Download presentation
Presentation is loading. Please wait.

1
Opiates and Opiate Pharmacology: A Research Perspective
D John Doyle MD PhD FRCPC Professor of Anesthesia November 3, 2006

2
Download this talk at opiateresearch.homestead.com

3
Outline History Kinds of opiates
Opiates vs. Narcotics (and Psychotic vs. Insane) Opiates and pain management Opiate receptors Opiates and the brain Opiates and respiratory depression Opiates and addiction Opiates and social policy Opiates and the search for artificial bliss
 Opiates and pain management. Opiate receptors. Opiates and the brain. Opiates and respiratory depression. Opiates and addiction. Opiates and social policy. Opiates and the search for artificial bliss.")
4
Journal Reports Laboratory Investigations Clinical Trials (many types)
Classical Reviews Systematic Reviews Best Evidence Reports Case Reports “How I Do It” Reports Safety Reports Pro / Con Debates Editorials Advocacy Pieces Statement of Hypotheses Letters to the Editor

5
Some Journal Types Peer-reviewed journals
Unreviewed paper archive collection Open peer commentary journals Open-access journals Medical education journals Newsletters Internet discussion forums

6
Opiates

7
The sedative, analgesic, and euphoric effects of opioids have been known since antiquity. First described by the Sumerians some 6,000 yr ago, the euphoric and analgesic properties of the seed-pod exudate of papaver somniferum are described in Homer's Iliad and were well known to physicians by the time of Hippocrates ( B.C.E.). However, since the time of Pliny the Elder (23-79 C.E.), it has also been known that opioids may produce life-threatening respiratory depression, which limits both their utility and their safety. From Anesthesiology: Volume 99(4) October 2003 pp
 October 2003 pp")
8
Papaver Somniferum

9
Opiates vs. Narcotics (and Psychotic vs. Insane)
Opiate – binds to opiate receptors Narcotic – legal term [U.S. Controlled Substances Act ] Example: Cocaine is a narcotic but not an opiate Psychotic – clinical term Insane – legal term “A person is insane, and is not responsible for criminal conduct if, at the time of such conduct, as a result of a severe mental disease or defect, he was unable to appreciate the nature and quality or the wrongfulness of his acts. This is because willfull intent is an essential part of most offenses; and a person who is insane is not capable of forming such intent. Mental disease or defect does not otherwise constitute a defense; the person has the burden of proving the defense of insanity by clear and convincing evidence.”

10
Opium Products

11
Grow your own poppies!!

13
Laudanum is an opium tincture, sometimes sweetened with sugar and also called wine of opium. It contains the equivalent of 10 milligrams of morphine per milliliter. Laudanum's weaker cousin, paregoric, also known as camphorated tincture of opium, is 1/25th the strength of laudanum, containing only 0.4 milligrams of morphine per milliliter. 1 grain = 65 mg

14
1 grain = 65 mg

16
Opium Wars The Opium Wars were two wars fought in the mid-1800s that were the climax of a long dispute between Britain and China concerning around the opium trade. The Chinese Emperor had banned opium in China due to its harmful effects on Chinese citizens and on Chinese culture; the British Empire, however, saw opium as a profitable good for commercial trade, as its import would help balance Britain's huge trade deficit with China. The Opium Wars and the unequal treaties signed afterwards led in part to the downfall of the Chinese Empire, as many countries followed Britain and forced more treaties to increase trade within China. Modified from

17
Early victims of the War On Drugs.
A battle-scene from the First Chinese Opium War ( )
")
18
DEA Schedule of Drugs

19
Morphine Morphine was first isolated in 1804 by the German pharmacist Friedrich Wilhelm Adam Sertürner, who named it "morphium" after Morpheus, the Greek god of dreams. But it was not until the development of the hypodermic needle (1853) that its use spread.
 that its use spread.")
22
"For instance, carfentanil is approximately 4000 times as potent as heroin and has an extremely favorable therapeutic index [...]. Hence, an easy week's work for two chemists could provide 1 (one) kilogram of carfentanil which would be equivalent to four metric tons of pure heroin“ Donald A. Cooper (DEA) in "Future Synthetic Drugs of Abuse“
![For instance, carfentanil is approximately 4000 times as potent as heroin and has an extremely favorable therapeutic index [...]. Hence, an easy week s work for two chemists could provide 1 (one) kilogram of carfentanil which would be equivalent to four metric tons of pure heroin](http://slideplayer.com/slide/1679342/7/images/22/For+instance%2C+carfentanil+is+approximately+4000+times+as+potent+as+heroin+and+has+an+extremely+favorable+therapeutic+index+%5B...%5D.+Hence%2C+an+easy+week+s+work+for+two+chemists+could+provide+1+%28one%29+kilogram+of+carfentanil+which+would+be+equivalent+to+four+metric+tons+of+pure+heroin.jpg "Donald A. Cooper (DEA) in Future Synthetic Drugs of Abuse")
23
Carfentanil synthesis:
[1] [2] US Pat. 5,106,983

24
It is thought that in the 2002 Moscow theater hostage crisis, the Russian military made use of an aerosol form of carfentanil to subdue Chechen hostage takers. Its short action, easy reversability and excellent therapeutic index (10600 vs. 300 for fentanyl) would make it a near-perfect agent for this purpose. Wax et al. (Ann Emerg Med 2003;41: ) surmise that the Moscow emergency services had not been informed of the use of the agent, and therefore did not have adequate supplies of naloxone or naltrexone (opioid antagonists) to prevent complications in many of the victims.
 would make it a near-perfect agent for this purpose. Wax et al. (Ann Emerg Med 2003;41: ) surmise that the Moscow emergency services had not been informed of the use of the agent, and therefore did not have adequate supplies of naloxone or naltrexone (opioid antagonists) to prevent complications in many of the victims..")
26
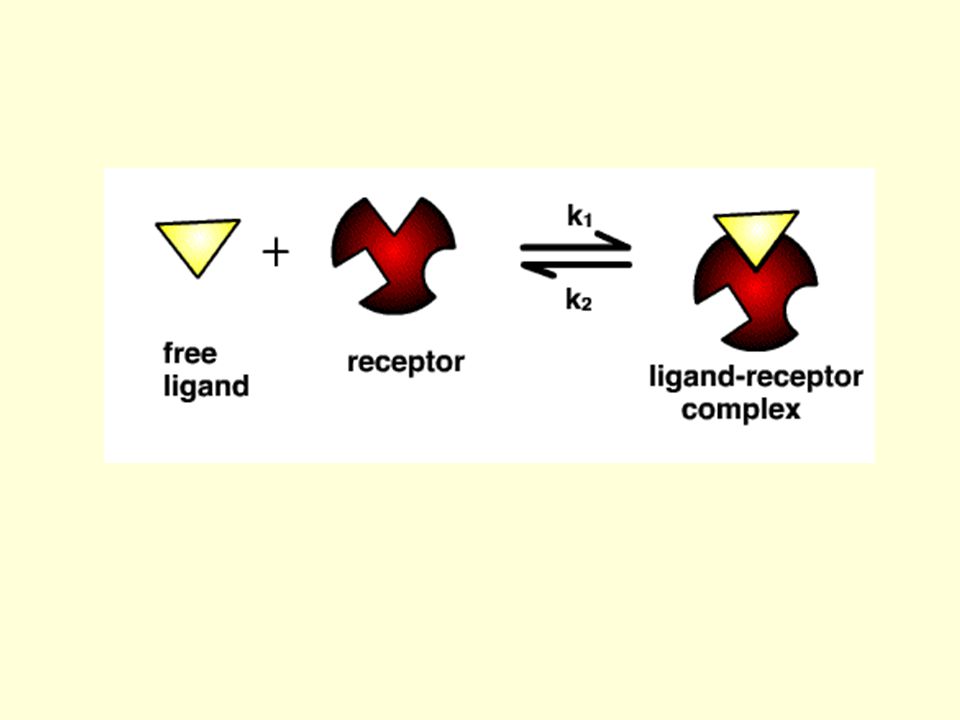
Opiate Receptors Discovered by Solomon Snyder and others in the 1970s
Discovery inspired by the teleological question why do drugs like morphine have the effect they do? (Endogenous opiate hypothesis) The endogenous opioid classes are dynorphins, enkephalins and endorphins.
 The endogenous opioid classes are dynorphins, enkephalins and endorphins.")
27
Solomon Snyder Many advances in molecular neuroscience have stemmed from Dr. Snyder's identification of receptors for neurotransmitters and drugs and elucidation of the actions of psychotropic agents. He pioneered the labeling of receptors by reversible ligand binding in the identification of opiate receptors and extended this technique to all the major neurotransmitter receptors in the brain. Discovering that human brains contain receptors to opiates such as heroin or morphine was another significant find. It led him and others to "natural" opiates, the enkephalins and endorphins that form the basis of the "runner's high." In 1978, the opiate work won Snyder a shared Lasker Award, the USA’s highest medical research honor.

