Download presentation
Presentation is loading. Please wait.

1
COLLABORATION IN CARDIOVASCULAR INTERVENTIONS: A NON-ZERO SOLUTION
Mark J. Russo, MD, MS Assistant Professor of Surgery Co-Director, Center for Aortic Diseases

2
ASSERTIONS Traditional barriers between medical specialties result in a provider-centric rather than a patient-centric healthcare system These barriers are not compatible with the effective application of today’s hybrid technologies Elimination of these barriers improves patient outcomes (win) and offers a non-zero opportunity for providers (win-win) -> WIN-WIN-WIN
 and offers a non-zero opportunity for providers (win-win) -> WIN-WIN-WIN.")
3
Traditional barriers between medical specialties result in a provider-centric rather than a patient-centric healthcare system

4
DISCONNECT BETWEEN PRESENTATION AND ORGANIZATION
Patients present with Conditions-Disease Process Providers organized by Specialties-Skills/Knowledge Coronary Artery Disease Valve Disease Heart Failure Aortic Disease Peripheral Vascular Disease Cardiology Interventional Cardiology Cardiac Surgery Vascular Surgery Radiology

5
CARE IS DECENTRALIZED Interventional Cardiology General Cardiology
Treatment Surgery

6
CARE IS DECENTRALIZED Patients are forced to seek care sequentially from various subspecialites (eg multiple appts) Interventional Cardiology General Cardiology Treatment Surgery

7
CARE IS DECENTRALIZED Patients are forced to seek care sequentially from various subspecialites (eg multiple appts) Interventional Cardiology General Cardiology Treatment Surgery

8
CARE IS DECENTRALIZED Patients are forced to seek care sequentially from various subspecialites (eg multiple appts) Interventional Cardiology General Cardiology Treatment Surgery

9
CARE IS DECENTRALIZED Patients are forced to seek care sequentially from various subspecialites (eg multiple appts) Interventional Cardiology General Cardiology Treatment Surgery

10
CARE IS DECENTRALIZED Patients are forced to seek care sequentially from various subspecialites (eg multiple appts) Interventional Cardiology General Cardiology ? Treatment Surgery

11
IMPACT OF DECENTRALIZED CARE
System Perspective Patient Perspective Poor information transfer Duplicative care increases in direct costs Decreased quality Wastes patients’ time increase in indirect costs Patients lost in system delays care Patients lost to system go elsewhere Patients forced to make decisions based on complex information provided by multiple disparate sources with competing interests

12
Compared w 4 other comparable countries, U.S. patients more likely to:
-undergo duplicative testing -tell the same story to multiple HCPs -experience delay in reporting of results

13
PATIENT CENTERED MODEL
Diagnostics Disease-Specific “Clinic” (eg, CAD, Valve, HF, Ao) w Cards/Imaging/IC/CVS Referring Treatment
 w Cards/Imaging/IC/CVS. Referring. Treatment.")
14
IT IS POSSIBLE. . . 87yo h/o B THR and L TKR, severe PHTN, walks w a cane but highly functional p/w severe AS; eval for TAVR Thurs: Referral secured by outreach team Facilitated direct MD-to-MD contact Tues: Next Valve Clinic date seen by Cards, CTS, IC, Vasc TTE (Cards) – previously unscheduled CTA C/A/P (Rads) – previously unscheduled Fri: Returned to referring MD for cardiac cath Sun: Spent Mothers Day with family Mon: Underwent TF-TAVR Uneventful case Awake and extubated < 30 mins after the procedure Fri: Discharged on POD #5 Home before the NATO riots Yes, but this should NOT be a case study it should be the standard of care
 – previously unscheduled. CTA C/A/P (Rads) – previously unscheduled. Fri: Returned to referring MD for cardiac cath. Sun: Spent Mothers Day with family. Mon: Underwent TF-TAVR. Uneventful case. Awake and extubated < 30 mins after the procedure. Fri: Discharged on POD #5. Home before the NATO riots. Yes, but this should NOT be a case study it should be the standard of care.")
15
These barriers between specialties are no longer compatible with the effective application of today’s hybrid therapies

