Download presentation
Presentation is loading. Please wait.

1
CRRT: It’s Not Just for Renal Failure Anymore
Presented by: Sue Fallone,MS,RN,CNN Clinical Nurse Specialist Adult and Pediatric Dialysis Albany Medical Center

2
Objectives Define Heart Failure Define Sepsis
Discuss medical management of heart failure and sepsis Describe indications for CRRT for these disorders Case Study

3
HEART FAILURE Clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood

4
Incidence of Heart Failure
More deaths from heart failure than from all forms of cancer Nearly 1 millions people are admitted to the hospital with CHF and 30%-60% are readmitted Contributed to 53,000 deaths in the U.S. each year About 550,000 new cases per year Affects men and women equally Related to the aging population, lower death rate from MI, and improved treatment for heart disease

5
Causes of Heart Failure
Main causes Ischemic heart disease, Cardiomyopathy, Hypertension, Diabetes Other causes: Valvular heart disease, Congenital heart disease, Alcohol and drugs, Hyperdynamic circulation (anemia, thyrotoxicosis, hemochromatosis, Paget's disease), Right heart failure (RV infarct, pulmonary hypertension, pulmonary embolism, cor pulmonale (COPD)), Arrhythmia and Pericardial disease.
, Right heart failure (RV infarct, pulmonary. hypertension, pulmonary embolism, cor pulmonale. (COPD)), Arrhythmia and Pericardial disease.")
6
Mechanisms Leading to Heart Failure
Impaired cardiac contractility as in myocardial infarction and cardiomyopathy Ventricular outflow obstruction (pressure overload) as in hypertension and aortic stenosis Impaired ventricular fillings as in mitral stenosis and constrictive pericarditis Volume overload as in mitral regurgitation
 as in hypertension and aortic stenosis. Impaired ventricular fillings as in mitral stenosis and constrictive pericarditis. Volume overload as in mitral regurgitation.")
7
Precipitating Factors
Infections Arrhythmias Physical, Dietary, Fluid, Environmental, and Emotional Excesses. Myocardial infarction Pulmonary embolism Anemia Thyrotoxicosis and pregnancy Aggravation of hypertension Rheumatic, Viral, and Other Forms of Myocarditis Infective endocarditis Diabetes

8
2. Sympathetic activity:
Cardiac remodeling: Hypertrophy & Dilatation C.O.P 2. Sympathetic activity: H.R. V.C E.D.V After-load Pre-load. Angiotensin Na+ & water retention Aldosterone

9
TYPES OF HEART FAILURE Left- sided or left ventricular (LV) heart failure is commonly caused by ischemic heart disease but can also occur with valvular heart disease and hypertension. 2 types of (LV) heart failure diastolic failure is a syndrome consisting of symptoms and signs of heart failure with preserved left ventricular ejection fraction above 45–50% and abnormal left ventricular relaxation assessed by echocardiography systolic failure is when the left ventricle loses it’s ability to contract normally, can pump enough blood into the systemic circulation Right-sided or right ventricular (RV)heart failure may be secondary to chronic( LV ) heart failure but can occur with primary and secondary pulmonary hypertension, right ventricular infarction.
 heart failure. diastolic failure is a syndrome consisting of symptoms and signs of heart failure with preserved left ventricular ejection fraction above 45–50% and abnormal left ventricular relaxation assessed by echocardiography. systolic failure is when the left ventricle loses it’s ability to contract normally, can pump enough blood into the systemic circulation. Right-sided or right ventricular (RV)heart failure. may be secondary to chronic( LV ) heart failure but can occur with primary and secondary pulmonary hypertension, right ventricular infarction.")
10
TYPES of HEART FAILURE Congestive Heart Failure-
Blood flow out of the heart slows, blood returning to the heart through the veins backs up and congestion in the body’s tissues Will see edema, SOB, can affect kidney function

11
Symptoms & Signs OF Heart Failure
Left heart failure Symptoms are predominantly fatigue, exertional dyspnea, orthopnea and PND Physical signs: Cardiomegaly, gallop functional mitral regurgitation and crackles a the lung bases.