28
Opioid Receptors There are three major subtypes of opioid receptors: μ (mu), κ (kappa), and δ (delta). The receptors were named using the first letter of the first ligand that was found to bind to them. Morphine was the first chemical shown to bind to mu receptors. The first letter of the drug morphine is `m'. But in biochemistry there is a tendency to use Greek letters so they converted the 'm' to μ. Similarly a drug known as ketocyclazocine was first shown to attach itself to kappa receptors. (
, κ (kappa), and δ (delta). The receptors were named using the first letter of the first ligand that was found to bind to them. Morphine was the first chemical shown to bind to mu receptors. The first letter of the drug morphine is `m . But in biochemistry there is a tendency to use Greek letters so they converted the m to μ. Similarly a drug known as ketocyclazocine was first shown to attach itself to kappa receptors. (")
29
Pasternak GW. Pharmacological mechanisms of opioid analgesics
Pasternak GW. Pharmacological mechanisms of opioid analgesics. Clin Neuropharmacol Feb;16(1): The description of multiple classes of opioid receptors has had a major impact on our understanding of the mechanisms of analgesia. Three major classes of opioid receptors have been defined: mu, kappa, and delta. The mu receptors have been further subclassified into two distinct subtypes (mu 1 and mu 2), as have the delta receptors (delta 1 and delta 2). Kappa receptors have been subdivided into kappa 1, kappa 2, or kappa 3 subtypes. All of these subtypes modulate pain perception, with the exception of the kappa 2 receptor, which has not been adequately examined. Supraspinal systems have been described for mu 1, kappa 3, and delta 2 receptors while mu 2, kappa 1, and delta 1 receptors modulate pain at the spinal level. In addition to their ability to act independently, the various systems also interact synergistically with each other. Thus, the relief of pain involves the complex interaction of at least six receptor systems. This review discusses the implications of opiate receptor multiplicity on the control of pain.
:1-18. The description of multiple classes of opioid receptors has had a major impact on our understanding of the mechanisms of analgesia. Three major classes of opioid receptors have been defined: mu, kappa, and delta. The mu receptors have been further subclassified into two distinct subtypes (mu 1 and mu 2), as have the delta receptors (delta 1 and delta 2). Kappa receptors have been subdivided into kappa 1, kappa 2, or kappa 3 subtypes. All of these subtypes modulate pain perception, with the exception of the kappa 2 receptor, which has not been adequately examined. Supraspinal systems have been described for mu 1, kappa 3, and delta 2 receptors while mu 2, kappa 1, and delta 1 receptors modulate pain at the spinal level. In addition to their ability to act independently, the various systems also interact synergistically with each other. Thus, the relief of pain involves the complex interaction of at least six receptor systems. This review discusses the implications of opiate receptor multiplicity on the control of pain.")
30
Activation of the mu receptor by an agonist such as morphine causes analgesia, sedation, reduced blood pressure, itching, nausea, euphoria, decreased respiration, miosis (constricted pupils) and decreased bowel motility often leading to constipation. Some of these effects, such as sedation, euphoria and decreased respiration, tend to disappear with continued use as tolerance develops. (

31
Tentative Classification of Opioid Receptor Subtypes and Their Actions
ANALGESIA RESPIRA- TORY GASTRO INTESTINAL ENDOCRINE OTHER Peripheral Gastric secretion GI transit - supraspinal and peripheral Antidiarrheal Skeletal muscle rigidity Pruritus ? Urinary retention (and/or ) Biliary spasm (probably >1 receptor type) Supraspinal Prolactin release Acetylcholine turnover Catalepsy 2 Spinal Respiratory depression GI transit – spinal and supraspinal Most cardiovascular effects ADH release Sedation 1 2 ? (Pharmacology unknown) 3 ? Respiratory depression GI transit – spinal Antidiarrheal – spinal and supraspinal ? Growth hormone release ? Urinary retention (and / or ) 1 Dopamine turnover 2 Unknown (receptor type not indentified) Pupillary constriction Nausea and vomiting Adapted from Pasternak GW: Pharmacological mechanisms of opioid analgesics. Clin Neuropharmacol 16:1, 1993.
 Biliary spasm (probably >1 receptor type) Supraspinal. Prolactin release. Acetylcholine turnover. Catalepsy. 2. Spinal. Respiratory depression. GI transit – spinal and supraspinal. Most cardiovascular effects. ADH release. Sedation. 1. 2. (Pharmacology unknown) 3. Respiratory depression. GI transit – spinal. Antidiarrheal – spinal and supraspinal. Growth hormone release. Urinary retention (and / or ) 1. Dopamine turnover. 2. Unknown (receptor type not indentified) Pupillary constriction. Nausea and vomiting. Adapted from Pasternak GW: Pharmacological mechanisms of opioid analgesics. Clin Neuropharmacol 16:1,")
32
Morin-Surun MP, Boudinot E, Gacel G, Champagnat J, Roques BP, Denavit-Saubie M. Different effects of mu and delta opiate agonists on respiration. Eur J Pharmacol Feb 17;98(2): The involvement of different opiate receptor subtypes in opiate-induced respiratory depression was studied in the unanaesthetized rat. Synthetic opioid agonists, specific for mu or delta receptors, were administered intraperitoneally in freely moving rats while respiratory parameters were recorded by means of the whole body plethysmographic method. TRIMU-4 (Tyr-D-Ala-Gly-NH-CH(CH3)-CH2-CH(CH3)2), a specific agonist of the mu receptor, reduced the tidal volume and did not change the respiratory frequency. DSLET (Tyr-D-Ser-Gly-Phe-Leu-Thr), a relatively specific agonist of the delta receptor subtype, reduced respiratory frequency and was significantly less effective on tidal volume than was TRIMU-4. It is concluded that the respiratory depression occurring after the administration of opiates in clinical practice is a dual complementary effect involving mu and delta receptors.
-CH2-CH(CH3)2), a specific agonist of the mu receptor, reduced the tidal volume and did not change the respiratory frequency. DSLET (Tyr-D-Ser-Gly-Phe-Leu-Thr), a relatively specific agonist of the delta receptor subtype, reduced respiratory frequency and was significantly less effective on tidal volume than was TRIMU-4. It is concluded that the respiratory depression occurring after the administration of opiates in clinical practice is a dual complementary effect involving mu and delta receptors.")
33
Mu Opiate Receptor Source: Goodman and Gillman 9th ed, p. 526

34
A map of the brain showing the concentration of mu receptors
A map of the brain showing the concentration of mu receptors. The red, orange and yellow areas have the highest concentrations of mu receptors, and therefore the most activity of opioid chemicals.

