Download presentation
Presentation is loading. Please wait.

1
HCM 540 – Operations Management
Outpatient Clinics HCM 540 – Operations Management

2
Outline Simulation primer and OP clinic example
Clinic flow, measures, issues Open access Mathematics of appointments Information systems Clinic operations analysis cases

3
Simulation for Managers
Many healthcare systems horribly complex Difficult to estimate impact of changes to system on performance Much easier and less expensive to experiment with a model instead of the real system Discrete even simulation allows capture of variability and complex interactions in systems Handed out two nice introductions to computer simulation for healthcare managers a few weeks ago: Benneyan, J.C., An introduction to using computer simulation in healthcare: patient wait case study Mahachek, A.R., An introduction to patient flow simulation for health-care managers Example: An outpatient clinic simulation model

4
Simulation for Managers
Basic components of a simulation study: Study real system to understand problem and need for simulation Develop model of real system using simulation software Concurrently collect data on key inputs to simulation model (e.g. processing times, arrival rates) as well on on outputs (wait times) if possible Verify and validate model Iterate through above 3 steps, with user involvement, until everyone satisfied model is reasonable representation of reality Conduct controlled experiments with simulation model by running it for various combinations of input values Statistically analyze the output from the simulation experiments to draw conclusions, gain insights, support decision making Software – MedModel (ServiceModel), ProcessModel, Arena, Extend, GPSS, see
 as well on on outputs (wait times) if possible. Verify and validate model. Iterate through above 3 steps, with user involvement, until everyone satisfied model is reasonable representation of reality. Conduct controlled experiments with simulation model by running it for various combinations of input values. Statistically analyze the output from the simulation experiments to draw conclusions, gain insights, support decision making. Software – MedModel (ServiceModel), ProcessModel, Arena, Extend, GPSS, see")
5
Generic Flow Modeled Wait for Provider Initial wait

6
Using Simulation to Support Capacity Planning - Research
Ran set of simulation experiments for range of volumes, exam times, staffing levels, rooms/doc, prep location estimate initial wait time, wait time for provider, total time in clinic, length of clinic session Developed simple spreadsheet based model using Pivot Tables to find max volume subject to constraints on patient waiting and clinic length The data is output from the simulation experiements Currently developing regression and neural network based prediction models from the simulation experimental output Developing decision support tools FamPractice_v5.xls, ClinicWhatIfLookup-v4-Example.xls if interested in collaboration, please contact me

7
Decision support tool

8
Interest in Clinic/Office Operations & Management
IHIs initiative (started 1999) on the “Idealized Clinic Office Practice”
 on the Idealized Clinic Office Practice")
9
Improving Chronic Illness Care
Higher level view A Robert Wood Johnson Foundation program Bodenheimer, Wagner, & Grumbach (2002) Improving primary care for patients with chronic illness, JAMA 288(14), Bodenheimer, Wagner, & Grumbach (2002) Improving primary care for patients with chronic illness: The chronic care model, Part 2, JAMA 288(15),
 Improving primary care for patients with chronic illness, JAMA 288(14), Bodenheimer, Wagner, & Grumbach (2002) Improving primary care for patients with chronic illness: The chronic care model, Part 2, JAMA 288(15),")
10
Some Operational Inputs and Outputs
Performance Measures Input/Decision Variables Quality of care Appointment Lead Time Patient Wait Time – initial, for provider, repeat waits Patient Time in Clinic Length of clinic day Exam Room Utilization Support Space Utilization Provider and Support Staff Utilization Patient satisfaction Staff satisfaction Profitability Volume by Patient Type Provider and Support Staffing Appointment Scheduling Policies Exam Room Allocation Policies Patient Flow Patterns

11
A High Level Clinic Model Architecture
balk, renege Q 2 1 Models again help to organize our thinking about complex systems 3

12
A Simple Patient Flow Model
multiple waits Interfaces 28:5 Sep-Oct 1998 (pp.56-69)
")
13
A myriad of questions – demand?
Who is the underlying population to serve? What is the level of demand that can be satisfied by a clinic? How do you manage panels of patients for providers? what is the expected workload generated by a given panel of patients? What is the “appropriate panel size”? What are the basic types of patients served? Appointments, walk-ins, both? Demand for advance appt’s vs. same-day appointments

14
The Front Desk? How should the “front desk” be staffed?
appointment scheduling patient phone questions patient check in/out billing How long do patients wait on the phone for scheduling appts, medical questions, billing questions? What about information systems to support patient records, appointment scheduling, billing?