16
TREATMENT OPTIONS WERE DISCRETE
ONCE UPON A TIME… TREATMENT OPTIONS WERE DISCRETE Its clear who provides services More likely to be complementary, less likely competing Medical Physician Surgeon Drugs Open Surgery

17
INTERVENTIONAL ERA: RECENT PAST
Technologies were competing and mutually exclusive, eg: PCI (IC) vs CABG (CTS) aka “The Stent Wars” Open distal bypass (VS) vs peripherial stenting (IC/IR) Drugs Interventions Open Surgery
 vs CABG (CTS) aka The Stent Wars Open distal bypass (VS) vs peripherial stenting (IC/IR) Drugs. Interventions. Open Surgery.")
18
HYBRID ERA: PRESENT Drugs Interventions Hybrid MIS Open Surgery
Differences are obscured Its unclear who provides which services/treats which pts Drugs Interventions Hybrid MIS Open Surgery

19
EXAMPLE: TAVR Procedural Steps Planning CT and echo: Aortic Valve Aorta Lower extremities Vascular access Percutaneous Femoral, iliac, axillary Apical, aortic Pass large bore- sheath -- approved device is only slightly smaller in caliber than a garden hose Cross the aortic valve Position Valve under echo/fluoro Balloon valvuloplasty/valve replacement Closure of access site Perc Open Complications Valve embolization Dissection Coronaries Vascular injury Specialty most suited Cards/CT Rads/CT/VS Rads/VS/IC IC/VS VS/CT CT IC CT/Cards/IC VS No single specialty competent to do all parts based on traditional training/skills. . . A TEAM IS REQUIRED

20
WHAT IS A TEAM? Comprises a group of people linked in a common purpose
Especially appropriate for conducting tasks that are high in complexity and have many interdependent subtasks Members have complementary skills Allow each member to maximize their strengths minimize their weaknesses generates synergy Improves on what is possible for an individual actor

21
In baseball, team members have different skills and fulfill different roles

22
THIS IS A PITCHING STAFF… NOT A BASEBALL TEAM
Curveball Knuckleballer Slightly different niches BUT… Working in parallel, not together All filling the same role Submarine Leftie Split-finger fastball

23
IN HEALTHCARE, “TEAM” MEMBERS OFTEN HAVE NEARLY IDENTICAL SKILLS

24
Elimination of these barriers improves patient outcomes and offers a non-zero opportunity for providers

25
GAME THEORY Zero Sum Scenarios Non-Zero Sum Scenarios
participant's gain (or loss) of utility is exactly balanced by the losses (or gains) of the utility of the other participant(s). If one gains, another losses Only Win-Lose possible Example: party goer eats a piece of cake…there is less cake for the other partiers Non-Zero Sum Scenarios a participant's gain (or loss) of utility is not balanced by the losses (or gains) of the utility of the other participant(s). If one gains, another may also gain Win-Win possible Example: Prisoners’ dilemma
 of utility is exactly balanced by the losses (or gains) of the utility of the other participant(s). If one gains, another losses. Only Win-Lose possible. Example: party goer eats a piece of cake…there is less cake for the other partiers. Non-Zero Sum Scenarios. a participant s gain (or loss) of utility is not balanced by the losses (or gains) of the utility of the other participant(s). If one gains, another may also gain. Win-Win possible. Example: Prisoners’ dilemma.")
26
WIN-WIN scenarios exist
PRISONERS DILEMMA In a NON-ZERO scenario. . . one player does not need lose for another to win. . . WIN-WIN scenarios exist Prisoners DO NOT cooperate more jail time (WIN-LOSE) Prisoners DO cooperate less jail time (WIN-WIN) Prisoners DO NOT cooperate more jail time (WIN-LOSE) Prisoners DO NOT cooperate more jail time (LOSE-LOSE)
 Prisoners DO cooperate less jail time (WIN-WIN) Prisoners DO NOT cooperate more jail time (WIN-LOSE) Prisoners DO NOT cooperate more jail time (LOSE-LOSE)")
27
OUR WORLD IS INCREASINGLY NON-ZERO
“The more complex societies get the more complex the networks of interdependence. . . the more people are forced in their own interests to find. . . win-win [non-zero] solutions instead of win-lose [zero] solutions. . . We find as our interdependence increases we do better when. . . people [around us] do better as well.” —an ex-US President, December 2000