36
Mu Receptor - Transmembrane View

37
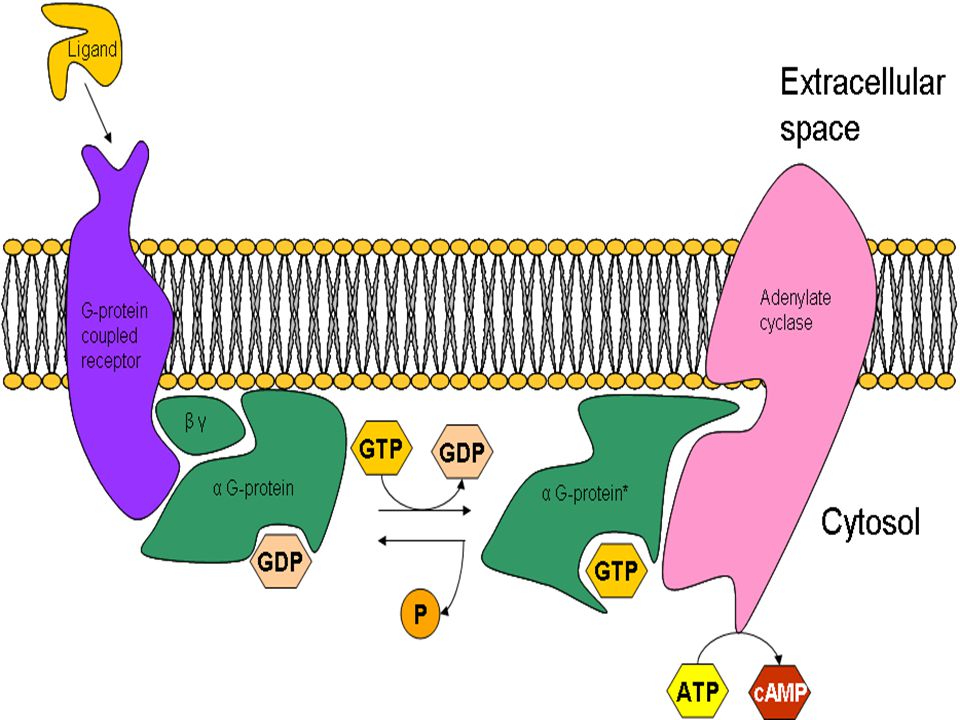
The opioid receptors belong to the G protein-coupled receptor family
The opioid receptors belong to the G protein-coupled receptor family. Opioid agonists like morphine bind to opioid receptors, leading to activation of the G-protein. Activity of adenylate cyclase and the voltage-dependent Ca2+ channels is suppressed, while inward rectifier K+ channels and the mitogen-activated protein kinase (MAPK) cascade are activated. Chronic exposure of the opioid receptors to agonists induces cellular adaptation mechanisms, which may be involved in opioid tolerance, dependence, and withdrawal symptoms.
 cascade are activated. Chronic exposure of the opioid receptors to agonists induces cellular adaptation mechanisms, which may be involved in opioid tolerance, dependence, and withdrawal symptoms.")
39
G protein-coupled receptors
Schoneberg, T., et al., Structural basis of G protein-coupled receptor function. Mol. Cell. Endocrinol., 151, (1999). LeVine, H., 3rd., Structural features of heterotrimeric G protein-coupled receptors and their modulatory proteins. Mol. Neurobiol., 19, (1999). Morris, A.J., et al., Physiological regulation of G protein-linked signaling. Physiol. Rev., 79, (1999).
. LeVine, H., 3rd., Structural features of heterotrimeric G protein-coupled receptors and their modulatory proteins. Mol. Neurobiol., 19, (1999). Morris, A.J., et al., Physiological regulation of G protein-linked signaling. Physiol. Rev., 79, (1999).")
40
Other Kinds of Receptors
The cannabinoid receptors are a class of receptors under the G-protein coupled receptor superfamily. Their ligands are known as cannabinoids. There are currently two known subtypes, CB1 which is expressed mainly in the brain, but also in the lungs, liver and kidneys and CB2 which is mainly expressed in the immune system and in hematopoietic cells. Mounting evidence suggests that there are novel cannabinoid receptors, that is, non-CB1 and non-CB2, which are expressed in endothelial and CNS. However, these have not been cloned yet. From

