Download presentation
Presentation is loading. Please wait.

1
Pediatrics in Review Craig T. Carter, D.O. Associate Professor
Department of Emergency Medicine and Pediatrics University of Kentucky 2/2013

2
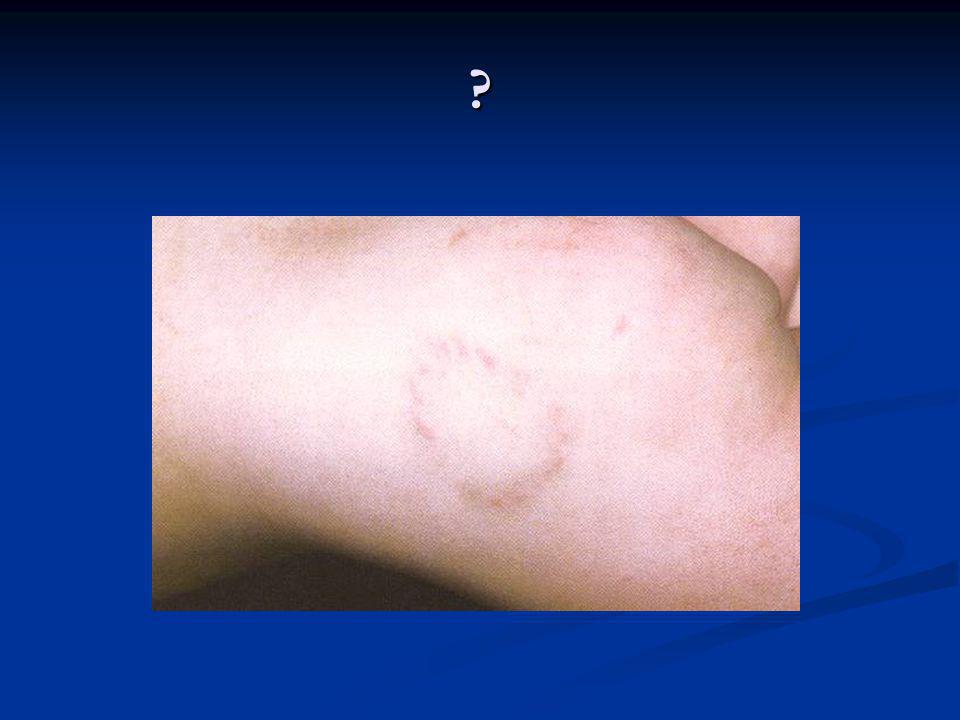
Some Pictures Do Not Require Captions ….

8
“Ringworm” Ringworm often causes itchy, red, scaly, slightly raised, expanding rings on the skin of the trunk of the body, face, groin or thigh fold. The ring grows outward as the infection spreads, and the center area becomes less actively infected.

9
Tinea… Athlete's foot (tinea pedis). This form affects the moist areas between your toes and sometimes on your foot itself. Jock itch (tinea cruris). This form affects your genitals, inner upper thighs and buttocks. Ringworm of the scalp (tinea capitis). This form is most common in children and involves red, itchy patches on the scalp, leaving bald patches.
. This form affects your genitals, inner upper thighs and buttocks. Ringworm of the scalp (tinea capitis). This form is most common in children and involves red, itchy patches on the scalp, leaving bald patches.")
10
Q: How are kids airways different?

11
Anatomical airway issues in kids
big tongue, soft tissue obstruction soft trachea no cuff soft VC no stylet anterior larynx short trachea narrowest at subglottis nose breathers < 6 mos big occiput big epiglottis straight blade

13
Airway positioning for children <2yrs

15
Chalazion

16
Chalazion Chalazions may be treated with any one of the following methods: 1) Antibiotics and/or steroid drops of injections; 2) Warm compresses; Warm compresses can be applied in a variety of ways, The simplest way is to hold a clean washcloth, soaked in hot water, against the closed lid for five to ten minutes, three to four times a day. Repeatedly soak the washcloth in hot water to maintain adequate heat. 3) Massage of expression of the glandular secretions; 4) Surgical incision or excision.
 Warm compresses; Warm compresses can be applied in a variety of ways, The simplest way is to hold a clean washcloth, soaked in hot water, against the closed lid for five to ten minutes, three to four times a day. Repeatedly soak the washcloth in hot water to maintain adequate heat. 3) Massage of expression of the glandular secretions; 4) Surgical incision or excision.")
21
Pre-septal and Orbital Cellulitis
Bacterial infection usually results from local spread of adjacent URTI Preseptal usually follows periorbital trauma or dermal infection Orbital most commonly secondary to ethmoidal sinusitis Preseptal Staphylococcus aureus and Staphylococcus epidermidis Streptococcus Orbital Strep pneumoniae and pyogenes, Staph aureus Haemophilus influenzae, anaerobes

22
Answers when you do not know the answers…

23
What is this?

24
Burn Depth Superficial partial thickness burn
Pink, moist,thin walled blisters Intact sensation Heal in 2-3 weeks No scarring

25
Burn Depth Deep partial thickness burn Red or Blanched
Thick walled blisters Decreased two point discrimination Mild or exquisitely painful May heal by epithelialization 3-6 weeks High scar and contracture potential

26
Burn Depth

27
Burn Depth Full thickness burn White, charred leathery
Capillary and nerve beds destroyed Less painful/ insensate Only 1-2cm lesions can heal by contraction Grafting required High complication rates and prolonged recovery

28
Burn Depth

29
Extent of Burn What is the Rule of Nines?

31
Itchy, stayed at friends house overnight, woke with pet in bed

32
Flea Bites

33
Rash

34
Rash w/ fever and abd pain

35
So what is it? Get your clickers…
1. Meningococcemia 2. ITP/TTP 3. HUS 4. HSP 5. Petichial hemorrhages 6. RMSF

38
Henoch-Schonlein Purpura
Clinical Presentation Effects predominantly young children, but adults are also affected Peak incidence is 4-5 years of age There is a slight male predominance The condition is more prevalent in the winter and early spring The onset of illness is usually sudden and is preceded by a URI in at least 1/3 of cases

39
HSP - Clinical Presentation
Classic Triad of symptoms is the most common presentation Purpura Colicky abdominal pain arthritis 50% of children may present with symptoms other than purpura Risk of Intuss

41
Q: How much of their blood volume can a kid lose, and still have a NORMAL bp?

42
Q: How much of their blood volume can a kid lose, and still have a NORMAL bp?
40%

44
Lymphadenitis

46
Spontaneous subconjunctival haemorrhage
Painless red eye without discharge VA not affected Clear borders Masks conjunctival vessels Check BP and body for other hemorrhages No treatment (lubricants) 10-14 days to resolve If recurrent: clotting, FBC Always consider abuse…
 days to resolve. If recurrent: clotting, FBC. Always consider abuse…")
47
Liver Laceration from ATV

50
What is it? 1. ECM 2. EM 3. Fifths disease 4. No clue
5. Erythema Nodosum

51
What is it? 1. ECM 2. EM 3. Fifths disease 4. No clue
5. Erythema Nodosum

53
Erythema Multiforme Symmetrically distributed, erythematous, expanding macules or papules evolve into classic iris or target lesions, with bright red borders and central petechiae, vesicles, or purpura. Lesions may coalesce and become generalized. Vesiculobullous lesions develop within preexisting macules, papules, or wheals. Rash favors palms and soles, dorsum of the hands, and extensor surfaces of extremities and face. Postinflammatory hyperpigmentation or hypopigmentation may occur. Eye involvement occurs in 10% of EM cases, mostly bilateral purulent conjunctivitis with increased lacrimation. Mucous membrane blistering occurs in about 25% of cases of EM, is usually mild, and typically involves the oral cavity.