12
Right Heart Failure Symptoms (fatigue, breathlessness, anorexia and nausea) relate to distension and fluid accumulation in areas drained by the systemic veins. Physical signs are usually more prominent than the symptoms, with: jugular venous distension tender smooth hepatic enlargement dependent pitting edema development of free abdominal fluid (ascites) Pleural effusion (commonly right-sided). Dilatation of the right ventricle produces cardiomegaly and may give rise to functional tricuspid regurgitation. Tachycardia and a right ventricular third heart sound are usual.
 relate to distension and fluid accumulation in areas drained by the systemic veins. Physical signs are usually more prominent than the symptoms, with: jugular venous distension. tender smooth hepatic enlargement. dependent pitting edema. development of free abdominal fluid (ascites) Pleural effusion (commonly right-sided). Dilatation of the right ventricle produces cardiomegaly and may give rise to functional tricuspid regurgitation. Tachycardia and a right ventricular third heart sound are usual.")
13
Major symptoms & signs of heart failure

14
Classification of Heart Failure Functional Capacity
Class I – patients with cardiac disease and no limitation of physical activity Class II- patients with cardiac disease slight limitation of physical activity results in fatigue, palpitation, dyspnea or angina Class III-patients with cardiac disease marked limitation of physical activity comfortable at rest Class IV-patients with cardiac disease inability to carry on any physical activity, symptoms of heart failure at rest

15
Treatment of heart failure 2. Sympathetic activity:
C.O.P Positive Inotropics 2. Sympathetic activity: Hypertrophy & Dilatation H.R. V.C Pre-load. E.D.V After-load vasodilators Angiotensin ACE inhibitors Diuretics Na+ & water retention Aldosterone

17
If Resistant to Diuretics
MAY NEED Ultrafiltration

18
UNLOAD STUDY The UNLOAD study was a randomized, multicenter study of 200 patients involving 28 hospitals and medical centers across the United States. UNLOAD compared the short and long-term safety and efficacy of an advanced form of ultrafiltration therapy(Aquapheresis) to the use of conventional diuretic drug therapy in fluid overloaded heart failure patients. The UNLOAD study was published in the February 13, issue of Journal of American College of Cardiology. (Costanzo MR et al. JACC 2007; 49(6): ).
 to the use of conventional diuretic drug therapy in fluid overloaded heart failure patients. The UNLOAD study was published in the February 13, 2007 issue of Journal of American College of Cardiology. (Costanzo MR et al. JACC 2007; 49(6): ).")
19
UNLOAD Study Results 28% with greater fluid loss with UF
43% reduction in patients being re-hospitalization for HF 63% fewer hospital days for HF

20
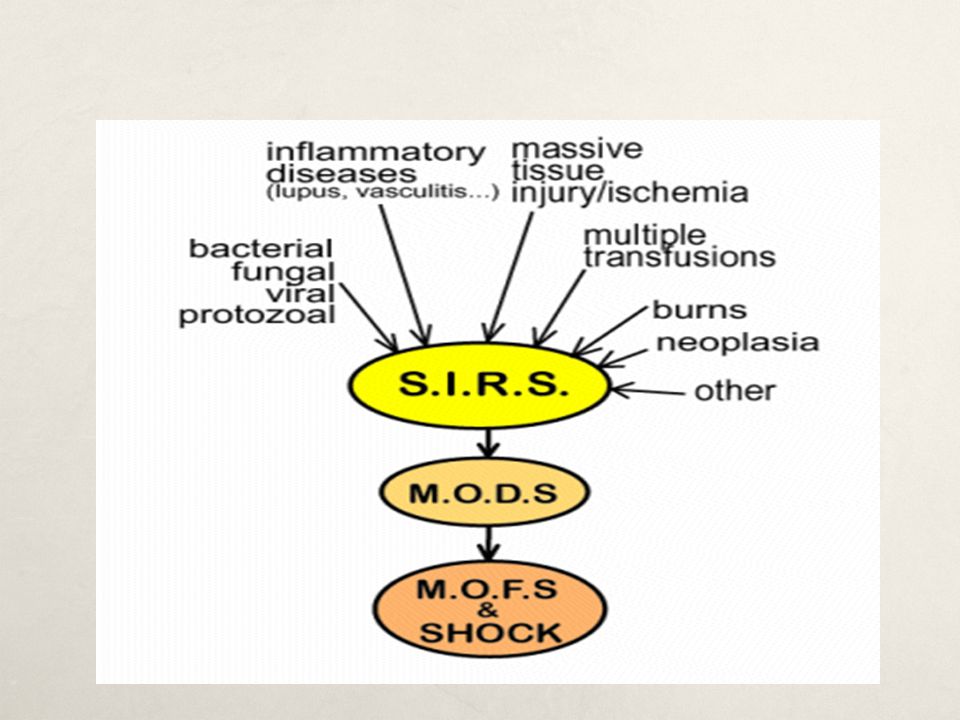
What is SIRS? The systemic inflammatory response syndrome is systemic level of acute inflammation, that may or may not be due to infection, and is generally manifested as a combination of vital sign abnormalities including fever or hypothermia, tachycardia, and tachypnea.