15
How is appointment capacity organized?
How much appointment vs. walk-in capacity is needed? appointment templates how many of each “type” of appointment to offer? how to best sequence mix of appointments? how to estimate length of time block for each type of appt? leave appt slots open for same day appointments? open access concept (Murray and Tantau) how many? how many and how to schedule different specialty “sub-clinics” within an OP Clinic
 how many how many and how to schedule different specialty sub-clinics within an OP Clinic.")
16
Appointment Templates
2 Template ID: Phys_Mon_AM_OB Provider Type: Physician Day / Time: Monday AM Clinic: OB How does one design good templates? how many each type? slot length? sequencing Template management Basis for generation of daily appointment schedules Start Slot Appointment Patients Time Length Type Per Slot 8:30 30 NEW 1 9:00 15 Postpartum 9:15 Follow Up 9:30 9:45 10:00 10:30 10:45 11:00 11:15 11:30

17
How is other resource capacity organized?
How many exam rooms per provider? are the rooms assigned? Do patients get appointments with specific providers? How much support staff needed? Where are various clinical interventions done? Who does them? How much waiting room capacity is needed?

18
Appointment scheduling?
Do you overbook? By how much? Performance measures for your overall appointment scheduling process? How do you measure how long your patients are waiting for an appointment? do you know when they want the appointment and whether their request was satisfied? How do you most effectively use appointment scheduling information systems?

19
Open Access Premise – adjust capacity as needed to meet customer demand One attempted response to chronic problem of delays to see primary care physician accommodate all appointment requests when patient wants developed by Kaiser Permanente (CA) popularized by Murray and Tantau (MT) Developed in early 1990s Recent articles in JAMA Three common models traditional access 1st generation open access 2nd generation open access
 popularized by Murray and Tantau (MT) Developed in early 1990s. Recent articles in JAMA. Three common models. traditional access. 1st generation open access. 2nd generation open access.")
20
Learning More About Open Acces

21
Appointment Access Methods

22
Traditional Access Stratify demand into urgent and non-urgent
See urgent now See non-urgent later Demand controlled by reservoir of supply Appts booked to end of queue, schedules get saturated, little holding of capacity for short-term demand Often multiple appt types Emphasis on matching demand to desired physician Urgent demand “added on” or “worked in” May lead to long appt lead times MT argue it artificially increases demand Focus on urgent condition only necessitates additional visits Diverted patients (e.g. different physician) end up coming back anyway – 1 visit becomes 2 visits
 end up coming back anyway – 1 visit becomes 2 visits.")
23
1st Generation Open Access A “carve out” approach
More “patient focused” I want to see my doc, and I want to see him/her now Premise: demand can be forecasted with sufficient accuracy to allow better matching of capacity to demand “Carve out” capacity each day for projected SDA demand Urgent vs. Routine appt stratification Developed by Dr. Marvin Smoller of Kaiser Permanente See Hawkins, S. “Creating Open Access to Clinic Appointments in the Henry Ford Medical Group” passed out in class

24
Some Problems with 1st Generation Open Access
Mismatches between patient and PCP Definition of “urgent” is fuzzy and changes as day goes on Creation of new appt types to meet urgent needs of patient who can’t come in today Queues for routine tend to grow gets shifted to use urgent capacity affects phone-in capacity and SDA capacity Black market or “second appt book” which fills “held” appts as they come available

25
2nd Generation Open Access
“Create capacity” by doing all today’s work today Providers responsible for panel, not appt slots No distinction between urgent and routine Appts are taken for the day the patient wants independent of capacity Every effort to match patient with PCP argued that this reduces “unnecessary demand” Challenges predict total demand provider flexibility panel management – how big?, how much work generated by a given panel?