54
54

56
Varicella 56

57
Varicella Agent: varicella zoster virus Transmission: respiratory
Period of communicability: 1 day before eruption of vesicles. Prodromal phase: slight fever, malaise, pruritic rash; macular to papular to vesicular. 57

58
Management of Varicella
Isolation Skin care: tepid bath, calamine lotion, clip finger nails. Keep from scratching Antihistamines for itching - Benadryl No ASA – acetaminophen only. Varicella vaccine now available. 97% immunity in 2m-12 y 78% immunity in 13y-adult 2% can have attenuated disease 58

59
Parent of the year…NOT!

60
What is it and what is next best test?

61
Seat Belt sign

64
What is it? 1. Mumps 2. Measeles 3. Ruebella 4. Small pox 5. No clue
Occurs more commonly in naïve populations Harder when physician has never seen a case and non-susceptible population at large = few cases

65
Measles: Diagnosis / Clinical
Clusters of children with fever, cough, conjunctivitis, coryza, morbilliform rash Occurs more commonly in naïve populations Harder when physician has never seen a case and non-susceptible population at large = few cases

66
Measles: Signs and Symptoms
Peak of Illness 2-4 days after onset of rash Other signs and symptoms Anorexia, malaise, HSM Resolution Rapid improvement at end of febrile period (1 week) Complete recovery in days Pearl: darker-skinned children Sandpaper feel to rash may be helpful
 Complete recovery in days. Pearl: darker-skinned children. Sandpaper feel to rash may be helpful.")
67
Measles or Rubeola Agent: Virus
Transmission: respiratory, blood and urine Incubation period: 10 to 20 days Period of Communicability: 4 days before and 5 days after rash appears. Prodromal stage: fever, cough, conjunctivitis, Koplik spots. Can get same rash/illness up to 10 d after MMR

68
Measles: Signs and Symptoms
Rash Hairline Behind Ears Erythematous papular eruption Travels inferior over 2-3 days Coalesces into macular “splotches” Often desquamates at end of illness Face Trunk Limbs

70
Nothing here

73
Parent of the year…NOT

78
Down Syndrome Described by John Landon Down in 1866
Etiology: nondisjuction mutation resulting in Trisomy 21 Prevalence 1:700 Most common chromosomal anomaly Associated with Maternal age > 35

79
Down Syndrome Characteristics Macroglossia Micrognathia
Midface hypoplasia Flat occiput Flat nasal bridge Epicanthal folds Up-slanting palpebral fissures Progressive enlargement of lips Hands: Simian crease (continuous line in the palm of the hand), short broad hands, underdevelopment of middle portion of the 5th finger resulting in the finger bending towards the outside of the hand.
, short broad hands, underdevelopment of middle portion of the 5th finger resulting in the finger bending towards the outside of the hand.")
80
Name 4 medical issues to consider in Down Syndrome patients…especially in ED!
Atlantal-axial dislocation – be wary in traumas or downs patient with neck pain or inability to ambulate Cardiovascular anomalies (40%) ASD, VSD, Tetralogy of Fallot, PDA GI anomalies (10-18%) Pyloric stenosis, duodenal atresia, TE fistula Malignancy 20 fold higher incidence of ALL Gonadal tumors
 ASD, VSD, Tetralogy of Fallot, PDA. GI anomalies (10-18%) Pyloric stenosis, duodenal atresia, TE fistula. Malignancy. 20 fold higher incidence of ALL. Gonadal tumors.")
81
Q: What’s the formula for minimal systolic bp for age?

82
Q: What’s the formula for minimal systolic bp for age?
70 + (Age x 2) Eg for 5 yo: 70+5x2 = 80
 Eg for 5 yo: 70+5x2 = 80.")
83
MCAD ? Group effort - Tell me everything you know
(I am certain this will be a very short conversation!)
")
84
Medium chain acyl-CoA dehydrogenase deficiency (MCAD)
Fatty acid oxidation defect Disorder of ammonia detoxification Most common mitochondrial β oxidation disorder 1/10,000 5% of 313 cases SIDS Screen all infants of mothers with HELLP syndrome Results in acute toxic encephalopathy with episodes of nonketotic hypoglycemia in the 1st 2 years of life provoked by fasting v/lethargy after fasting , usually with URI/AGE In ED: coma, hypoglycemic hypoketotic, hyperammonemia, LFTs TX: D10 Avoid fasting Carnitine 100mg/k/d

88
Mulluscum Contagiosum

89
Dictation goofs and gaffs..
“Unsure the etiology of this left upper shimmy pain.” “He had reported that he slipped and fell landing primarily with his hip on the patient's right knee. The child did not lose consciousness and did not appear to strike any other body parts. They report a car immediately afterwards” “History of present illness: Six-year-old nontender by mother mother reports intermitten…”

90
Febrile Seizures CRITERIA FOR THE DIAGNOSIS OF SIMPLE FEBRILE SEIZURE
Between 6 months and 5 years of age Seizure lasting less than 15 minutes Fever present prior to the onset of the seizure No other neurologic diagnoses Non-focal, generalized seizure, involving all limbs No severe metabolic disturbance No more than a single seizure per 24-hour period No evidence of intracranial infection

91
Febrile SZ work-up Clinicians evaluating infants or young children after a simple febrile seizure should direct their attention toward identifying the cause of the child's fever. In general, a simple febrile seizure does not usually require further evaluation, specifically EEGs, blood studies, or neuroimaging. PEDIATRICS Vol. 127 No. 2 February 2011, pp

92
Febrile Seizures – Parental Education
The risk of febrile seizure in the general population is between ? 2% and 5% There is no evidence that treating simple febrile seizures with anti-epileptics decreases the incidence of epilepsy later in life or results in improved cognitive outcomes.