21
Definitions Severe SIRS – SIRS in which at least 1 major organ system has failed. Sepsis – SIRS which is secondary to infection. Severe Sepsis – Severe SIRS which is secondary to infection. Septic Shock – Severe sepsis resulting in hypotensive cardiovascular failure.

22
Systemic Inflammatory Reponse(SIRS)
Can be triggered by infectious and non-infectious events Infectious causes bacteria or fungi Non infectious causes are prancreatitis,burns, trauma SIRS is the term used for noninfectious causes

23
Criteria for SIRS Requires 2 of the following 4 features to be present: Temp >38.3° or <36.0° C Tachypnea (RR>20 or MV>10L) Tachycardia (HR>90, in the absence of intrinsic heart disease) WBC > 10,000/mm3 or <4,000/mm3 or >10% band forms on differential
 WBC > 10,000/mm3 or <4,000/mm3 or. >10% band forms on differential.")
24
Criteria for Severe SIRS
Must meet criteria for SIRS, plus 1 of the following: Altered mental status SBP<90mmHg or fall of >40mmHg from baseline Impaired gas exchange Metabolic acidosis (pH<7.30 & lactate > 1.5 x upper limit of normal) Oliguria (<0.5mL/kg/hr) or renal failure Hyperbilirubinemia Coagulopathy (platelets < 80, ,000/mm3, INR >2.0, PTT >1.5 x control, or elevated fibrin degredation products)
 Oliguria (<0.5mL/kg/hr) or renal failure. Hyperbilirubinemia. Coagulopathy (platelets < 80, ,000/mm3, INR >2.0, PTT >1.5 x control, or elevated fibrin degredation products)")
25
Pathophysiology of Sepsis
Overwhelming inflammatory response Increased production of proimflamatory cytokines and decreased production of cytokines( which inhibit inflammation) Clotting cascade activated Peripheral Vasodilatation systemic vascular resistance
 Clotting cascade activated. Peripheral Vasodilatation systemic vascular resistance.")
26
Pathophysiology of Sepsis continued
C/O decreases Intravascular fluid loss Decreased pre load-hypotension ATN-renal hypoperfusion and ischemic injury MODS MOF

28
Relationship Between SIRS and Sepsis
Adapted from: Marini JJ, et al. Critical Care Medicine, 2nd ed

32
Risk Factors for SIRS/Sepsis
Age Indwelling lines/catheters Immunocompromised states Malnutrition Alcoholism Malignancy Diabetes Cirrhosis Male sex Genetic predisposition?

33
Prognosis Overall mortality from SIRS/sepsis in the U.S. is approximately 20%. Mortality is roughly linearly related to the number of organ failures, with each additional organ failure raising the mortality rate by 15%. Hypothermia is one of the worst prognostic signs. Patients presenting with SIRS and hypothermia have an overall mortality of ~80%.

34
Treatment Fluid Resuscitation Vasopressors Antibiotics
Eradication of infection Ventilatory support, activated protein C, steroids, glycemic control, nutrition CRRT

35
CONTINUOUS RENAL REPLACMENT THERAPY
Helen

36
CRRT Definition CRRT = Continuous Renal Replacement Therapy Defined as
“Any extracorporeal blood purification therapy intended to substitute for impaired renal function over an extended period of time and applied for or aimed at being applied for 24 hours /day.” * * Bellomo R., Ronco C., Mehta R, Nomenclature for Continuous Renal Replacement Therapies, AJKD, Vol 28, No. 5, Suppl 3, November 1996 CRRT is the blanket term which encompasses all continuous therapies. It has been defined as ……read the slide. Make sure to note the proof source.

