Socio-dental approach.

62
Material and Methods Design: a cross sectional survey Sample: 1034 grade 6 children (aged 11 to 12 years) Data collected: 1. Demographic information. 2. Normative need through the Index for Orthodontic Treatment Need (Brook and Shaw 1989(

65
4. Oral health behaviours (propensity):
Material and Methods Data collected: 3. Oral Health-Related Quality of Life (OHRQoL) through the Child-OIDP (Gherunpong et al. 2004) 4. Oral health behaviours (propensity): - The Simplified-Oral Hygiene Index (Greene and Vermillion 1964) - Dental attendance pattern: visit dentist when get appointment
 through the Child-OIDP (Gherunpong et al. 2004) 4. Oral health behaviours (propensity): - The Simplified-Oral Hygiene Index (Greene and Vermillion 1964) - Dental attendance pattern: visit dentist when get appointment.")
69
Implications of using OHRQoL measures for planning health services
• Encourage a shift in emphasis away from the purely mechanical to the behavioural aspects of treatment. • Support the development of a health-oriented model of care in preference to the model that dominates current health services. • Promote the adoption of preventive behaviour by populations.

70
Conclusions • Estimates of orthodontic need assessed normatively and socio-dentally differed markedly. The prevalence of NN and IRN was 35.0 and 10.5% respectively, thus representing a reduction of approximately 70 per cent in the volume of treatment need. • Children with IRN had different levels of propensity for treatment and required appropriate treatment plans according to their PRN. Of the 10.5% with IRN, 6.9% had high or medium-high PRN, while 3.6% were at medium-Iow and low levels of propensity.

71
Implications of using OHRQoL measures for planning health services
• Guarantee the higher effectiveness of treatment and a greater degree of long-term success. Facilitate a better division of labour in health care provision and an improvement in the use of scarce resources.

Similar presentations






























>")