93
Febrile Seizures – Parental Education
If a patient is less than 12 months of age at the time of the first simple febrile seizure, the risk of second simple febrile seizure is 50%. If a patient is over 12 months of age at the time of the first simple febrile seizure, the risk of a second simple febrile seizure is 30%. Following a second simple febrile seizure, the risk of future simple febrile seizures is 50%, regardless of the age of the initial simple febrile seizure. The risk of epilepsy is minimally increased from 1% to 2.4% in patients who have a simple febrile seizure

96
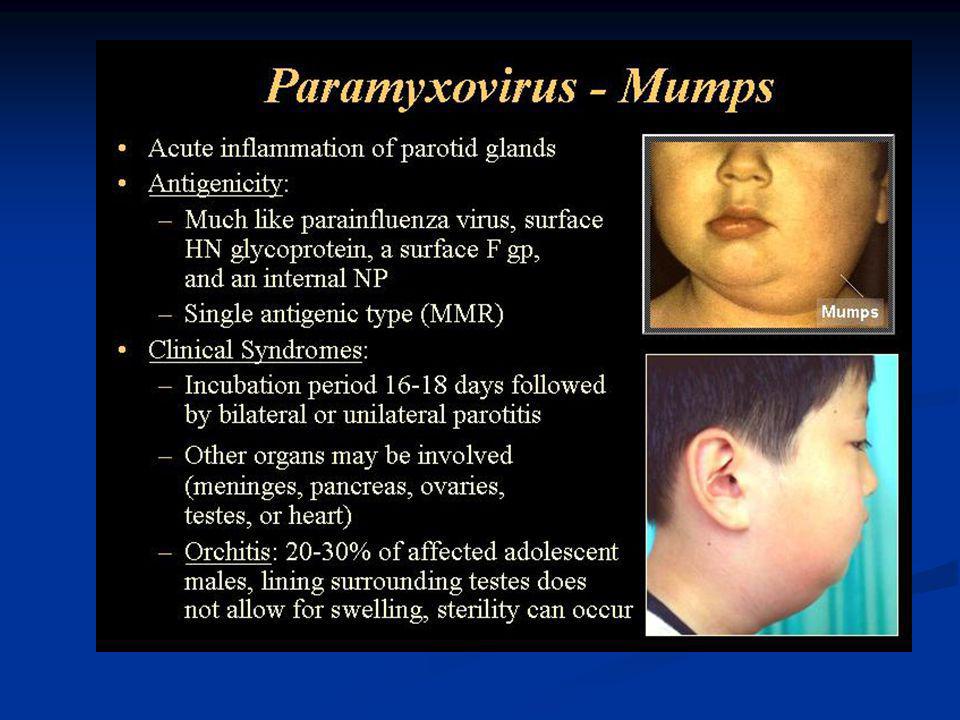
Mumps Clinical Features
Incubation period days Nonspecific prodrome of low-grade fever, headache, malaise, myalgia Parotitis in 30%-40% Up to 20% of infections asymptomatic May present as lower respiratory illness, particularly in preschool-aged children

97
Mumps Pathogenesis Respiratory transmission of virus
Replication in nasopharynx and regional lymph nodes Viremia days after exposure with spread to tissues Multiple tissues infected during viremia

98
?
99
Human Bites-ABUSE

100
Q: Name 4 things that can result in an agitated pediatric trauma patient.

101
Causes of agitation… Head Injury Decreased Oxygenation Shock
Altered LOC due to Alcohol, drug etc

102
What is this rash? Drug Reaction/Eruption

103
Treatment ?

104
Differential Dx ? List 3…

105
Hand edema – What is it? How about now? Coronary artery aneurysms

107
Kawasaki Disease - Clinical Manifestations
High fever Conjunctivitis Strawberry tongue Edema of hands and feed Reddening of palms and soles Lymph node swelling

108
Kawasaki Disease - Clinical Tests
LFTs/TBili Albumin ESR CRP Urine CBC Thrombocytosis Leukocytosis Anemia (normocytic)
")
109
A 4yo boy presents with painful rectal bleeding
A 4yo boy presents with painful rectal bleeding. Mom describes the blood as “bright red, my son is going to bleed to death!” The most common etiology of painful rectal bleeding in this age group is? Juvenile polyposis Anal fissure Crohn’s Disease Meckel’s diverticulum

110
A 4yo boy presents with painless rectal bleeding
A 4yo boy presents with painless rectal bleeding. Mom describes the blood as “bright red, my son is going to bleed to death!” The most common etiology of painless rectal bleeding in this age group is? Juvenile polyposis Anal fissure Crohn’s Disease Meckel’s diverticulum

111
Dictation goofs and gaffs… What???
“I discussed this with the family and felt as though he most likely had some dry skin no switching off in this area” “She is taken to court Riche already performed chest x-ray” “Patient presents with bruising the posterior thighs which appears consistent with Niceville trauma”

112
Salter 1 Salter 2 Salter 3 Salter 4 Salter 5

113
Salter 1 Salter 2 Salter 3 Salter 4 Salter 5

114
Salter 1 Salter 2 Salter 3 Salter 4 Salter 5

115
Salter Fracture I and II

116
Salter Fracture III, IV and V

117
?

118
Abnormal bruising patterns- ABUSE

119
Bowden & Greenberg Tripod position

120
Epiglottitis Symptoms
Acute inflammation of supra-glottic structures. Medical Emergency Sudden onset High fever Dysphasia and drooling Epiglottis is cherry red and swollenDiagnosis made on presenting symptoms No tongue blade in mouth Emergency tracheostomy set No procedures until in the operating room Keep quiet

121
Purple Rash Bowden & Greenberg Characteristic purpuric lesions.

122
Meningococcemia Necrosis of skin

123
Bacterial Meningitis Pathogens
Under 2 months :E-coli, Group B streptococcus, Listeria, Haemophilus influenza type B, and Streptococcus pneumonia Beyond neonate: Strep, Haemophilus, Neisseria.

124
Clinical Manifestation
Severe abdominal pain Currant jelly-like stool is a classic sign. Bowden & Greenberg

125
Intussusception Telescoping of part of intestine into an adjacent
distal portion. Bowden Text

126
Barium Enema Ball & Bindler

127
Gas filled loops of bowel

128
Necrotizing Enterocolitis
Necrotizing = damage and death of cells Entero = refers to intestines Colitis = inflammation of the colon60 to 80% are premature infants Feeding of concentrated formulas Infants who have received blood transfusion Infants with GI infections Infants with polycythemia: congenital heart disease

129
Q: List 3 trauma considerations that we often forget about, especially in children?

130
Q: List 3 trauma considerations that we often forget about?
Hypothermia Child Abuse Hazardous Environments

133
Myelomeningocele A protruding saclike structure
containing meninges, spinal fluid and neural tissue.

134
Bulging anterior fontanelle Eyes deviated downward “Setting” Sun sign
Bates: Physical Assessment

135
Severe Hydrocephalus

136
Hydrocephalus Greek meaning water on the brain
Dilation of the ventricles Two primary causes: Congenital .5 to 1% Acquired: Lesion, tumors, infection, intracranial bleed, myelomeningocele

138
Retinal Hemorrhages Normal retinal Retinal hemorrhage

140
What is it? MRSA Burn Grp A strep Yeast No clue

141
Erysipelas Streptococcal Skin Infections
Group A Streptococci (Strep. pyogenes), which cause erysipelas, an infection affecting the superficial layers of the skin, and which classically has sharply defined borders.
, which cause erysipelas, an infection affecting the superficial layers of the skin, and which classically has sharply defined borders.")
143
Clostridium tetani Anaerobic gram-positive, spore-forming bacteria
Spores found in soil, dust, animal feces; may persist for months to years Multiple toxins produced with growth of bacteria Tetanospasmin estimated human lethal dose = 2.5 ng/kg