42
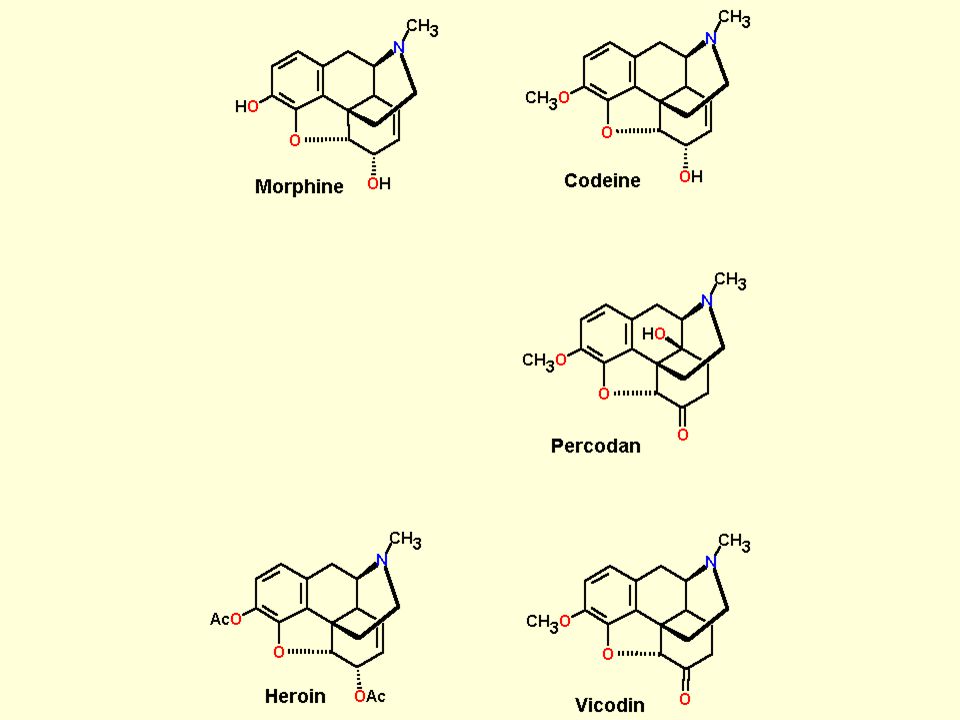
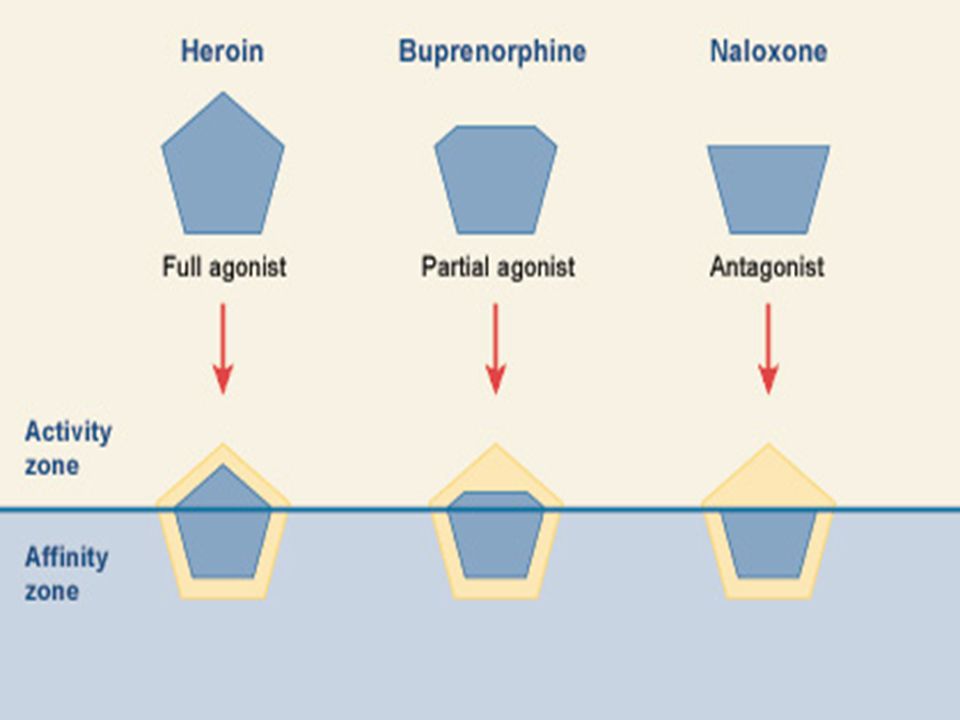
Kinds of Opiates Pure Opiate Agonists (e.g., morphine)
Mixed Agonist / Antagonists (e.g., nalbuphine) Opiate Antagonists (e.g., naloxone (Narcan®))
 Opiate Antagonists (e.g., naloxone (Narcan®))")
44
Opiate Agonists (partial list)
Opium Pantopon Morphine Meperidine (Demerol ® ) Hydrocodone Hydromorphone (Dilaudid®) Heroin Methadone Oxycodone Fentanyl Alfentanil Sufentanil Remifentanil Carfentanil
 Hydrocodone. Hydromorphone (Dilaudid®) Heroin. Methadone. Oxycodone. Fentanyl. Alfentanil. Sufentanil. Remifentanil. Carfentanil.")
45
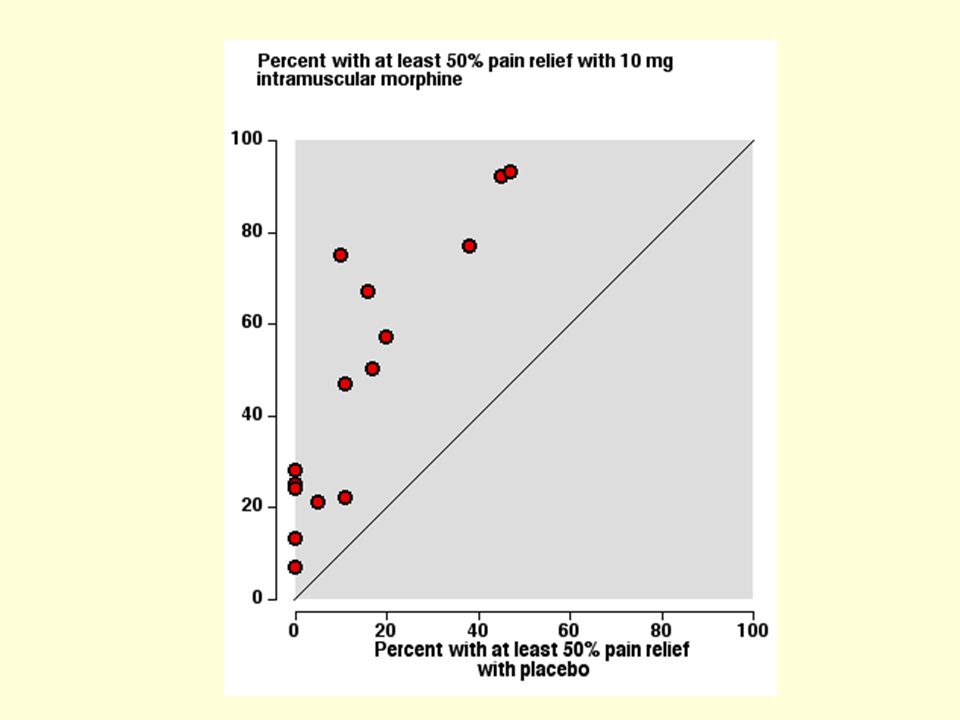
Why Opiates? Particularly effective in treating severe pain (kidney stones, orthopedic surgery) Dirt cheap (morphine 10 mg IV costs under 25 cents) Effective in lower doses when used in conjunction with less effective analgesics (e.g., acetaminophen, NSAIDs) Remarkably nontoxic to liver, kidneys BUT …..
 Remarkably nontoxic to liver, kidneys. BUT …..")
46
Problems with Opiates Respiratory depression Addiction / dependence
Less important issues: Constipation Itching Nausea / vomiting Mental clouding

47
Celebrity Heroin Overdoses
Jonathan Melvoin — 34, keyboardist for the rock band Smashing Pumpkins Brad Nowell — 28, vocalist for the punk rock band Sublime Kristin Pfaff — 27, bass player with the grunge rock band Hole River Phoenix — 23, film star of such movies as “My Private Idaho,” of a drug overdose. Autopsy blood test verified the presence of lethal levels of heroin, cocaine, alcohol and valium in his blood at the time of death. Stefanie Sargeant — 25, guitarist with the grunge rock band 7 Year Bitch John Belushi — 33, star of “Animal House” and “Saturday Night Live,” of a drug overdose after injecting a heroin-cocaine mixture commonly called a “speedball.” Darby Crash — 22, lead vocalist for the punk rock band Darby Crash & The Germs Sid Vicious — 21, bass player for the punk rock band The Sex Pistols Janis Joplin — 30, legendary rock star found dead at Hollywood’s Landmark Hotel

48
Heroin Users Warned About Deadly Additive
By Peter Slevin and Kari Lydersen Washington Post June 4, 2006 CHICAGO -- The largest clue that something had changed in Chicago's vibrant heroin market came in February, when police found a dozen users sprawled unconscious in one place. One day in April, there were dozens more. Toxicologists at the Cook County morgue discovered fentanyl, a powerful painkiller many times stronger than morphine, in the bodies of addicts who died. A small amount of fentanyl in a dose of heroin adds a pop that many users have come to crave.