26
2nd Generation Open Access What it is and what it is not…..
It is a theory designed to improve appointment access and customer satisfaction. It is not a rigid formula(s)….each clinic will implement the theory in the manner that works best for them. Demand is not insatiable. Staff is not in the office until all hours of the day and night. How Clinic X tried to convey open access concepts to staff and mgt
….each clinic will implement the theory in the manner that works best for them. Demand is not insatiable. Staff is not in the office until all hours of the day and night. How Clinic X tried to convey open access concepts to staff and mgt.")
27
Precursors to Open Access
Prospective demand measurement track actual demand for appts by patients (when they want slot, not when got slot) track provider requests for follow-up demand Panel sizes must be manageable and equitable no method can deal with demand>>capacity tying panel size to workload can be challenging Must estimate current supply # of providers, # of available appointment slots taking into account time each provider is actually in clinic Must eliminate backlog of appointments temporary increase in capacity through extended hours, weekends, etc. Reduce # of appt types PCP vs other short and long (e.g. long = 2xshort) Develop contingency plans dealing with short term imbalances in supply or demand Reduce and shape demand continuity of provider multiple issues at a visit group visits non-visit care (education, reference, self-care) Increase effective supply (especially of bottleneck resource) relieve providers of tasks that can be done by other Review call center processes, staffing, etc. to assure telephone access
 track provider requests for follow-up demand. Panel sizes must be manageable and equitable. no method can deal with demand>>capacity. tying panel size to workload can be challenging. Must estimate current supply. # of providers, # of available appointment slots taking into account time each provider is actually in clinic. Must eliminate backlog of appointments. temporary increase in capacity through extended hours, weekends, etc. Reduce # of appt types. PCP vs other. short and long (e.g. long = 2xshort) Develop contingency plans. dealing with short term imbalances in supply or demand. Reduce and shape demand. continuity of provider. multiple issues at a visit. group visits. non-visit care (education, reference, self-care) Increase effective supply (especially of bottleneck resource) relieve providers of tasks that can be done by other. Review call center processes, staffing, etc. to assure telephone access.")
28
Myths and Rumors at Clinic X
Correct Concept Myth/Rumor Appointment Scheduling Appointments are scheduled for when the patient would like to be seen. Appointment can be scheduled ahead of time (as far in advance as patient would like) Patient is driver of when to schedule appointment. Scheduled with PCP if in the office Cannot schedule return appointment until day want to be seen. PCP has to remain until patient is able to get to the office. Must add on as many patients as call to be seen that day. Insatiable Demand Patients are added on within a reasonable limit (contingency plans are developed). Providers are remaining in the clinic until all hours of the night. Teaming Providers are encouraged to form teams of 2-4 providers to care for patients. Teammates are utilized when PCP is out of the office. Patients still have PCP and see that individual as long as they are in the clinic. Must have only 2 people per team. Panel Size Panel size must be within reasonable limits. (Utilize Smoller’s demand model to help determine appropriate size). Panel is allowed to continue to grow without regard to demand. Appointment Types The pure theory dictates that there is no differentiation in appt types. Many clinics choose to continue with SDA (to maintain holds in the schedule). All appointments have to be 1 slot. All appointments are considered “routine” or same day. Overtime Support staff schedule is worked to decrease overtime and allow for provider support. People are staying late into the night with little support staff for assistance. Overall Many clinics are already doing a modified 2nd Generation Model and there are few changes. Drastic change in the way we do business.
 Patient is driver of when to schedule appointment. Scheduled with PCP if in the office. Cannot schedule return appointment until day want to be seen. PCP has to remain until patient is able to get to the office. Must add on as many patients as call to be seen that day. Insatiable Demand. Patients are added on within a reasonable limit (contingency plans are developed). Providers are remaining in the clinic until all hours of the night. Teaming. Providers are encouraged to form teams of 2-4 providers to care for patients. Teammates are utilized when PCP is out of the office. Patients still have PCP and see that individual as long as they are in the clinic. Must have only 2 people per team. Panel Size. Panel size must be within reasonable limits. (Utilize Smoller’s demand model to help determine appropriate size). Panel is allowed to continue to grow without regard to demand. Appointment Types. The pure theory dictates that there is no differentiation in appt types. Many clinics choose to continue with SDA (to maintain holds in the schedule). All appointments have to be 1 slot. All appointments are considered routine or same day. Overtime. Support staff schedule is worked to decrease overtime and allow for provider support. People are staying late into the night with little support staff for assistance. Overall. Many clinics are already doing a modified 2nd Generation Model and there are few changes. Drastic change in the way we do business.")
29
Questions/Concerns about Open Access?
Under what conditions would OA seem to be most applicable? When would it not be applicable and if so, are modifications possible? What is effect on care for chronic conditions? Will follow-up care slip through the cracks? Are we trading wait for an appointment for a wait at the clinic? What will day to day variation actually look like? How often will we be working until , say, 8pm? Effect on staff morale? How to actually implement? How to sustain? How pervasive and successful has it actually been? Impact on patient satisfaction? Impact on demand for visits? More...?