28
OUR WORLD IS INCREASINGLY NON-ZERO
“The more complex therapies get the more complex the networks of interdependence. . . the more clinicians are forced in their own interests to find. . . win-win [non-zero] solutions instead of win-lose [zero] solutions. . . We find as our interdependence increases we and--our patients--do better when. . . people [around us] do better as well.”

29
REVELATION In a 25 mile radius of UofC, there are:
75 cardiac surgery programs (more than NYS - 7x the pop) 79 cath labs (more than Canada – 12.5x the pop) No dominant center Each center is doing a fraction of the total CV work in the area What if we worked together? try to take cases from the guys across the street . . . rather than cases from the guys across the hall?
 79 cath labs (more than Canada – 12.5x the pop) No dominant center. Each center is doing a fraction of the total CV work in the area. What if we worked together try to take cases from the guys across the street rather than cases from the guys across the hall")
30
OUR EXPERIMENT Create a team composed of members with different skills sets/from different disciplines Cardiology Vascular surgery Radiology Objectives: To expand our practice To increase our volume To improve our outcomes To deliver patient-centric care Methods: Sought out opportunities to collaborate Leverage unique skills and existing systems Interventional Cardiology Cardiac Surgery Anesthesiology

31
NEW SYSTEMS PRACTICES

32
TRANSPARENCY/SHARE THE WORK
Eliminate the “I’m a hammer you’re a nail” approach = Pt gets the procedure the MD can offer Instead, offer the best solution for the pt Coronary revascularization cases discussed (IC and CTS) Valve cases discussed in valve conf and valve clinic (Cards/CTS/IC) Aortic cases discussed in aortic conf and aortic clinic (CTS/VS/Cards)
 Valve cases discussed in valve conf and valve clinic (Cards/CTS/IC) Aortic cases discussed in aortic conf and aortic clinic (CTS/VS/Cards)")
33
LEVERAGE ESTABLISHED SYSTEMS
Example: ECMO Emergency surgery only exists in Level 1 Trauma Centers….and on TV OR: 1-3 hours to active 80%+ of ECMO is now initiated in the cath lab Advantages Cath lab - Faster and Cheaper activated in mins Cost < 20% of the OR Better imaging for perc access, if needed Opportunity for collaboration