50
CMAJ • September 19, 2000 Battling opiate overdoses D. John Doyle I thoroughly enjoyed your recent articles on substance abuse in the June 13 issue of CMAJ, especially Kyle Stevens' essay. I cannot help but think that if the narcotic antagonist naloxone was made readily available to heroin addicts and others as a harm reduction measure (perhaps as an expansion of a needle exchange program) there would be fewer deaths from opiate overdose. After all, most addicts would have little trouble subcutaneously or intravenously injecting naloxone into an unresponsive friend while awaiting a 911 response, and the drug would certainly not be used for recreational purposes. Indeed, this idea is being seriously explored in the addiction literature.
 there would be fewer deaths from opiate overdose. After all, most addicts would have little trouble subcutaneously or intravenously injecting naloxone into an unresponsive friend while awaiting a 911 response, and the drug would certainly not be used for recreational purposes. Indeed, this idea is being seriously explored in the addiction literature.")
51
BEST EVIDENCE TOPIC REPORT
Emergency Medicine Journal 2006;23: Intranasal naloxone in suspected opioid overdose ABSTRACT A short cut review was carried out to establish whether intransasal naloxone is effective in suspected opiate overdose. 596 papers were screened, of which eight presented the best evidence to answer the clinical question. The author, date and country of publication, patient group studied, study type, relevant outcomes, results and study weaknesses of these best papers are tabulated. The clinical bottom line is that it is likely that intranasal Naloxone is a safe and effective first line prehospital intervention in reversing the effects of an Opioid overdose and helping to reduce the risk of needle stick injury. A large, well conducted trial into it’s usage is however required to confirm this.

52
Rapid Opiate Detoxification And Naltrexone Induction
Rapid Opiate Detoxification is a method of rapidly detoxifying the body of opiates without the patient experiencing significant withdrawal. This is done under general anesthesia and takes 4 to 8 hours. Being unconscious, the patient does not experience the agonizing withdrawal symptoms of quitting "cold turkey” reducing the potential of an individual returning to using as a result of the withdrawal symptoms. AAROD = Anesthesia Assisted Rapid Opiate Detoxification

53
Rapid Opiate Detoxification: Too Good to Be True?
Induce general anesthesia, including IV access, tracheal intubation, positive pressure ventilation, full monitoring Titrate in large dose of IV naltrexone or naloxone to displace all opiates from the receptors Manage the resulting metabolic / hemodynamic storm with vasodilators, beta blockers and other drugs (akin to a pheochromcytoma storm) 8 hours later, wake up the now detoxified patient BUT …
 8 hours later, wake up the now detoxified patient. BUT …")
54
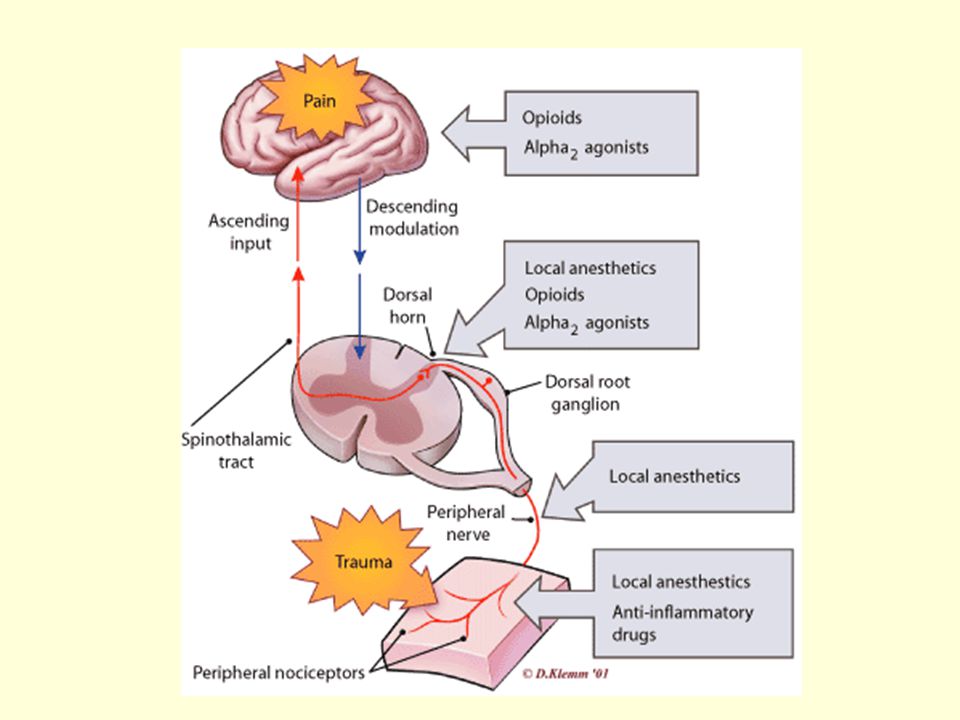
Opiates in Pain Management Landmine Injury ( MEPERIDINE

56
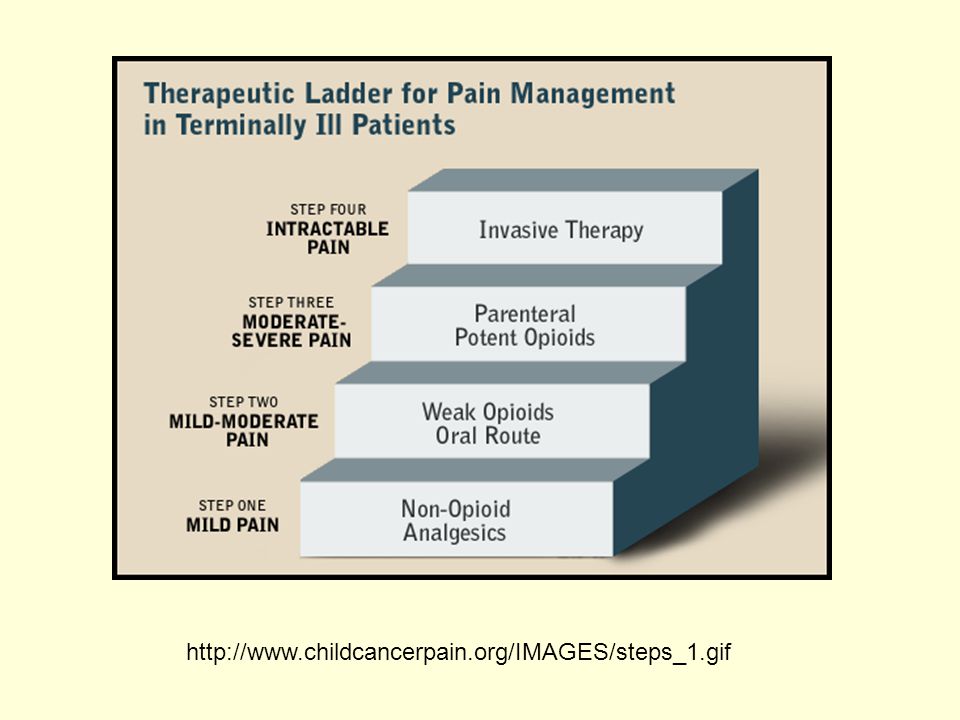
Classes of Analgesics: The WHO Pain Management Ladder
WHO has developed a four-step "ladder" for pain relief. If pain occurs, there should be prompt oral administration of drugs in the following order: [1] nonopioids (aspirin and acetaminophen); then, as necessary, [2] mild opioids (codeine); then [3] strong opioids such as morphine, until the patient is free of pain. To calm fears and anxiety, additional drugs – “adjuvants” – should be used. To maintain freedom from pain, drugs should be given “by the clock”, that is every 3-6 hours, rather than “on demand”. Surgical intervention on appropriate nerves may provide further pain relief if drugs are not wholly effective [Step 4].
; then, as necessary, [2] mild opioids (codeine); then [3] strong opioids such as morphine, until the patient is free of pain. To calm fears and anxiety, additional drugs – adjuvants – should be used. To maintain freedom from pain, drugs should be given by the clock , that is every 3-6 hours, rather than on demand . Surgical intervention on appropriate nerves may provide further pain relief if drugs are not wholly effective [Step 4].")
59
Postop Pain Therapy Examples
Tylenol #3 1 to 2 tabs PO q4h prn Morphine 5-10 mg IM or SQ q4h prn Morphine 2-4 mg IV q1h prn Meperidine 100 mg IM q3h prn Morphine 5 mg via epidural catheter q12h Morphine IV PCA 1.5 mg IV with lockout 6 minutes and max hourly dose of 10 mg.