144
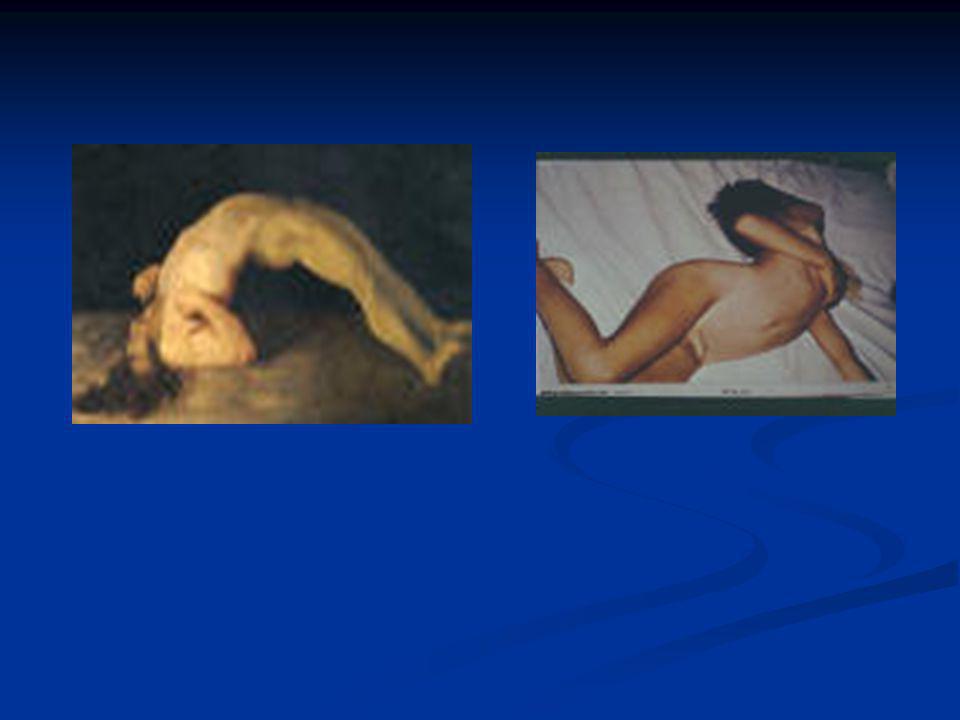
Tetanus Clinical Features
Incubation period; 8 days (range, 3-21 days) Three clinical forms: Local (not common), cephalic (rare), generalized (most common) Generalized tetanus: descending symptoms of trismus (lockjaw), difficulty swallowing, muscle rigidity, spasms Spasms continue for 3-4 weeks; complete recovery may take months
 Three clinical forms: Local (not common), cephalic (rare), generalized (most common) Generalized tetanus: descending symptoms of trismus (lockjaw), difficulty swallowing, muscle rigidity, spasms. Spasms continue for 3-4 weeks; complete recovery may take months.")
147
Pathogenesis of Lyme Borreliosis
Lyme disease characterized by three stages: Initially a unique skin lesion (erythema chronicum migrans (ECM)) with general malaise ECM not seen in all infected hosts ECM often described as bullseye rash Lesions periodically reoccur Subsequent stage seen in 5-15% of patients with neurological or cardiac involvement Third stage involves migrating episodes of non-destructive, but painful arthritis Acute illness treated with phenoxymethylpenicillin or tetracycline
) with general malaise. ECM not seen in all infected hosts. ECM often described as bullseye rash. Lesions periodically reoccur. Subsequent stage seen in 5-15% of patients with neurological or cardiac involvement. Third stage involves migrating episodes of non-destructive, but painful arthritis. Acute illness treated with phenoxymethylpenicillin or tetracycline.")
148
Diagnosis of Lyme Borreliosis

151
Rickettsia rickettsii - Rocky mountain spotted fever

155
Q: What are the risk factors for child abuse?

156
Child Abuse History story injuries history changing
injury development delay seeking help inappropriate level of concern Physical Exam multiple old and new bruises posterior rib #, sternum #, spiral # < 3 yo immersion burns, cigarette

158
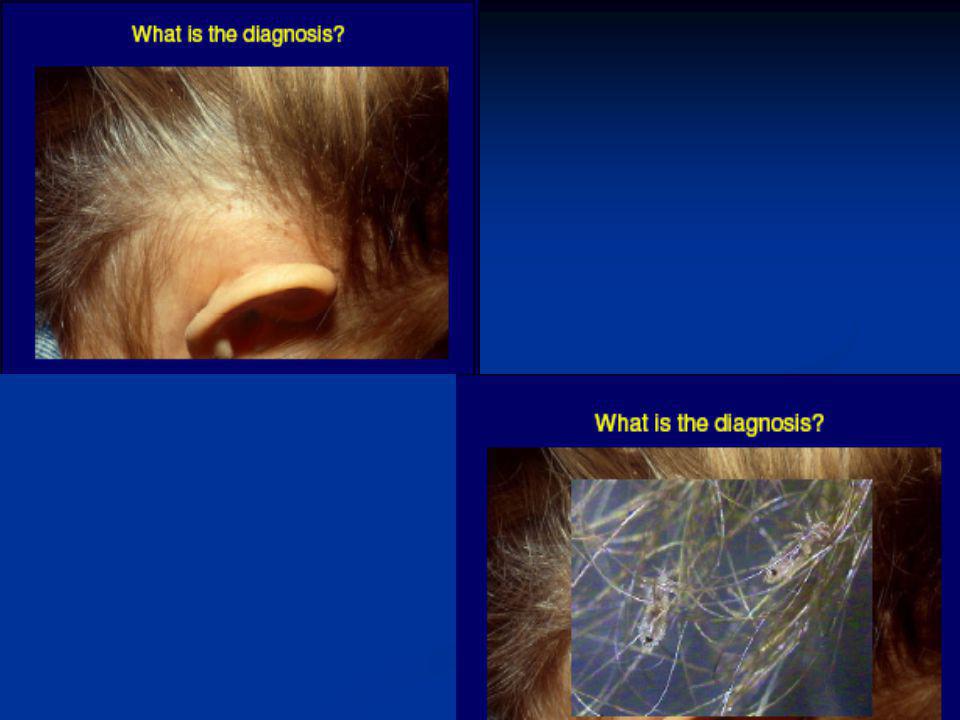
Impetigo Impetigo contagiosa The most common form of impetigo is impetigo contagiosa, which usually starts as a red sore on your child's face, most often around the nose and mouth. The sore ruptures quickly, oozing either fluid or pus that forms a honey-colored crust. Eventually the crust disappears, leaving a red mark that heals without scarring. The sores may be itchy