34
EXAMPLES OF CLINICAL COLLABORATION

35
AO DEBRACHING/REOP ARCH
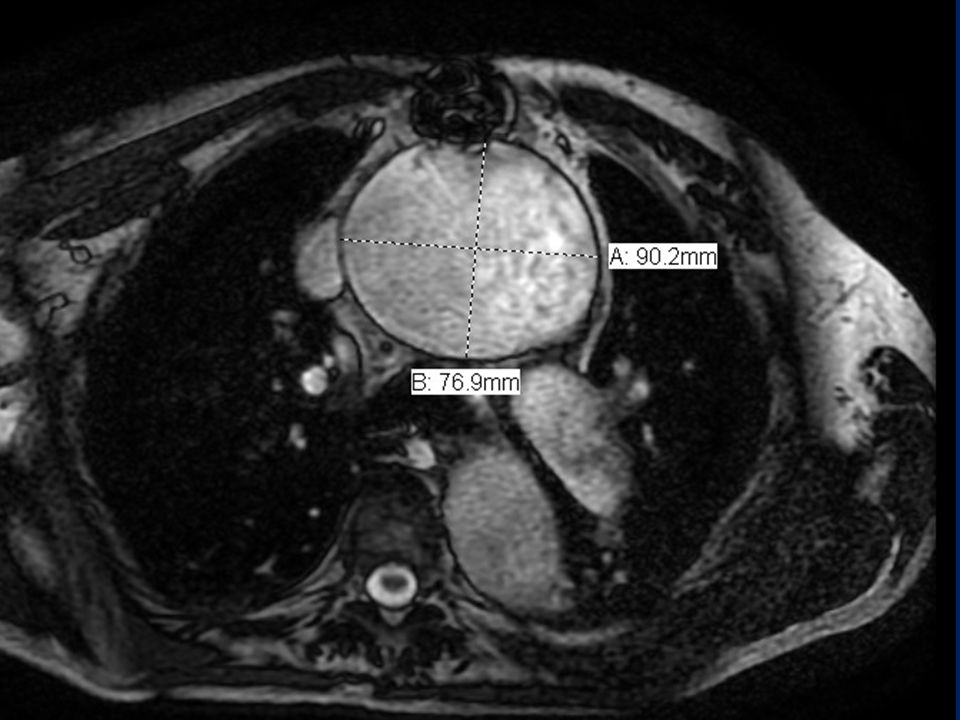
82yo s/p repair a 6 cm Asc Ao Aneurysm in 1993 4 Aneurysms Recurrent Asc Ao aneurysm extending into the arch (9 cm) Innominate aneurysm (4.4 cm) Right subclavian aneurysm (2.4 cm) Left common carotid aneurysm (2.8 cm) -> Also had mid-descending TA (5.0 cm) and AAA (~5cm) LAD stent placed by IC preop To OR after 2 wks of plavix
 Innominate aneurysm (4.4 cm) Right subclavian aneurysm (2.4 cm) Left common carotid aneurysm (2.8 cm) -> Also had mid-descending TA (5.0 cm) and AAA (~5cm) LAD stent placed by IC preop. To OR after 2 wks of plavix.")
36
A B

38
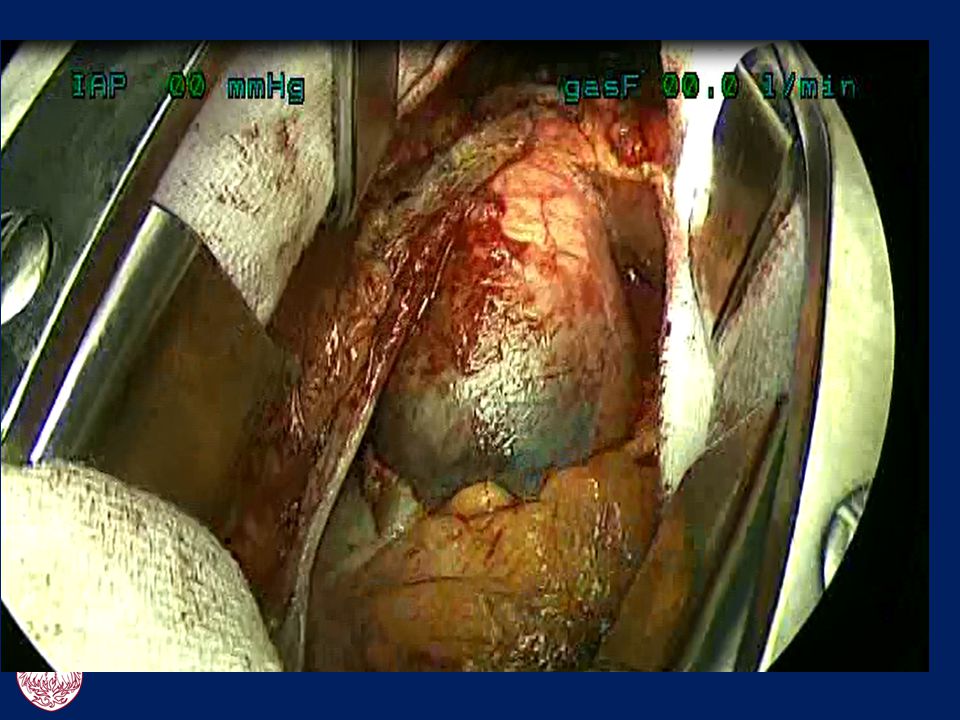
Apposition of the aneurysm to the previous sternotomy with compression of the vena cava and innominate veins