60
Patient Controlled Analgesia

61
Patient-controlled analgesia. D. John Doyle and Kim J. Vicente
CMAJ • March 6, 2001; 164 (5) Patient-controlled analgesia. D. John Doyle and Kim J. Vicente Patient-controlled analgesia (PCA) is a computer-based medical technology now used extensively in Canada to treat postoperative pain. A typical PCA machine contains an embedded microcomputer programmed to give, for instance, 1 mg of morphine intravenously every time the patient pushes a button on the end of a cable. To prevent excessive drug administration, the onboard computer ignores further patient demands until a lockout period (usually set for 5–10 minutes) has passed. Recently, the Institute for Safe Medication Practices reported that a patient had received a lethal morphine overdose while connected to the Abbott Lifecare 4100 PCA Plus II machine. This machine is easily misprogrammed by caregivers, who must manually enter the PCA parameters, and it needs a more sensible and forgiving user interface. A number of patients have received opiate overdoses as a result of PCA errors: insertion of a 5 mg/mL morphine cartridge when the machine is expecting a 1 mg/mL concentration, or acceptance of the default (initial) drug concentration when the correct action is to scroll up to the correct value, among other errors. In 1997, ECRI documented 3 deaths that occurred while patients were connected to the Lifecare In at least 2 of the cases, the alleged reasons for the deaths were the same. In the mode of operation in use, when nurses program the drug concentration the Lifecare 4100 display shows a particular concentration (e.g., 0.1 mg/mL). Nurses can either accept this initially displayed value or modify it using the arrow controls. The critical flaw in the design is that in this situation the Lifecare 4100 offers the minimal drug concentration as the initial choice. If nurses mistakenly accept the initially displayed minimal value (e.g., 0.1 mg/mL) instead of changing it to the correct (and higher) value (e.g., 2.0 mg/mL), the machine will "think" that the drug is less concentrated than it really is. As a result, it will pump more liquid, and thus more narcotic, into the patient than is desired. The purpose of this letter is to warn clinicians of continuing fatal drug overdoses from the Abbott Lifecare 4100 PCA Plus II machine. If you use this machine, please contact your risk management officer and your biomedical engineering department for advice. Fortunately, Abbott is not the only supplier of PCA machines. We have informed American and Canadian regulatory authorities; they are, of course, now studying the problem.
 Patient-controlled analgesia. D. John Doyle and Kim J. Vicente. Patient-controlled analgesia (PCA) is a computer-based medical technology now used extensively in Canada to treat postoperative pain. A typical PCA machine contains an embedded microcomputer programmed to give, for instance, 1 mg of morphine intravenously every time the patient pushes a button on the end of a cable. To prevent excessive drug administration, the onboard computer ignores further patient demands until a lockout period (usually set for 5–10 minutes) has passed. Recently, the Institute for Safe Medication Practices reported that a patient had received a lethal morphine overdose while connected to the Abbott Lifecare 4100 PCA Plus II machine. This machine is easily misprogrammed by caregivers, who must manually enter the PCA parameters, and it needs a more sensible and forgiving user interface. A number of patients have received opiate overdoses as a result of PCA errors: insertion of a 5 mg/mL morphine cartridge when the machine is expecting a 1 mg/mL concentration, or acceptance of the default (initial) drug concentration when the correct action is to scroll up to the correct value, among other errors. In 1997, ECRI documented 3 deaths that occurred while patients were connected to the Lifecare In at least 2 of the cases, the alleged reasons for the deaths were the same. In the mode of operation in use, when nurses program the drug concentration the Lifecare 4100 display shows a particular concentration (e.g., 0.1 mg/mL). Nurses can either accept this initially displayed value or modify it using the arrow controls. The critical flaw in the design is that in this situation the Lifecare 4100 offers the minimal drug concentration as the initial choice. If nurses mistakenly accept the initially displayed minimal value (e.g., 0.1 mg/mL) instead of changing it to the correct (and higher) value (e.g., 2.0 mg/mL), the machine will think that the drug is less concentrated than it really is. As a result, it will pump more liquid, and thus more narcotic, into the patient than is desired. The purpose of this letter is to warn clinicians of continuing fatal drug overdoses from the Abbott Lifecare 4100 PCA Plus II machine. If you use this machine, please contact your risk management officer and your biomedical engineering department for advice. Fortunately, Abbott is not the only supplier of PCA machines. We have informed American and Canadian regulatory authorities; they are, of course, now studying the problem.")
62
What is Action Research?
Action research is often aimed at achieving a particular social goal, such as eliminating disparities in access to health care or improving patient safety

63
Canadian Journal of Anesthesia 50:328-332 (2003)
")
64
Canadian Journal of Anesthesia 50:328-332 (2003)
Purpose: To identify the factors that threaten patient safety when using patient-controlled analgesia (PCA) and to obtain an evidence-based estimate of the probability of death from user programming errors associated with PCA.
 and to obtain an evidence-based estimate of the probability of death from user programming errors associated with PCA.")
65
Canadian Journal of Anesthesia 50:328-332 (2003)
Clinical features: A 19-yr-old woman underwent Cesarean section and delivered a healthy infant. Postoperatively, morphine sulfate (2 mg bolus, lockout interval of six minutes, four-hour limit of 30 mg) was ordered, to be delivered by an Abbott Lifecare 4100 Plus II Infusion Pump. A drug cassette containing 1 mg•mL-1 solution of morphine was unavailable, so the nurse used a cassette that contained a more concentrated solution (5 mg•mL-1). 7.5 hr after the PCA was started, the patient was pronounced dead. Blood samples were obtained and autopsy showed a toxic concentration of morphine. The available evidence is consistent with a concentration programming error where morphine 1 mg•mL-1 was entered instead of 5 mg•mL-1. Based on a search of such incidents in the Food and Drug Administration MDR database and other sources and on a denominator of 22,000,000 provided by the device manufacturer, mortality from user programming errors with this device was estimated to be a low likelihood event (ranging from 1 in 33,000 to 1 in 338,800), but relatively numerous in absolute terms (ranging from 65–667 deaths).
 was ordered, to be delivered by an Abbott Lifecare 4100 Plus II Infusion Pump. A drug cassette containing 1 mg•mL-1 solution of morphine was unavailable, so the nurse used a cassette that contained a more concentrated solution (5 mg•mL-1). 7.5 hr after the PCA was started, the patient was pronounced dead. Blood samples were obtained and autopsy showed a toxic concentration of morphine. The available evidence is consistent with a concentration programming error where morphine 1 mg•mL-1 was entered instead of 5 mg•mL-1. Based on a search of such incidents in the Food and Drug Administration MDR database and other sources and on a denominator of 22,000,000 provided by the device manufacturer, mortality from user programming errors with this device was estimated to be a low likelihood event (ranging from 1 in 33,000 to 1 in 338,800), but relatively numerous in absolute terms (ranging from 65–667 deaths).")
66
Canadian Journal of Anesthesia 50:328-332 (2003)
Conclusion: Anesthesiologists, nurses, human factors engineers, and device manufacturers can work together to enhance the safety of PCA pumps by redesigning user interfaces, drug cassettes, and hospital operating procedures to minimize programming errors and to enhance their detection before patients are harmed.