159
Staphylococcus aureus
Topical antibiotics. Your doctor may prescribe an antibiotic that you apply to your child's skin (topical antibiotic), such as mupirocin ointment (Bactroban). Topical antibiotics avoid side effects such as diarrhea that can result from some oral medications, but as with oral antibiotics, bacteria can become resistant to them over time. Oral antibiotics. Your doctor is likely to prescribe an oral antibiotic for ecthyma and severe cases of impetigo contagiosa. The specific antibiotic will depend on the severity of the infection and any allergies or conditions your child might have. Be sure to finish the entire course of medication even if your child seems better. This helps prevent the infection from recurring and makes antibiotic resistance less likely.
, such as mupirocin ointment (Bactroban). Topical antibiotics avoid side effects such as diarrhea that can result from some oral medications, but as with oral antibiotics, bacteria can become resistant to them over time. Oral antibiotics. Your doctor is likely to prescribe an oral antibiotic for ecthyma and severe cases of impetigo contagiosa. The specific antibiotic will depend on the severity of the infection and any allergies or conditions your child might have. Be sure to finish the entire course of medication even if your child seems better. This helps prevent the infection from recurring and makes antibiotic resistance less likely.")
161
Pityriasis Rosea It most often develops in the spring and the fall, and seems to favor adolescents and young adults. The skin rash follows a very distinctive pattern. In 3/4 of the cases, a single, isolated oval scaly patch (the "herald patch") appears on the body, particularly on the trunk, upper arms, neck, or thighs. These patches often form a pattern over the back resembling the outline of an evergreen tree with dropping branches. Patches may also appear on the neck and, rarely, on the face. These spots usually are smaller than the "herald" patch. The rash begins to heal after 2-4 weeks and is usually gone by 6-14. Aveeno oatmeal baths, anti-itch medicated lotions and steroid creams may be prescribed to combat the rash. Lukewarm, rather than hot, baths , ERYC, Famvir
 appears on the body, particularly on the trunk, upper arms, neck, or thighs. These patches often form a pattern over the back resembling the outline of an evergreen tree with dropping branches. Patches may also appear on the neck and, rarely, on the face. These spots usually are smaller than the herald patch. The rash begins to heal after 2-4 weeks and is usually gone by Aveeno oatmeal baths, anti-itch medicated lotions and steroid creams may be prescribed to combat the rash. Lukewarm, rather than hot, baths , ERYC, Famvir.")
163
Fractures of Abuse FIGURE 6. Multiple healing posterior rib fractures (arrows) from a compression injury of the chest. FIGURE 7. Metaphyseal or "bucket-handle" fracture (arrow) of the tibia.
 of the tibia.")
164
1. Parvovirus B19 2. Chilblans (cold) 3. Fifths Disease 4. Sixth disease 5. SLE butterfly rash 6. Erythema Infectiosum 7. No clue

165
Erythema Infectiosum (Fifth Disease)
History: Erythema infectiosum typically has an incubation period of 4-14 days and is spread primarily via aerosolized respiratory droplets. Transmission also occurs through blood products and from mother to fetus. The prodromal phase often is mild enough to be noticed only rarely but may include headache, coryza, low-grade fever, pharyngitis, and malaise. Infrequently, nausea, diarrhea, arthralgias, and abdominal pain may occur. In hosts who are immunocompetent, the patient is viremic and capable of spreading the infection only during the incubation period. Classic cutaneous findings follow within 3-7 days for some patients, while other patients may manifest no findings.

166
Erythema Infectiosum (Fifth Disease)
Physical: Pertinent physical findings predominantly are limited to the skin and joints. Skin (first stage): The exanthem begins with the classic slapped-cheek appearance. The bright red erythema appears abruptly over the cheeks and is marked by nasal, perioral, and periorbital sparing. The exanthem may appear like a sunburn, occasionally is edematous, and typically fades over 2-4 days. Skin (second stage): Within 1-4 days of the malar rash, an erythematous macular-to-morbilliform eruption occurs primarily on the extremities. While the eruption tends to favor the extensor surfaces, it can involve the palms and soles. Pruritus is rare. Skin (third stage): After several days, most of the second stage eruption fades into a lacy pattern, with particular emphasis on the proximal extremities. Despite its synonym, slapped-cheek disease, the reticulate pattern is distinctly characteristic for erythema infectiosum and may be the only manifestation of the illness. The third stage lasts from 3 days to 3 weeks. After starting to fade, the exanthem may recur over several weeks following physical stimuli, such as exercise, sun exposure, friction, bathing in hot water, or stress.
: The exanthem begins with the classic slapped-cheek appearance. The bright red erythema appears abruptly over the cheeks and is marked by nasal, perioral, and periorbital sparing. The exanthem may appear like a sunburn, occasionally is edematous, and typically fades over 2-4 days. Skin (second stage): Within 1-4 days of the malar rash, an erythematous macular-to-morbilliform eruption occurs primarily on the extremities. While the eruption tends to favor the extensor surfaces, it can involve the palms and soles. Pruritus is rare. Skin (third stage): After several days, most of the second stage eruption fades into a lacy pattern, with particular emphasis on the proximal extremities. Despite its synonym, slapped-cheek disease, the reticulate pattern is distinctly characteristic for erythema infectiosum and may be the only manifestation of the illness. The third stage lasts from 3 days to 3 weeks. After starting to fade, the exanthem may recur over several weeks following physical stimuli, such as exercise, sun exposure, friction, bathing in hot water, or stress.")
167
Erythema Infectiosum (Fifth Disease)
Complications of PV-B19 infection include the following: Aplastic crisis: The parvovirus infects erythroid cells, causing a reticulocytopenia that lasts 7-10 days. A healthy host experiences no consequences, since the normal lifespan of a red blood cell is 120 days. In patients with a background of shortened red blood cell survival, such as hemolytic anemia, an acute aplastic crisis ensues. Congenital infection: PV-B19 can cross the placenta during pregnancy and have a direct cytotoxic effect on fetal red blood cells. Infection

168
For a 24-kg child, the daily maintenance fluid requirement is approximately which of the following?
a cc/24hrs b cc /24hrs c cc/24hrs d cc/24hrs “4-2-1 rule” 0-10 kg 4cc/hr x wt 11-20 kg 2cc/hr x wt >20 kg 1cc/hr x wt Easy method Anyone >20kg =wt + 40

169
Proper fluid bolus for a 9kg infant who presents as a severe trauma with unstable vitals is?
a cc LR x 2, then 90cc/kg pRBCs b cc NSS, then 90 cc NSS c cc LR, then 180cc pRBCs d cc LR x 2, then 90cc 5% albumin, then 90cc pRBCs

172
Scarlet fever / scarlatiniform rash
Background: Scarlet fever is a syndrome characterized by exudative pharyngitis, fever, and scarlatiniform rash. It is caused by an infection with a pyogenic exotoxin-producing group A beta-hemolytic streptococci Infections occur year-round, but the incidence of pharyngeal disease is highest in school-aged children (5-15 y) during winter and spring and in a setting of crowding and close contact. Person-to-person spread by means of respiratory droplets is the most common mode of transmission. The incubation period for scarlet fever ranges from 12 hours to 7 days. Patients are contagious during the acute illness and during the subclinical phase.
 during winter and spring and in a setting of crowding and close contact. Person-to-person spread by means of respiratory droplets is the most common mode of transmission. The incubation period for scarlet fever ranges from 12 hours to 7 days. Patients are contagious during the acute illness and during the subclinical phase.")
173
Scarlet fever / scarlatiniform rash
The rash appears 1-2 days after onset of illness, first on the neck and then extending to the trunk and extremities. Scarlatiniform rash Exanthem texture is usually of coarse sandpaper, and the erythema blanches with pressure. The skin can be pruritic but usually is not painful. A few days following generalization of the rash, it becomes more intense along skin folds and produces lines of confluent petechiae known as the Pastia sign. These lines are caused by increased capillary fragility. The rash begins to fade 3-4 days after onset, and the desquamation phase begins. This phase begins with flakes peeling from the face. Peeling from the palms and around the fingers occurs about a week later and can last up to a month. TX Treat patients with a standard 10-day course of penicillin or erythromycin. This regimen prevents acute renal failure if antibiotics are initiated within 1 week of the onset of acute pharyngitis