39
Apposition of the aneurysm to the previous sternotomy with compression of the vena cava and innominate veins

40
Vasc Surgery LCA to LSCA transposition

41
Vasc Surgery LCA to LSCA transposition Graft LCA to RCA to RSCA bypass

42
Vasc Surgery LCA to LSCA transposition Graft LCA to RCA to RSCA bypass Graft was connected to the pump used as inflow

43
Circuit allowed for: Exclusion 3 aneurysms of great vessels Decompressed Ao during reop sternotomy Allowed for cerebral protection during distal mosis by clamping LCA to initiate ACP Chest opened with decompressed aorta intact

44
Cardiac Surgery Distal Ao under ACP (17 mins) AVR Prox Ao - new to old graft XCL time: 97 mins
 AVR Prox Ao - new to old graft XCL time: 97 mins")
45
VS and CTS Off Pump graft -> RSCA; graft to RCA Extubated on POD #2 D/c’ed: neuro intact nl EF baseline Cr

46
TRANS-ILIAC - TAVR Proctored case Proctor extremely experienced w TAVR
IC does TF cases w/o surgeon Reviewed case and recommended cancelling 2/2 poor femoral access Proposed was approach was trans-iliac w iliac conduit via RP exposure by VS/CTS Proctor resistant b/c he had never done (seen) it Relented based on surgeons’ experience w approach for other procedures Procedure successfully performed < 2hrs skin-to-skin
 it. Relented based on surgeons’ experience w approach for other procedures. Procedure successfully performed < 2hrs skin-to-skin.")
47
ASCENDING AORTIC PSEUDOANEURYSM
57yo s/o Type A Dissection Repair in presented with chest pain PMHx: CRI, previous significant EtOH and smoking Found to have a PSA at prox suture line Operative mortality >>20%

48
Selective cannulation of pseudoaneurysm using coronary catheter
WORK-UP Aortic root injection Selective cannulation of pseudoaneurysm using coronary catheter

49
THE PLAN 10mm graft to LSCA for device access (Vasc)
8mm graft to RSCA to initiate CPB (CTS) Selective catheterization of LCA (IC) Approach allowed for: Control BP/volume status for more precise deployment of device Protection if coronary covered
 Selective catheterization of LCA (IC) Approach allowed for: Control BP/volume status for more precise deployment of device. Protection if coronary covered.")
50
THE TEAM IC CTS VS Cards Imaging/Anes

51
THE RESULT Successful deployment Exclusion of PSA D/ced home POD #2

52
CSB/TEVAR 72yo w large penetrating ulcer requiring CSB and TEVAR
Possible approaches: Advantages of Concomitant Approach: Single trip to the OR; Less OR utilization Potential for decrease LOS, faster recovery Advantages of Staged Approach No physician fatigue – 2 short cases “If complication occurs, we know who caused,” but…if the patient has a stroke, do THEY really case “who caused it”? Actual Approach - Concomitant HD #1: Spinal drain by Anes HD #2: 5 hours in OR; labor divided -> little stress/fatigue, max learning opportunity VS + fellow -> LCA-graft anastomosis CTS + fellow -> LSCA-graft anastomosis VS + CTS + fellows -> TEVAR HD #4: pt discharged

53
CSB/TEVAR Secondary advantage of collaboration – prepared for complications If arch is covered by VS – CTS likely is needed for bailout If iliac is avulsed by CTS – VS likely is needed for bailout If each service is not immediately available…complication is likely irreversible before help arrives If each service is committed to primary treatment choice, they will be more committed bailout if needed