67
Correspondence Programming errors from patient-controlled analgesia Jonathan D. Lamb, MD FRCPC To the Editor: I read with interest this case report of the tragic death of a young woman while receiving patient-controlled analgesia (PCA) post-Cesarean delivery. The authors conclude their report with several recommendations. These are all very sensible. The most important recommendation, not mentioned however, concerns the initial nursing assessment of a loudly snoring and unarousable patient while receiving PCA on the ward. This obviously can be an urgent and life-threatening situation which must be dealt with expeditiously. Typically a nursing protocol exists which provides for an immediate and effective response. Did this not exist, or, if so, was it not followed? A different and more favourable outcome might have resulted. An astute and appropriately trained nurse is the last line of defense for a wide range of untoward and potentially critical situations, such as could arise from a PCA programming error. This, in my opinion, is the paramount message in this tragic case, and not the programming error itself. Reference Vicente KJ, Kada-Bekhaled K, Hillel G, Cassano A, Orser BA. Programming errors contribute to death from patient-controlled analgesia: case report and estimate of probability. Can J Anesth 2003; 50: 328–32.
 post-Cesarean delivery. The authors conclude their report with several recommendations. These are all very sensible. The most important recommendation, not mentioned however, concerns the initial nursing assessment of a loudly snoring and unarousable patient while receiving PCA on the ward. This obviously can be an urgent and life-threatening situation which must be dealt with expeditiously. Typically a nursing protocol exists which provides for an immediate and effective response. Did this not exist, or, if so, was it not followed A different and more favourable outcome might have resulted. An astute and appropriately trained nurse is the last line of defense for a wide range of untoward and potentially critical situations, such as could arise from a PCA programming error. This, in my opinion, is the paramount message in this tragic case, and not the programming error itself. Reference. Vicente KJ, Kada-Bekhaled K, Hillel G, Cassano A, Orser BA. Programming errors contribute to death from patient-controlled analgesia: case report and estimate of probability. Can J Anesth 2003; 50: 328–32.")
68
D. John Doyle, MD PhD Programming errors from patient-controlled analgesia
Canadian Journal of Anesthesia 50: (2003)
")
69
Fentanyl Lolipop

70
Fentanyl Patch

72
Iontophoresis

73
CO2 Response Curve Normal PCO2 maintained at 40 mmHg
If PCO2 incrementally increases (e.g., from increased CO2 production due to increased metabolic rate), alveolar ventilation will increase to blunt the rise in PCO2 If PCO2 incrementally decreases (e.g., from decreased CO2 production due to decreased metabolic rate), alveolar ventilation will decrease to blunt the drop in PCO2
, alveolar ventilation will increase to blunt the rise in PCO2. If PCO2 incrementally decreases (e.g., from decreased CO2 production due to decreased metabolic rate), alveolar ventilation will decrease to blunt the drop in PCO2.")
74
Anesthesiology: Volume 99(4) October 2003 pp 767-770
Curve A represents the normal carbon dioxide response of an awake individual; the hockey stick appearance at low values of Paco2 corresponds to the observation that following hyperventilation, awake individuals do not become apneic but rather show a modest decrease in VE until Paco2 returns to its resting value. Curve B represents the carbon dioxide response curve following administration of a sedative or anesthetic medication, which decreases its slope by 50%. Note that the curve no longer has a hockey stick shape but rather falls linearly to a VE of 0 (the apneic threshold). Once apnea develops, the Pco2 must increase to approximately the resting value before ventilation restarts, accounting for the hysteresis loop (line B). Curve C represents the carbon dioxide excretion hyperbola, which depends on the principle of conservation of mass: Assuming constant carbon dioxide production, increasing VE will decrease Paco2, whereas decreasing VE tends to increase Paco2. In the awake state, point X (the intersection of carbon dioxide response curve A with carbon dioxide excretion hyperbola C) defines the resting Paco2 and VE, whereas point Y represents the values of Paco2 and VE during sedation or anesthesia.
. Once apnea develops, the Pco2 must increase to approximately the resting value before ventilation restarts, accounting for the hysteresis loop (line B). Curve C represents the carbon dioxide excretion hyperbola, which depends on the principle of conservation of mass: Assuming constant carbon dioxide production, increasing VE will decrease Paco2, whereas decreasing VE tends to increase Paco2. In the awake state, point X (the intersection of carbon dioxide response curve A with carbon dioxide excretion hyperbola C) defines the resting Paco2 and VE, whereas point Y represents the values of Paco2 and VE during sedation or anesthesia.")
75
Opiates and the search for artificial bliss

76
"If we could sniff or swallow something that would, for five or six hours each day, abolish our solitude as individuals, atone us with our fellows in a glowing exaltation of affection and make life in all its aspects seem not only worth living, but divinely beautiful and significant, and if this heavenly, world-transfiguring drug were of such a kind that we could wake up next morning with a clear head and an undamaged constitution - then, it seems to me, all our problems (and not merely the one small problem of discovering a novel pleasure) would be wholly solved and earth would become paradise." ALDOUS HUXLEY

77
"If it was possible to become free of negative emotions by a riskless implementation of an electrode - without impairing intelligence and the critical mind - I would be the first patient." Dalai Lama (Society for Neuroscience Congress, Nov. 2005)
")
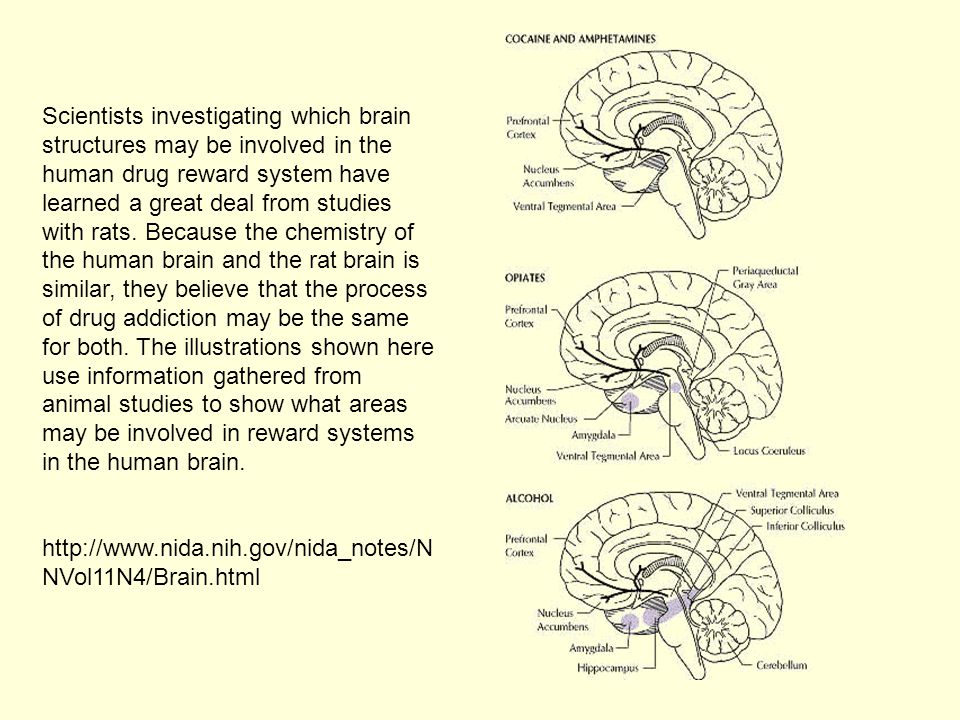
78
Scientists investigating which brain structures may be involved in the human drug reward system have learned a great deal from studies with rats. Because the chemistry of the human brain and the rat brain is similar, they believe that the process of drug addiction may be the same for both. The illustrations shown here use information gathered from animal studies to show what areas may be involved in reward systems in the human brain.
79
Nucleus Accumbens "At a purely chemical level, every experience humans find enjoyable - whether listening to music, embracing a lover, or savoring chocolate - amounts to little more than an explosion of dopamine in the nucleus accumbens as exhilarating and ephemeral as a firecracker." J Madelaine Nash