30
Measurements related to OA
Patient satisfaction: Quarterly reports - all levels of care Annual access satisfaction surveys Provider and staff satisfaction Availability of appointments compared to model Lead time for future appointments and/or “defect rate” Percentage of patients seeing own PCP and % seeing team member Telephone performance compared to standards: Average speed to answer Hold times Call abandonment rates Talk times Panel Size Visits per month

31
Resource Based Relative Value Units
Used as relative measure of clinical workload as well as basis for reimbursement by CMS Developed in late 1980’s by researchers from Harvard in conjunction with HCFA and physicians from numerous specialties Adopted in 1992 by HCFA RBRVUs also used to measure physician productivity performance monitoring incentive plans comparisons across departments panel management resource allocation Shortcomings as a productivity measure medical care has changed since 1988 RBRVU development especially with respect to pre and post-encounter work don’t fully account for effort for coordination of care, on-call, supervision of allied health professionals, remote communication with patients CPT coding basis not very detailed for E+M (evaluation & management) for OP visit for new patient, for OP visit for established patient E+M codes cannot be combined to reflect multiple E+M tasks done at 1 visit Limited reflection of complexity variation in patient populations, provider experience or quality of care See Johnson, S.E. and Newton, W.P. (2002) Resource-based Relative Value Units: A Primer for Academic Family Physicians, Family Medicine, 34(3), pp nice overview references include the original research leading to RBRVU development
 for OP visit for new patient, for OP visit for established patient. E+M codes cannot be combined to reflect multiple E+M tasks done at 1 visit. Limited reflection of complexity variation in patient populations, provider experience or quality of care. See Johnson, S.E. and Newton, W.P. (2002) Resource-based Relative Value Units: A Primer for Academic Family Physicians, Family Medicine, 34(3), pp nice overview. references include the original research leading to RBRVU development.")
32
Measuring Work Effort – “Panels”
How to translate a panel of patients to workload (# of visits, RVUs)? # of patients not a good measure of work different patient types generate different numbers and types of visits Why might you want to be able to put a workload measure to a panel of patients? How would you use it? What are practical difficulties with measuring physician workload? effect of FFS and HMO patients substitution of specialist and/or ER care for primary care covering for a colleague HFMG built regression models based on patient age, sex, and Ambulatory Diagnostic Group (ADG) to predict workload for a panel Kachal, S.K., Bronken, T., McCarthy, B., Schramm, W., Isken, N. – Performance measurement for primary care physicians, QQPHS 1996 Conference Proceedings (avail upon request) Have been using for the last 10 years for a variety of purposes
 # of patients not a good measure of work. different patient types generate different numbers and types of visits. Why might you want to be able to put a workload measure to a panel of patients How would you use it What are practical difficulties with measuring physician workload effect of FFS and HMO patients. substitution of specialist and/or ER care for primary care. covering for a colleague. HFMG built regression models based on patient age, sex, and Ambulatory Diagnostic Group (ADG) to predict workload for a panel. Kachal, S.K., Bronken, T., McCarthy, B., Schramm, W., Isken, N. – Performance measurement for primary care physicians, QQPHS 1996 Conference Proceedings (avail upon request) Have been using for the last 10 years for a variety of purposes.")
33
The Mathematics of Appt Scheduling
tradeoffs between patient & provider wait, length of clinic day, provider utilization appt time last patient x x x x x idle clinic run over end of exam patient wait individual appointments or blocks of patients given same appt time? (ex: 2 patients at start of day, then individual)
")
34
The Mathematics of Appt Scheduling
Decent amount of research on various simplified versions of the appt scheduling problem single patient type usually considered punctuality often assumed (patients and providers) simple patient care path (one visit to provider) Important variables mean exam time, coefficient of variation of exam time number of appts scheduled in a session punctuality, no-show rates relative wait cost ratio between providers and patients Some findings need good estimates of exam times relatively simple rules like scheduling 2 patients at the start of the clinic and then spacing appts out by mean exam time performed well in simulation experiments the “best” schedule depends on your objectives and parameter values impact on practice has been limited (O’Keefe, Worthington, Vissers)
 simple patient care path (one visit to provider) Important variables. mean exam time, coefficient of variation of exam time. number of appts scheduled in a session. punctuality, no-show rates. relative wait cost ratio between providers and patients. Some findings. need good estimates of exam times. relatively simple rules like scheduling 2 patients at the start of the clinic and then spacing appts out by mean exam time performed well in simulation experiments. the best schedule depends on your objectives and parameter values. impact on practice has been limited (O’Keefe, Worthington, Vissers)")
35
More about the math of appt scheduling
Handout – annotated bibliography of recent research in appointment scheduling Vissers, J. “Selecting a suitable appointment system in an outpatient setting”, Medical Care, XVII, No. 12, Dec Ho and Lau, “Minimizing total cost in scheduling outpatient appointments”, Management Science, 38, 12, Dec 1992. Vanden Bosch, P.M. and D.C. Dietz, “Scheduling and sequencing arrivals to an appointment system”, Bailey, N.T.J., “A study of queues and appointment systems in hospital outpatient departments”, J. Roy. Stat. Soc. B, 14, 185, 1952 first paper published about the topic of appt systems Fetter, R.B. and J.D. Thompson, “Patients waiting time and physicians’ idle time in the outpatient setting”, Health Services Research, 1, 66, 1966. another early classic