174
Centor Criteria 1. Exudative pharyngitis 2. Fever
3. Anterior Cervical Lymphadenopathy 4. No “cold” symptoms (ie no cough or runny nose)
")
175
? (Hint – Not E.T.’s Finger)
")
176
Clubbing of Finger/Cystic fibrosis
Background: Cystic fibrosis (CF) is the most common lethal inherited disease in white persons. CF is an autosomal recessive disorder, and most carriers of the gene are asymptomatic. CF is a disease of exocrine gland function, involving multiple organ systems and chiefly resulting in chronic respiratory infections, pancreatic enzyme insufficiency, and associated complications in untreated patients. Pulmonary involvement occurs in 90% of patients surviving the neonatal period. End-stage lung disease is the principal cause of death. Gastrointestinal tract manifestations (intestinal) Neonates: Infants may present with intestinal obstruction at birth and a variety of surgical findings, for example, meconium ileus (7-10% of patients with CF), volvulus, intestinal atresia, perforation, and meconium peritonitis. Less commonly, passage of meconium may be delayed (>24-48 h after birth) or cholestatic jaundice may be prolonged. Infants and children: Patients present with increased frequency of stools, which suggests malabsorption (ie, fat in stools, oil drops in stools), failure to thrive, intussusception (ileocecal), or rectal prolapse.
 is the most common lethal inherited disease in white persons. CF is an autosomal recessive disorder, and most carriers of the gene are asymptomatic. CF is a disease of exocrine gland function, involving multiple organ systems and chiefly resulting in chronic respiratory infections, pancreatic enzyme insufficiency, and associated complications in untreated patients. Pulmonary involvement occurs in 90% of patients surviving the neonatal period. End-stage lung disease is the principal cause of death. Gastrointestinal tract manifestations (intestinal) Neonates: Infants may present with intestinal obstruction at birth and a variety of surgical findings, for example, meconium ileus (7-10% of patients with CF), volvulus, intestinal atresia, perforation, and meconium peritonitis. Less commonly, passage of meconium may be delayed (>24-48 h after birth) or cholestatic jaundice may be prolonged. Infants and children: Patients present with increased frequency of stools, which suggests malabsorption (ie, fat in stools, oil drops in stools), failure to thrive, intussusception (ileocecal), or rectal prolapse.")
178
Stevens-Johnson syndrome (SJS)
Pathophysiology: SJS is an immune-complex–mediated hypersensitivity disorder that may be caused by many drugs, viral infections, and malignancies. Cocaine recently has been added to the list of drugs capable of producing the syndrome. In up to half of cases, no specific etiology has been identified In 3-15% of cases, patients with severe SJS die

179
Stevens-Johnson syndrome (SJS)
The 4 etiologic categories are (1) infectious, (2) drug-induced, (3) malignancy-related, and (4) idiopathic. Viral diseases that have been reported include herpes simplex virus (HSV), AIDS, Coxsackie viral infections, influenza, hepatitis, mumps, mycoplasmal infection, lymphogranuloma venereum (LGV), rickettsial infections, and variola. Bacterial etiologies include group A beta streptococci, diphtheria, Brucellosis, mycobacteria, Mycoplasma pneumoniae, tularemia, and typhoid. Coccidioidomycosis, dermatophytosis, and histoplasmosis are the fungal possibilities. Malaria and trichomoniasis have been reported as protozoal causes. In children, Epstein-Barr virus and enteroviruses have been identified. Drug etiologies include penicillins and sulfa antibiotics. Anticonvulsants including phenytoin, carbamazepine, valproic acid, lamotrigine, and barbiturates have been implicated. Mockenhapupt et al stressed that most anticonvulsant-induced SJS occurs in the first 60 days of use. In late 2002, the US Food and Drug Administration (FDA) and the manufacturer Pharmacia noted that SJS had been reported in patients taking the cyclooxygenase-2 (COX-2) inhibitor valdecoxib. Various carcinomas and lymphomas have been associated. SJS is idiopathic in 25-50% of cases
 infectious, (2) drug-induced, (3) malignancy-related, and (4) idiopathic. Viral diseases that have been reported include herpes simplex virus (HSV), AIDS, Coxsackie viral infections, influenza, hepatitis, mumps, mycoplasmal infection, lymphogranuloma venereum (LGV), rickettsial infections, and variola. Bacterial etiologies include group A beta streptococci, diphtheria, Brucellosis, mycobacteria, Mycoplasma pneumoniae, tularemia, and typhoid. Coccidioidomycosis, dermatophytosis, and histoplasmosis are the fungal possibilities. Malaria and trichomoniasis have been reported as protozoal causes. In children, Epstein-Barr virus and enteroviruses have been identified. Drug etiologies include penicillins and sulfa antibiotics. Anticonvulsants including phenytoin, carbamazepine, valproic acid, lamotrigine, and barbiturates have been implicated. Mockenhapupt et al stressed that most anticonvulsant-induced SJS occurs in the first 60 days of use. In late 2002, the US Food and Drug Administration (FDA) and the manufacturer Pharmacia noted that SJS had been reported in patients taking the cyclooxygenase-2 (COX-2) inhibitor valdecoxib. Various carcinomas and lymphomas have been associated. SJS is idiopathic in 25-50% of cases.")
181
?