37
Introduction to CRRT Why continuous therapies?
Continuous therapies closely mimic the native kidney in treating ARF and fluid overload Slow & gentle Remove fluid and waste products over time Tolerated well by the hemodynamically unstable patient The continuous therapies provide a slow, gentle treatment of ARF and fluid overload very much like the native kidney. CRRT is generally well tolerated by critically ill, hemodynamically unstable patients. Moreover, control of azotemia, acid-base balance and fluid volume can easily be achieved with CRRT.

38
Circulating Blood Volume
Three Compartment Model 2 Intra-cellular Space Extra-cellular Space Intra-Vascular Space Circulating Blood Volume Toxins Fluid Dialyzer 23 L 17 L 40 Liters 5 Liters

39
Indications for Therapy
Acute kidney injury- preferred in the critically ill patient Fluid overload- can removed large amounts of fluid slowly Hemodynamically unstable- continuous therapy allow for slow hourly fluid removal which allows the intravascular spaces to refill

40
Indications continued
Highly catabolic patients who need increased clearance rates Patients needing large molecular weight substances removed Sepsis

41
Molecular Weight SMALL MOLECULES- 0-500 daltons (urea, creatinine)
MIDDLE MOLECULES daltons ( vitamin B12) LARGE MOLECULES ,000 daltons ( heparin, Beta 2 drugs)
 LARGE MOLECULES ,000 daltons ( heparin, Beta 2 drugs)")
42
CRRT Modalities SCUF OR ULTRAFILTRATION - Slow Continuous UltraFiltration CVVHD - Continuous Veno-Venous HemoDialysis CVVH - Continuous Veno-Venous Hemofiltration CVVHDF – Continuous Veno-Venous Hemodiafiltration CRRT acronyms...read slide...

43
SCUF/Ultrafiltration
Primary therapeutic goal: Safe management of fluid removal Patient UF rate ranges up to 2 L/Hr No dialysate;No replacement fluids No molecule removal Large fluid removal via ultrafiltration Blood Flow rates = ml/min SCUF…read the slide. Note that when using this therapy, significant amounts of fluid are removed from the patient. No dialysate or replacement fluid are used to increase solute removal. Ultrafiltration can be adjusted to cause dramatic fluid shifts. This therapy is best suited to severely hypervolemic patients (i.e. post OHS, post resuscitation, etc.) and is not generally employed for lengthy periods of time. It is not uncommon to remove fluid from the patient over a short (8-12 hr.) time period and then to D/C the treatment.
 and is not generally employed for lengthy periods of time. It is not uncommon to remove fluid from the patient over a short (8-12 hr.) time period and then to D/C the treatment.")
44
Slow Continuous UltraFiltration SCUF/ULTRAFILTRATION Access Return
Effluent SCUF/ULTRAFILTRATION Slow Continuous UltraFiltration As this slide shows, the circuit for SCUF is a simple one. Blood enters the extracorporeal circuit through an access line, passes through the hemofilter, and returns to the patient circulation via the return line. As the blood passes through the filter, ultrafiltration takes place and effluent goes down the effluent waste line. Pumps control blood flow and fluid removal rates.

45
Ultrafiltration Particles move through a semi-permeable membrane by use of HYDROSTATIC pressure. The separation of particles from a suspension by passage through a filter. The separation is accomplished by convective transport.