36
Information Technology and Appointment Scheduling/Practice Management
AppointmentsPro One-Call (Per-Se Technologies) Brickell Scheduler e-MDs Manage.md (ASP) The Medical Office Many more... The open source movement... Open source practice management projects MedPlexus – open source EHR initiative with AAFP OSCAR dev’d at McMaster in Canada stand alone appt scheduling vs. integrated with practice management single appointments vs. series of appointments comprehensive resource scheduling? enterprise wide vs. departmental? integration with existing IS? remote access? capacity price, vendor support, vendor viability
 Brickell Scheduler. e-MDs. Manage.md (ASP) The Medical Office. Many more... The open source movement... Open source practice management projects. MedPlexus – open source EHR initiative with AAFP. OSCAR. dev’d at McMaster in Canada. stand alone appt scheduling vs. integrated with practice management. single appointments vs. series of appointments. comprehensive resource scheduling enterprise wide vs. departmental integration with existing IS remote access capacity. price, vendor support, vendor viability.")
37
Case 1: A Partially Successful OR Engagement (Bennett and Worthington)
Ophthalmology clinic new and follow up patients Routine, Soon, Urgent Three ½ day clinic sessions per week 3 docs (11New, 33FollowUp for regular clinic) Overbooked, overrun, excessive patient waits Mr. T suspected the appt system Fundamental issue of matching capacity to demand “systems thinking” view User involvement Awareness of fit within broader organization Interfaces 28:5 Sep-Oct 1998 (pp.56-69)
 Overbooked, overrun, excessive patient waits. Mr. T suspected the appt system. Fundamental issue of matching capacity to demand. systems thinking view. User involvement. Awareness of fit within broader organization. Interfaces 28:5 Sep-Oct 1998 (pp.56-69)")
38
Why might not the clinic be running smoothly?
Patients late/early Doctors late No shows, cancellations Excessive overbooking Inappropriate appt lengths Highly variable consultation times Lack of data about operations Walk-ins Staff absences Understaffing Not enough space Not enough appt capacity Poor information flow Many more...