182
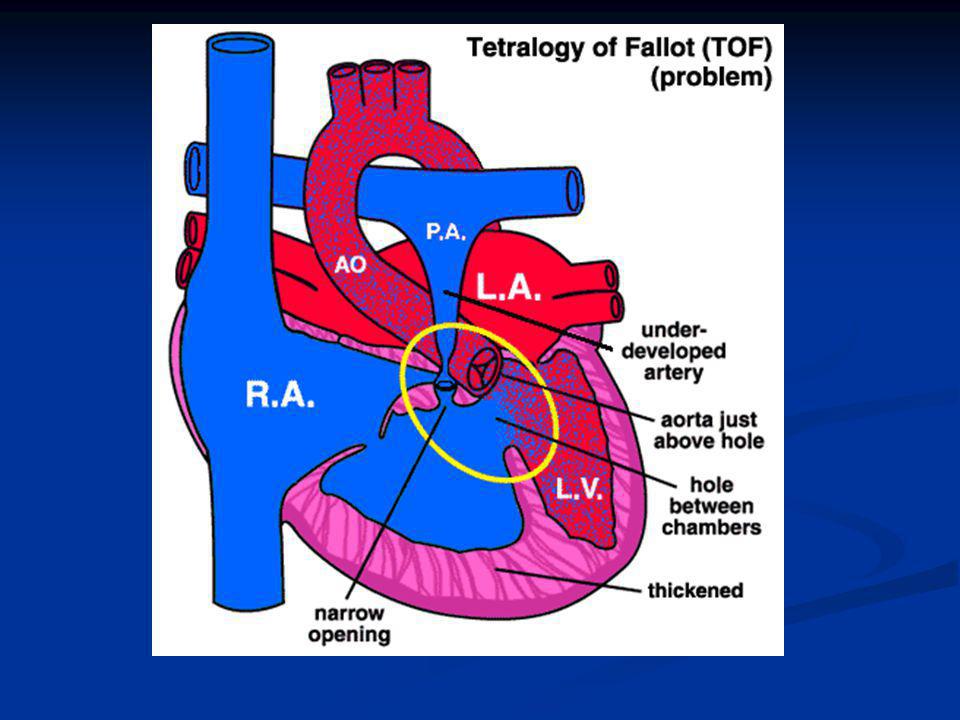
TOF Pulmonary stenosis (a narrowing of the blood vessel to the lungs)
Overriding aorta (the main blood vessel from the heart to the entire body is somewhat displaced) A ventricular septal defect (hole in the wall between the lower two chambers of the heart) Right ventricular hypertrophy (a thick muscle in the right pumping chamber)
 A ventricular septal defect (hole in the wall between the lower two chambers of the heart) Right ventricular hypertrophy (a thick muscle in the right pumping chamber)")
184
TOF First presentation may include poor feeding, fussiness, tachypnea, and agitation. Emergency Department Care: The ED physician should be able to recognize and treat a hypercyanotic episode as one of the very few pediatric cardiology emergencies that may present to the ED. Hypoxic tet spell: Hypercyanotic episodes are characterized by paroxysms of hyperpnea, prolonged crying, intense cyanosis, and decreased intensity of the murmur of pulmonic stenosis. Mechanism - Secondary to infundibular spasm and/or decreased SVR with increased right-to-left shunting at the VSD, resulting in diminished pulmonary blood flow If left untreated, may result in syncope, seizure, stroke, or death

185
Treatment for the acute setting of hypercyanosis includes the following:
Knee-chest position: Place the baby on the mother's shoulder with the knees tucked up underneath. This provides a calming effect, reduces systemic venous return, and increases SVR. Oxygen is of limited value since the primary abnormality is reduced pulmonary blood flow. Morphine sulfate, mg/kg IM/SC, may reduce the ventilatory drive and decrease systemic venous return. Phenylephrine, 0.02 mg/kg IV, is used to increase SVR. Treat acidosis with sodium bicarbonate, which may reduce the respiratory center stimulating effect of acidosis. General anesthesia is a last resort.

186
? Candida EBV CMV Diptheria No clue

187
Infectious mononucleosis
History: IM may have a varied clinical presentation, but the symptoms usually consist of fever, pharyngitis, and lymphadenopathy. The incubation period of IM is 4-6 weeks. Patients usually do not recall a history of possible exposure. Prodromal symptoms consisting of 1-2 weeks of fatigue, malaise, and myalgia are common In more than 90% of cases, IM is secondary to EBV infection

188
Infectious mononucleosis - Labs
Liver function tests (LFTs) are abnormal in more than 90% of patients with IM. Serum transaminase and alkaline phosphatase levels usually are modestly elevated. The serum bilirubin may be increased in approximately 40% of patients, but jaundice only occurs in approximately 5% of IM cases. CBC : differential that demonstrates greater than 50% lymphocytes, an absolute lymphocyte count greater than 4500, or an elevated lymphocyte count with greater than 10% atypical lymphocytes Also can have thrombocytosis Splenic rupture is a serious complication of IM, but it occurs in fewer than 0.5% of cases. More than 90% of splenic rupture cases occur in male patients.
 are abnormal in more than 90% of patients with IM. Serum transaminase and alkaline phosphatase levels usually are modestly elevated. The serum bilirubin may be increased in approximately 40% of patients, but jaundice only occurs in approximately 5% of IM cases. CBC : differential that demonstrates greater than 50% lymphocytes, an absolute lymphocyte count greater than 4500, or an elevated lymphocyte count with greater than 10% atypical lymphocytes. Also can have thrombocytosis. Splenic rupture is a serious complication of IM, but it occurs in fewer than 0.5% of cases. More than 90% of splenic rupture cases occur in male patients.")
189
?

190
Slipped Capital Femoral Epiphysis
The Limping Child Slipped Capital Femoral Epiphysis What is the red line called?

191
Slipped Capital Femoral Epiphysis
Klein’s line Superior femoral neck-lateral portion femoral head Mild widening, lucency, irregularity of physis Blurring of junction-metaphysis/physis (early)
")
196
Radiograph This is the radiograph taken of the patient.
Do you know the diagnosis?

197
Note in the AP pelvis on the left that the joint appears widened – this is a finding seen in septic arthritis (unlikely given the long time course of the pain) and Legg-Calvé-Perthes (LCP) disease. In LCP, the joint space widening represents increased soft tissue in the joint space. In the closeup of the same hip, note the crescent sign. The crescent sign results from the fact that the cortical rim or periosteum is nourished by the synovial fluid but the underlying cortical bone begins to collapse because of lack of blood supply to the area. The result is subcortical collapse, which forms a lucent crescent. These are the earliest findings of LCP disease.

198
Legg-Calvé-Perthes Disease
Avascular necrosis leading to collapse, fragmentation, and then reossification Most frequent between 4 and9 years Boys more often than girls Bilateral in 10% of cases LCP disease is an avascular necrosis of the femoral head, leading to collapse, fragmentation, and then finally a reossification process. It occurs most frequently in younger children (ages 4 to 9) but has been reported as early as 2 and as late as 13 years. Boys tend to get it more frequently than girls, and bilateral involvement, although not common, does occur.
 but has been reported as early as 2 and as late as 13 years. Boys tend to get it more frequently than girls, and bilateral involvement, although not common, does occur.")
199
Management - LCP Disease is self-limited – limp can last 2 to 4 years
Nonsteroidal anti-inflammatory agents Limit activities Crutches/braces occasionally needed May help maintain spherical femoral head Better outcomes in younger children This disease is generally a self-limited one but can last for several years, and thus supportive care is all that is generally required. The disease is a prolonged one, however, and the patient will need to be quite vigilant over the 2- to 4-year disease period. Generally pain control and limiting of activities are the recommended treatment course. Occasionally braces or crutches are recommended. The primary goal of treatment is to maintain the spherical shape to the femoral head until the reossification period takes place. The younger the child, the better the prognosis. Long-term studies reveal a higher incidence of osteoarthritis and total hip replacement much later in life.

200
?