54
COMPLICATION AFTER TAVR
77yo with severe, symptomatic AS Deemed in operable 2/2 h/o radiation to chest Undergoes uneventful TAVR procedure LFA sheath pulled in ICU At MN, noted to have no pulses below L knee Vascular surgeon involved in pts original TAVR case was consulted Taken immediately to OR for embolectomy No discussion of possible vasospasm, trial heparin, watchful waiting Pulses regained in OR Pts remaining hosp course uneventful

55
Even more compelling when hybrid room is available
R/O AoD 68yo w substernal pain x 5 hrs presents to an OSH Reported to have moderate to severe AI and moderate pericardial effusion Presumed diagnosis: Type A AoD Outside ED called Transfer center paged covering surgeon, but in OR (unable to be reached) CT Surgeon was reached….accepted the pt UCAN (helicopter) dispatched Pt directly to OR TEE revealed: mild AI, trace effusion, moderate TR No evidence of AoD, but (+) RV dysfunction Pt transferred directly to cath for aortography, diagnostic cath possible PCI RCA stent placed Repeat CT and TEE on HD#1 – no evidence of AoD Discharged on POD#3 Even more compelling when hybrid room is available
 CT Surgeon was reached….accepted the pt. UCAN (helicopter) dispatched. Pt directly to OR. TEE revealed: mild AI, trace effusion, moderate TR. No evidence of AoD, but (+) RV dysfunction. Pt transferred directly to cath for aortography, diagnostic cath possible PCI. RCA stent placed. Repeat CT and TEE on HD#1 – no evidence of AoD. Discharged on POD#3. Even more compelling when hybrid room is available.")
56
AoD 61 yo M presented to OSH with substernal chest pain radiating to the back Diagnosis: Type A AoD Outside ED called > paged Ao pager Reached Vasc Surgeon 1st….accepted the pt Pact to “Just say YES” eg AoD accepted by cards, AAA by CTS, Type As by Vasc Without collaboration, vasc surgeon will tell OSH to find a CT surgeon OSH may call other hospital

57
UCAN DISPATCHED

58
PROCEDURE Pt directly to OR TEE confirmed Type A – AoD w severe AI
Cardiac surgeon made a 3F valved conduit in preparation for aortic root replacement (30 mins) Concurrently vascular surgeon performed R axillary cannulation in preparation for CPB Saved mins. . . and possibly the patients life
 Concurrently vascular surgeon performed R axillary cannulation in preparation for CPB. Saved mins. . . and possibly the patients life.")
60
PROCEDURE Type A repair w aortic root replacement and hemiarch under ACP At end of procedure, lactate = 10 Gen surg consult; diagnostic lap’scopy in OR: (-) ischemic bowel
 ischemic bowel.")
61
FAMILY LETTER “I’d like to thank you for saving my father’s life last week. My dad is not only alive, but is walking, talking, and ornery as ever all thanks to your expertise. It truly has been a surreal week to say the least. I feel very fortunate to know that my father was in such good hands. “I wanted to extend my most sincere gratitude towards you and your extremely skilled and professional team at U of C for your amazing and miraculous work. Thank you a million times over, from the bottom of our hearts (and the top of my father’s newly grafted aorta).” Best regards
. Best regards")
62
NEXT STEPS