46
Convection – Step 1 Filter Action
Red Cell Na K Na Na Na H2O H2O U H2O Na U Na Na U Red Cell H2O K H2O H2O K H2O Red Cell U U Na Na U Red Cell H2O Na Na Na K Na U K H2O H2O K U H2O K H2O U Na Na Na H2O On the left represents the filter with blood coming from the patient through the red tubes and yello represent the plasma water being filtered out of the patient. The figure on the right represents one of the red tubes and the action with the filter. Note the blood concentration of solutes (electrolytes) within the inner portion (blood) of the filter and concentration of solutes (electrolytes). With convection the plasma water is shifted from the patient to the outside of the filter, during this action the solutes (electrolytes) are dragged along with the plasma water. Of note: with convection, there’s a large amount of plasma water shifted or removed. See the next slide. U Na K K H2O Red Cell U Na K H2O Na Na U K
 within the inner portion (blood) of the filter and concentration of solutes (electrolytes). With convection the plasma water is shifted from the patient to the outside of the filter, during this action the solutes (electrolytes) are dragged along with the plasma water. Of note: with convection, there’s a large amount of plasma water shifted or removed. See the next slide. U. Na. K. K. H2O. Red Cell. U. Na. K. H2O. Na. Na. U. K.")
47
Solute Removal by Convection
To illustrate convection, we go back to the use of the cups. The cup now has a concentrated solution on one side of the semipermeable membrane. As fluid moves (by ultrafiltration), solutes small enough to pass through the pores of the membrane move along with the fluid. Change in blood concentration of a specific solute is dependent on the fluid volume removed. Convection: The movement of solutes with a water-flow, “solvent drag”, e.g... the movement of membrane-permeable solutes with water across the semipermeable membrane
, solutes small enough to pass through the pores of the membrane move along with the fluid. Change in blood concentration of a specific solute is dependent on the fluid volume removed. Convection: The movement of solutes with a water-flow, solvent drag , e.g... the movement of membrane-permeable solutes with water across the semipermeable membrane.")
48
Continuous Veno-Venous Hemofiltration
Replacement (pre or post dilution) Access Return Effluent CVVH Continuous Veno-Venous Hemofiltration This schematic represents a CVVH circuit. As I stated earlier, note that the replacement fluids (indicated by the dotted lines) can be delivered either pre or post filter. In the past replacement fluids were used to control patient’s fluid volume. No equipment was available to provide precise volume control and it was the nurse’s responsibility to calculate total patient intake and output every hour and compare that to the MD’s prescription. Invariably the doctor’s prescribed fluid removal and the actual volume removed were not equal, requiring either the addition of fluid to the patient or trying not to increase fluid removal for the next hour. More often than not, “catch up” was played and this volume infused was referred to as the replacement fluid. With the advent of precise control systems, integrated pumps are used to take the mystery out of fluid management. Solute removal is accomplished by convection. Note that the effluent waste line not only contains UF from the patient, but also the replacement fluid volume.
 Access. Return. Effluent. CVVH. Continuous Veno-Venous Hemofiltration. This schematic represents a CVVH circuit. As I stated earlier, note that the replacement fluids (indicated by the dotted lines) can be delivered either pre or post filter. In the past replacement fluids were used to control patient’s fluid volume. No equipment was available to provide precise volume control and it was the nurse’s responsibility to calculate total patient intake and output every hour and compare that to the MD’s prescription. Invariably the doctor’s prescribed fluid removal and the actual volume removed were not equal, requiring either the addition of fluid to the patient or trying not to increase fluid removal for the next hour. More often than not, catch up was played and this volume infused was referred to as the replacement fluid. With the advent of precise control systems, integrated pumps are used to take the mystery out of fluid management. Solute removal is accomplished by convection. Note that the effluent waste line not only contains UF from the patient, but also the replacement fluid volume.")
49
Molecular Transport Mechanisms
Convection - The movement of solutes with a water-flow, “solvent drag”, the movement of membrane-permeable solutes with water across the semipermeable membrane There are a number of key scientific principles used to accomplish the goals of CRRT. They are listed here and before we discuss the individual therapies, I would like to review them. Understanding the principles of diffusion, ultrafiltration and convection will clarify which therapy will best produce the desired outcome whether used alone or in combination.