39
Vicious Circle of Insufficient Capacity and Overbooking
Interfaces 28:5 Sep-Oct 1998 (pp.56-69)
")
40
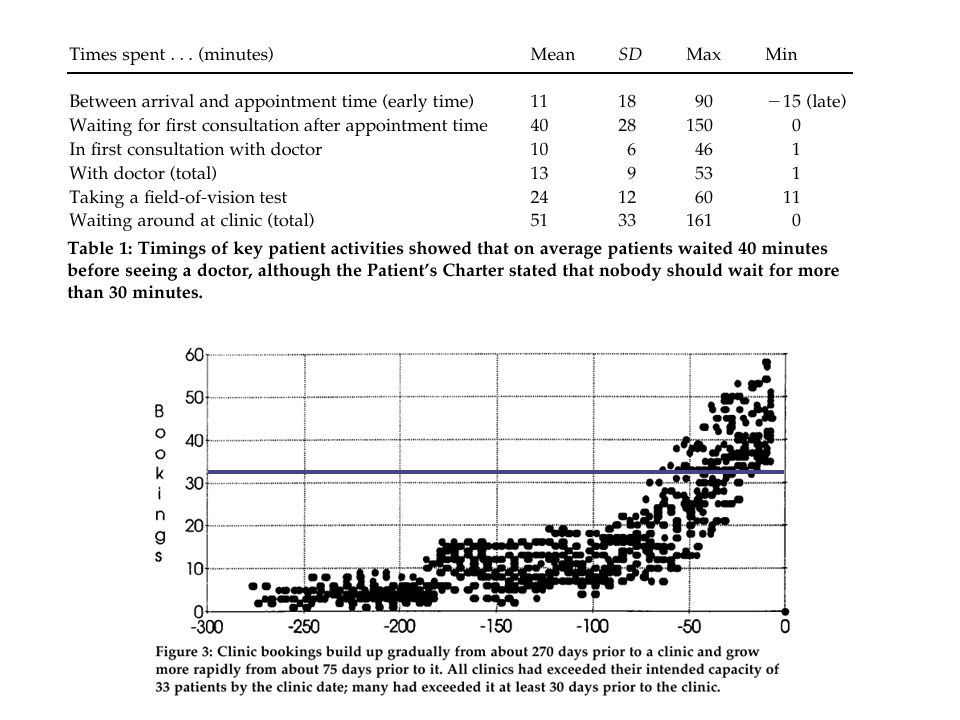
Analysis Highlights Consideration of both process and organizational issues Patients were generally punctual waited on avg 40 mins to see physician (51 mins including repeat waits) Simple model for “clinic appt build up” highlighted severity of demand>capacity If demand>capacity in long term, no appointment scheduling magic is going to help vacation notice deadline for providers Simple model to assess impact of lengthening time between routine visits an attempt to decrease demand Interfaces 28:5 Sep-Oct 1998 (pp.56-69)
 Simple model for clinic appt build up highlighted severity of demand>capacity. If demand>capacity in long term, no appointment scheduling magic is going to help. vacation notice deadline for providers. Simple model to assess impact of lengthening time between routine visits. an attempt to decrease demand. Interfaces 28:5 Sep-Oct 1998 (pp.56-69)")
42
Analysis Highlights Used specialized queueing model to explore different appt scheduling patterns as expected, by spacing out appts further, wait to see provider decreased but at increase in provider idleness of course, less appts will also exacerbate the difficulty in getting an appt Developed list of long term and shorter term operational strategies some were implemented to various degrees however, not much really changed over 2½ years OP Clinics are messy, complex, and different constituencies have different goals and objectives Simple models and “applied common sense” Interfaces 28:5 Sep-Oct 1998 (pp.56-69)
")
43
Demand Management Upstream Midstream Downstream population mgt
prevention and wellness self-care disease mgt manage chronic conditions Midstream walk-in or call-in coordinate with ancillary providers maximize visit efficiency match patient to provider group visits Downstream education telephone follow-up lengthen visit intervals change future point of service entry

44
Case 2: Simulation provides surprising staffing and operation improvements at family practice clinics (Allen, Ballash, and Kimball) Simulation quite useful for exploring impact of operational inputs on system performance Intermountain Health Care integrated health system based in Utah > 70 clinics, 840,000 enrollees, 2000 docs clinics ranged in size, configuration, operating tactics Developed generic clinic simulation model to explore impact of different configurations/tactics on performance MedModel – healthcare specific simulation development tool Paper has very nice description of a typical simulation analysis in healthcare Proceedings of the 1997 HIMSS Conference – available upon request

45
A few highlights and things to note ( from Allen, Ballash, and Kimball)
Started with “simple” model and added complexity as needed Obtained “patient treatment profiles” from healthcare consulting firm Fig 3,6 – “Low” MA utilization is “good” MA team had dramatic positive effect over assigned MAs – from 6 down to 4 MAs with only 4% ACLOS increase 3 rooms/doc not better than 2 per doc wait “moved” from waiting room to exam room Dedicating exam rooms to docs did not adversely impact performance – not the bottleneck Patient scheduling matters at higher workloads Overbooking had significant negative impact on patient waits Proceedings of the 1997 HIMSS Conference – available upon request

46
A few highlights and things to note ( from Allen, Ballash, and Kimball)
Used results as springboard to look at IHC clinics and how they operate Assessed feasibility of implementing insights gained from the modeling process Noted that significant changes (“reengineering”) of the patient care process will likely change the results of the analysis so, rerun it, that’s the beauty of having a model. Proceedings of the 1997 HIMSS Conference – available upon request
 of the patient care process will likely change the results of the analysis. so, rerun it, that’s the beauty of having a model. Proceedings of the 1997 HIMSS Conference – available upon request.")
47
More Resources http://www.ihi.org/idealized/idcop/
American Academy of Family Practice Family Practice Management Journal of Medical Practice Management Journal of the American Board of Family Practice Managed Care Quarterly Medical Group Management Journal

Similar presentations



















 MANAGEMENT Efficient &>")