63
BLURRING LINES Cross coverage Disease-specific pagers Clinics Cases
TAVR covered by IC/CTS Aortic covered by VS/CTS Clinics Aortic staffed by VS/CTS/CV Radiology Valve staffed by Cards/Cards Imaging/IC/CTS/VS Cases Pact to “Just say YES” (eg .AoD accepted by cards; AAA by CTS; Type As by Vasc) Cross training: in combined cases, attempt the part less comfortable w under the supervision of more experience operators
 Cross training: in combined cases, attempt the part less comfortable w under the supervision of more experience operators.")
64
COMMON OUTREACH CME w outreach team Disease specific contact/pager
Aortic disease: (UCCAD)/8222 TAVR: (TAVR) Worked with the call center to initiate a phone tree Websites Visits/day: ~200 Pageviews/day: ~300 Clinic Visits/week: 1-3 4 OR cases per mo Retention of clinic patients Bottom line < $3000
/8222. TAVR: (TAVR) Worked with the call center to initiate a phone tree. Websites. Visits/day: ~200. Pageviews/day: ~300. Clinic Visits/week: OR cases per mo. Retention of clinic patients. Bottom line < $3000.")
65
POTENTIAL BENEFITS Patients Providers Healthcare System

66
POTENTIAL BENEFITS: PATIENTS
Care focused on patients condition Avoid competing sales pitches Higher quality Receive appropriate therapies More eyes on the pts (attendings/fellows/APNs/PAs from multiple service) Decreased costs Direct and indirect Decreased delay in care Higher patient satisfaction
 Decreased costs. Direct and indirect. Decreased delay in care. Higher patient satisfaction.")
67
POTENTIAL SUCCESS: PROVIDERS
Better working environment Common mission No finger pointing Egos checked at the door Easier acquisition of others’ input Planning procedures, management, complications Providers more invested in al CV patients Broader understanding of disease process and available therapies Learning new skill sets “CCF Effect” – MDs refer to team/organization, not a specific MD Decreases hurt egos when a CTS refers a complex CTS pt to an outside CTS; IC a complex IC pt; or VS a complex VS pt

68
POTENTIAL SUCCESS: PROVIDERS
Expanding practice TAVR, Frozen Elephant Trunk, Asc Ao Stent Graft, Ao Arch Stent, Antegrade Ao Stent, Perc Closure of PSA, Perc Closure of Aortic Valve, Pararenal Snokel, MD-Modified Stent Graft Increased volume TEVAR: , 2011 – 8, 2012 – 20+ (through Aug; 40 projected) EVAR: up 40% over previous year Academic productivity/TAVR Team 2011: 50 publications 2012: 40 (to date)
 EVAR: up 40% over previous year. Academic productivity/TAVR Team. 2011: 50 publications. 2012: 40 (to date)")
69
POTENTIAL BENEFITS: THE HEALTH CARE SYSTEM
Decreased resource utilization Decreased duplicative testing Decreased need for multiple encounters Higher quality care More appropriate/balanced use of technology Team polices themselves for appropriateness rather than leaving it to an outside non-clinical entity (eg govt, insurance) Better outcomes
 Better outcomes.")
70
OBSTACLES Playing field – need a hybrid room; available in Feb
“The Division of . . .Cardiac Surgery/Cardiology/Vascular Surgery . . .” Artificial divisions exist between groups that should naturally work together, particular in our 100% hospital-based employment model Resources no mechanism to share across disciplines; different services Billing who gets the RVUs; how to divide Personal Incentives Reimbursement Prob not maximizing Existing Culture buy-in not universal

71
Presenting ourselves separately?
THE FUTURE? Presenting ourselves separately?

72
FUTURE Single CV Service Line Integrated Interventional Service
Structural heart, PCI, TEVAR/EVAR, Hybrid cases Cross training/covering Present: CT and VS cross cover aortic cases Future: CT and IC; IC and VS cross cover cases IC/CT/VS -> CVI VS/CT -> CVS

73
VALVE DISEASE CORONARY DISEASE CORONARY DISEASE EP AORTIC DISEASE HEART FAILURE PVD

74
For Providers: Win-Win
For Patients: Win Win-Win-Win

Similar presentations

 Associate Professor Department of Orthopaedics & Rehabilitation Portland, Oregon.>")











 Arch Debranching vs. Elephant Trunk for Hybrid Repair of the Proximal Thoracic Aorta Arch Debranching versus Elephant Trunk Procedures for Hybrid Repair.>")