50
Convection – Step 1 Filter Action
Red Cell Na K Na Na Na H2O H2O U H2O Na U Na Na U Red Cell H2O K H2O H2O K H2O Red Cell U U Na Na U Red Cell H2O Na Na Na K Na U K H2O H2O K U H2O K H2O U Na Na Na H2O On the left represents the filter with blood coming from the patient through the red tubes and yello represent the plasma water being filtered out of the patient. The figure on the right represents one of the red tubes and the action with the filter. Note the blood concentration of solutes (electrolytes) within the inner portion (blood) of the filter and concentration of solutes (electrolytes). With convection the plasma water is shifted from the patient to the outside of the filter, during this action the solutes (electrolytes) are dragged along with the plasma water. Of note: with convection, there’s a large amount of plasma water shifted or removed. See the next slide. U Na K K H2O Red Cell U Na K H2O Na Na U K
 within the inner portion (blood) of the filter and concentration of solutes (electrolytes). With convection the plasma water is shifted from the patient to the outside of the filter, during this action the solutes (electrolytes) are dragged along with the plasma water. Of note: with convection, there’s a large amount of plasma water shifted or removed. See the next slide. U. Na. K. K. H2O. Red Cell. U. Na. K. H2O. Na. Na. U. K.")
51
Solute Removal by Convection
To illustrate convection, we go back to the use of the cups. The cup now has a concentrated solution on one side of the semipermeable membrane. As fluid moves (by ultrafiltration), solutes small enough to pass through the pores of the membrane move along with the fluid. Change in blood concentration of a specific solute is dependent on the fluid volume removed. Convection: The movement of solutes with a water-flow, “solvent drag”, e.g... the movement of membrane-permeable solutes with water across the semipermeable membrane
, solutes small enough to pass through the pores of the membrane move along with the fluid. Change in blood concentration of a specific solute is dependent on the fluid volume removed. Convection: The movement of solutes with a water-flow, solvent drag , e.g... the movement of membrane-permeable solutes with water across the semipermeable membrane.")
52
CVVHD - Continuous VV Hemodialysis
Primary therapeutic goal: Solute removal by diffusion Safe fluid volume management by ultrafiltration Requires Dialysate solution Patient UF rate ranges 2-7 L/24 hours (~300 ml/hr) Dialysate Flow rate = ml/min (~2 L/hr) Blood Flow rate = ml/min No replacement solution Solute removal determined by Dialysate Flow rate. The next therapy for discussion is CVVHD - continuous veno-venous hemodialysis. This therapy uses a dialysate on the fluid side of the filter to increase solute exchange by diffusion. Replacement fluid is not administered with this therapy. Dialysate is infused at ml/min (1-3 L/ hour). The blood flow rate is maintained between ml/min. This compares to intermittent HD that uses typical blood flow rates of ml/min and dialysate flow rates of ml/min.
 Dialysate Flow rate = ml/min (~2 L/hr) Blood Flow rate = ml/min. No replacement solution. Solute removal determined by Dialysate Flow rate. The next therapy for discussion is CVVHD - continuous veno-venous hemodialysis. This therapy uses a dialysate on the fluid side of the filter to increase solute exchange by diffusion. Replacement fluid is not administered with this therapy. Dialysate is infused at ml/min (1-3 L/ hour). The blood flow rate is maintained between ml/min. This compares to intermittent HD that uses typical blood flow rates of ml/min and dialysate flow rates of ml/min.")
53
Diffusion – Filter Action
Na Na K Mg Mg Na H2O U Na Na Na Na U H2O H2O U Na Na K K U Na Mg H2O K H2O Na U Na U H2O K U H2O K H2O H2O U Na Na Mg On the left represents the filter with blood coming from the patient through the red tubes with the dialysate being infused to the outer portion of the filter in the opposite direction. The figure on the right represents one of the red tubes and the action with the filter. Note the blood concentration of solutes (electrolytes) within the inner portion (blood) of the filter and concentration of solutes (electrolytes). With diffusion the solutes will move from a high concentration to a low concentration until there’s equilibrium; the dialysate controls the amount of movement of solutes. Of note: with diffusion, minimal plasma water is shifted or removed. U Na U K H2O Na H2O U Na H2O Na K U K Na Na Mg K
 within the inner portion (blood) of the filter and concentration of solutes (electrolytes). With diffusion the solutes will move from a high concentration to a low concentration until there’s equilibrium; the dialysate controls the amount of movement of solutes. Of note: with diffusion, minimal plasma water is shifted or removed. U. Na. U. K. H2O. Na. H2O. U. Na. H2O. Na. K. U. K. Na. Na. Mg. K.")
54
Vascular Access Depending on the device used lumen size matters
If using AquaDex FlexFlow Fluid Removal System midline catheters can be used If using CRRT devices hemodialysis type catheters need to be placed.

55
Catheter Size Adults Children (weight based) 12.5 to 14 french
Length will vary 16,19,24,cm Femoral placement least preferred Children (weight based) 5 french single catheter 7 fr dual lumen 8 fr dual lumen 10 fr dual lumen 11 fr dual lumen Length 9 cm, 10 cm, 12 cm, 15 cm
 5 french single catheter 7 fr dual lumen. 8 fr dual lumen. 10 fr dual lumen. 11 fr dual lumen. Length. 9 cm, 10 cm, 12 cm, 15 cm.")
57
Case Study #1 Mr. G is a 60 year old man with CAD s/p MI and PTCA to LAD in 1997, dyslipidemia, and tobacco use who called 911 for severe chest pain on 11/01/10. This pain was similar in nature to his previous MI.