80
Clinical Study for Alleviating Opiate Drug Psychological Dependence by a Method of Ablating the Nucleus Accumbens with Stereotactic Surgery Stereotact Funct Neurosurg. 2003;81(1-4): ABSTRACT The aim of this study was to explore a new way of treating drug addiction by ablating the nucleus accumbens (NA(C)), which has a close relationship with drug-induced psychological dependence, using stereotactic surgery, blocking the mesocorticolimbic dopamine circuit, alleviating craving for drugs and lowering the relapse rate after detoxification. On the basis of animal experiments, stereotactic surgery was performed in 28 patients by making a lesion in the NA(C) bilaterally to treat opiate drug dependence. Indications, the criterion of therapeutic effect, treatment process and the therapeutic and safety evaluation index of the surgery were formulated particularly. The mean follow-up period was 15 months. Relapse has not occurred in 11 cases up till now. Drug-free time in these patients has been more than half a year in 4 cases (more than a year in 3 cases), and less than half a year in 7 cases. Relapse occurred in 15 cases after surgery. Drug-free time in these patients was more than half a year in 3 cases, between 1 month and half a year in 10 cases and less than 1 month in 2 cases. The therapeutic effect was excellent in 7 cases (26.9%), good in 10 cases (38.5%) and poor in 2 cases (7.7%). Another 7 cases were still under investigation at the time of writing. Relapse rates after surgery were 7.7, 38.5 and 57.5% within 1 month, between 1 month and half a year and after more than half a year, respectively. There were no common complications of surgery such as intracranial hematoma or infection in these patients after operation. Character type was changed slightly in 2 cases, and 4 cases suffered temporary memory loss, which did not affect their daily lives and learning function. They all recovered within 1 month. There were different degrees of effectiveness of treating drug addicts' psychological dependence by making lesions in the NA(C) bilaterally with stereotactic surgery. No particular complications occurred. The operation is safe and feasible. The mean follow-up time in this study was 15 months. The effectiveness was satisfactory. The relapse rate of drug addicts after detoxification was clearly reduced.
: ABSTRACT. The aim of this study was to explore a new way of treating drug addiction by ablating the nucleus accumbens (NA(C)), which has a close relationship with drug-induced psychological dependence, using stereotactic surgery, blocking the mesocorticolimbic dopamine circuit, alleviating craving for drugs and lowering the relapse rate after detoxification. On the basis of animal experiments, stereotactic surgery was performed in 28 patients by making a lesion in the NA(C) bilaterally to treat opiate drug dependence. Indications, the criterion of therapeutic effect, treatment process and the therapeutic and safety evaluation index of the surgery were formulated particularly. The mean follow-up period was 15 months. Relapse has not occurred in 11 cases up till now. Drug-free time in these patients has been more than half a year in 4 cases (more than a year in 3 cases), and less than half a year in 7 cases. Relapse occurred in 15 cases after surgery. Drug-free time in these patients was more than half a year in 3 cases, between 1 month and half a year in 10 cases and less than 1 month in 2 cases. The therapeutic effect was excellent in 7 cases (26.9%), good in 10 cases (38.5%) and poor in 2 cases (7.7%). Another 7 cases were still under investigation at the time of writing. Relapse rates after surgery were 7.7, 38.5 and 57.5% within 1 month, between 1 month and half a year and after more than half a year, respectively. There were no common complications of surgery such as intracranial hematoma or infection in these patients after operation. Character type was changed slightly in 2 cases, and 4 cases suffered temporary memory loss, which did not affect their daily lives and learning function. They all recovered within 1 month. There were different degrees of effectiveness of treating drug addicts psychological dependence by making lesions in the NA(C) bilaterally with stereotactic surgery. No particular complications occurred. The operation is safe and feasible. The mean follow-up time in this study was 15 months. The effectiveness was satisfactory. The relapse rate of drug addicts after detoxification was clearly reduced.")
81
Case Study: Boy with Congenital Absence of Pain
Accornero N, Berardelli A, Medolago L. Congenital absence of pain.Manfredi M, Bini G, Cruccu G, Arch Neurol Aug;38(8): A 16-year-old boy had congenital absence of pain sensitivity and no impairment of other sensory modalities. Routine electrophysiologic investigation showed no abnormalities. The threshold and latency of electrically elicited corneal reflex and cortical potentials evoked by tooth pulp stimulation were normal, but suprathreshold electric stimulation of corneal mucosa and dental pulp, as well as electric stimulation of dorsal roots, did not elicit pain. The total CSF opioid activity was raised. However, naloxone hydrochloride administration failed to reverse the analgesia. The axon reflex to intradermal injection of histamine dihydrochloride was absent. Cutaneous nerve branches showed unspecific changes affecting part of unmyelinated axons. Most of the unmyelinated as well as the myelinated axons were normal. We consider the case an example of congenital indifference to pain.
: A 16-year-old boy had congenital absence of pain sensitivity and no impairment of other sensory modalities. Routine electrophysiologic investigation showed no abnormalities. The threshold and latency of electrically elicited corneal reflex and cortical potentials evoked by tooth pulp stimulation were normal, but suprathreshold electric stimulation of corneal mucosa and dental pulp, as well as electric stimulation of dorsal roots, did not elicit pain. The total CSF opioid activity was raised. However, naloxone hydrochloride administration failed to reverse the analgesia. The axon reflex to intradermal injection of histamine dihydrochloride was absent. Cutaneous nerve branches showed unspecific changes affecting part of unmyelinated axons. Most of the unmyelinated as well as the myelinated axons were normal. We consider the case an example of congenital indifference to pain.")
82
Case Study: Boy with Congenital Absence of Pain
Question: What was the underlying genetic mutation? Question: What protein was not correctly produced as a result? Question: How is this protein involved in the transduction of pain?

83
Readings [Review] [The Brain's Drug Reward Systems ] [Terminal Sedation]
![Readings [Review]](http://slideplayer.com/slide/1679342/7/images/83/Readings+++%5BReview%5D.jpg "[The Brain s Drug Reward Systems ] [Terminal Sedation]")
84
The End

Similar presentations



















 Medical University of Sofia, Faculty of Medicine Department of Pharmacology and Toxicology.>")
 Analgesics and Antagonists.>")