58
ECG in the ambulance

59
History In the ambulance en route to the emergency room, the patient developed two episodes of ventricular fibrillation which both successfully responded to DC cardioversion. After arrival to the cath lab, the patient developed cardiogenic shock and recurrent ventricular fibrillation requiring multiple shocks (he was shocked 11 times in the cath lab prior to intervention) and intubation with mechanical ventilation.
 and intubation with mechanical ventilation.")
60
Cath Lab Course Coronary angiography showed:
Totally occluded mid LAD with thrombus Mild diffuse atherosclerosis of left circumflex and right coronary arteries Soon after the first injection there was proximal propagation of the LAD thrombus which occluded the left main coronary artery A wire was passed to the distal LAD and an AngioJet thrombectomy device was used which re-established flow

61
Cath Lab Course After the Impella device was placed, the patient had no further episodes of ventricular fibrillation

62
Immediately Post Cath Patient admitted to the CCU on IV Epinephrine, Dobutamine, and Dopamine continuous infusions Echocardiogram the next day showed severe anterior wall hypokinesis with EF 25% The patient was placed on CVVH then on SCUF to remove excess fluid

63
Hospital Course Hospital day 3: Impella device was removed
Hospital Day 6: Repeat echocardiogram, EF 50-55% Hospital Day 8: Extubated, neurologically intact Hospital Day 16: Discharged to home

64
Case Study #2 Alan is a 20 year old admitted to a cardiology unit with CHF and Situs Inversus. He had SOB , anascara, arrythmias. His blood pressure was 110/60 mm Hg. He has a serum creatinine of 1.5 mg/dl. He is in need of a pacemaker but first needs 10 liters of fluid removed before placement of a pacemaker. He is started on furosemide 80 mg every 8 hours and metolazone 10mg/d for 2 days. On day three he is given mannitol 25 g every eight hours. He is putting out 3L of urine a day but has only decreased his net fluid loss by 3 L due to lack of adherance to his fluid restriciton

65
Case Study Continued Because of his need for a pacemaker, the decision was made to place the patient on SCUF. After three days of therapy the patient was at his dry weight and stable and was able to receive his pacemaker Consideration has to be given related to rate of fluid removal and his overall renal function Patient was discharged to home with a follow up to a nephrologist

66
Case Study #3 Mrs. D was admitted to MICU for sepsis. She had been hypotensive that required vasopressors. During the course of her stay in MICU, she developed AKI. To manage her fluid and electrolytes, she was started on CRRT. She seemed to tolerate CRRT well. On her 5th day of therapy, her Serum Creatinine was down to 1.2 from 6.9 and her electrolytes were stable, her BP was borderline with MAP > 60 mmHg and < 70 mmHg. CRRT was discontinued and only to be restarted after 2 days when the patient became hypotensive again that regular HD was not possible given her hemodynamic parameters. Patient was started on phenylephrine at 200 mcg/min and nor- epinephrine at 10 mcg/min. On the 3rd day of the 2nd therapy, the patient had the following data:

67
Patient Data Time BP CVP I and O Balance 2/15 2200 125/60 14 Off -100
Vasopressor I and O Balance 2/ 125/60 14 Off -100 2/ 110/65 12 -250 2/ 73/85 6 ON -1100 2/ 108/55 10 -500

68
Questions What happened in this scenario?
What should have been considered in setting the net fluid removal rate? How would we assess for the intravascular vs extra-vascular fluid status? When will be the right time to advocate for discontinuance of CRRT?

69
CRRT IS NOT JUST FOR RENAL FAILURE
Conclusion CRRT therapies can be applied to many clinical situations The patient goals/outcomes can be enhanced with early initiation of this therapy CRRT IS NOT JUST FOR RENAL FAILURE

70
THANK YOU

Similar presentations









>")






 Department of Clinical Pharmacy Salman Bin AbdulAziz University College Of Pharmacy.>")






 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")