201
Clinical Features: Your First Clue
Irritability Fever Erythema Limp/refusal to walk Decreased range of motion of limb To review, the clues to this diagnosis, particularly in the younger child, include irritability, fever (present in 50% of cases), redness overlying the joint, limp or refusal to walk, and decreased range of motion of the limb.
, redness overlying the joint, limp or refusal to walk, and decreased range of motion of the limb.")
202
Septic Arthritis of ankle

203
Management Once the diagnosis of septic joint is made, surgical intervention should proceed ASAP. Needle aspiration or open surgical drainage required Once the diagnosis is made, surgical intervention should proceed as soon as possible. Needle aspiration or open surgical drainage should be arranged, and antibiotics should be given immediately.

204
Synovial Fluid Findings
The synovial fluid of septic arthritis is often turbid or grossly purulent with a WBC greater than 40-50,000/mm3. Glucose in synovial fluid is often low, and protein and lactate are elevated.

205
Septic Arthritis Treatment by Age
The correct initial coverage should be for Staphylococcus aureus in the normal host, with broader coverage given to special patient populations such as the sickle cell population (Salmonella), the IV drug abuser (Methicillin-resistant S aureus), and the neonate (Group B strep and Gram-negative organisms).
, the IV drug abuser (Methicillin-resistant S aureus), and the neonate (Group B strep and Gram-negative organisms).")
207
Kerion This is a vigorous inflammatory reaction to dermatophyte infection, occasionally associated with secondary bacterial infection, that occurs on the scalp, resulting in a boggy inflammatory swelling Untreated tinea capitis

208
Dictation Gaffs and Goofs…
“Patient is a 3-year-old male who presents after a fall from a trampoline heart about an hour and half ago” “Patient presents to emergency department on orders from right ear CBS worker” “7-year-old male female presents to emergency department with complaints of pain or right ankle. Mom prospective about 57 concrete steps last night”

210
Oral thrush Signs and symptoms
Oral thrush usually produces creamy white lesions on your tongue and inner cheeks and sometimes on the roof of your mouth, gums and tonsils. The lesions, which resemble cottage cheese

213
Rubella/German Measles
Background: The name rubella is derived from a Latin term meaning "little red." Rubella is generally a benign communicable exanthematous disease. The major complication of rubella is its teratogenic effects when pregnant women contract the disease, especially in the early weeks of gestation. The virus can be transmitted to the fetus through the placenta and is capable of causing serious congenital defects, abortions, and stillbirths

214
Rubella Incubation period: The incubation is usually days after exposure to a person with rubella. Prodromal phase: Prodromal symptoms are unusual in young children but are common in adolescents and adults.

215
Rubella The following signs and symptoms usually appear 1-5 days before the onset of rash: Eye pain on lateral and upward eye movement (a particularly troublesome complaint) Conjunctivitis Sore throat Headache General body aches Low-grade fever Chills Anorexia Nausea Tender lymphadenopathy
 Conjunctivitis. Sore throat. Headache. General body aches. Low-grade fever. Chills. Anorexia. Nausea. Tender lymphadenopathy.")
217
Sturge-Weber Syndrome
Sturge-Weber syndrome is a neurological disorder indicated at birth by seizures accompanied by a large port-wine stain birthmark on the forehead and upper eyelid of one side of the face. Some children will have developmental delays and mental retardation; most will have glaucoma (increased pressure within the eye) at birth or developing later. “Port wine stain”
 at birth or developing later. Port wine stain")
218
Peds GCS/EMV - ? 1 year old, MVC, cries during exam, opens eyes spontaneously when saying Dr says name, localizes pain but not following commands 15 14 13 12 11 10 No clue

219
1 year old, MVC, cries during exam = 3 or 4 1. opens eyes spontaneously = 4 localizes pain but not following commands = 5 Total = 12 or 13

220
Modified Pediatric Glasgow Coma Scale
Eye Opening 4 Spontaneously 3 To voice 2 To pain 1 No response Verbal Response 5 Appropriate words, spontaneous cooing 4 Inappropriate words 3 Cries 2 Incomprehensible sounds, grunts Motor Response 6 Obeys 5 Localizes pain 4 Flexion withdrawal 3 Flexion abnormal (decorticate posturing) 2 Extension (decerebrate posturing) 1 No response 220
 2 Extension (decerebrate posturing) 1 No response")
221
Peds ICI/BHT Found significant ICI is unlikely in a child who does not exhibit at least 1 of the high-risk criteria Evidence of significant skull fx Altered level of alertness Neuro deficit Persistent vomiting Scalp hematoma Abnl behavior coagulopathy

222
Symptoms and Signs of Concussion
Headache Dizziness Depression Confusion Nausea/vomiting Sensitivity to light or noise Anxiety Poor memory Lethargy Slow response to questions Decreased energy Irritability Blurred or double vision Poor concentration Poor balance Insomnia

223
Table 2. Recommendations for Return to Sports after Head Injury Based on Grade of Concussion
Severity Symptoms Management Grade 1 (Mild) No LOC, ringing, headache, dizziness, or memory loss Observation May not return to competition until symptom-free upon exertion Grade 2 (Moderate) LOC <5 min or PTA >30 min Observation May not return to competition for 1 wk after symptom-free upon exertion Grade 3 (Severe) LOC >5 min or PTA >24 h Admit Refer for neurocognitive testing prior to resumption of contact sports LOC=loss of consciousness; PTA=posttraumatic amnesia
 No LOC, ringing, headache, dizziness, or memory loss. Observation May not return to competition until symptom-free upon exertion. Grade 2 (Moderate) LOC <5 min or PTA >30 min. Observation May not return to competition for 1 wk after symptom-free upon exertion. Grade 3 (Severe) LOC >5 min or PTA >24 h. Admit Refer for neurocognitive testing prior to resumption of contact sports. LOC=loss of consciousness; PTA=posttraumatic amnesia.")
226
Eczema / Atopic Dermatitis

227
The most common surgical cause of vomiting in infancy is
a. Intestinal atresias b. Malrotation c. Pyloric stenosis d. Meconium ileus

230
Pyloric Stenosis Pathophysiology: Marked hypertrophy and hyperplasia of the 2 (circular and longitudinal) muscular layers of the pylorus occurs, leading to narrowing of the gastric antrum. Frequency: In the US: The incidence of IHPS is 2-4 per 1000 live births Sex: IHPS has a male-to-female predominance of 4:1, with 30% of patients with IHPS being first-born males Age: The usual age of presentation is approximately 3 weeks of life (1-18 wk). History: Classically, the infant will have nonbilious vomiting or regurgitation, which may become projectile (up to 70%), after which the infant is still hungry. Emesis may be intermittent or occur after each feeding
 muscular layers of the pylorus occurs, leading to narrowing of the gastric antrum. Frequency: In the US: The incidence of IHPS is 2-4 per 1000 live births. Sex: IHPS has a male-to-female predominance of 4:1, with 30% of patients with IHPS being first-born males. Age: The usual age of presentation is approximately 3 weeks of life (1-18 wk). History: Classically, the infant will have nonbilious vomiting or regurgitation, which may become projectile (up to 70%), after which the infant is still hungry. Emesis may be intermittent or occur after each feeding.")
231
Branchial cleft remnants present most commonly as a(n)?
a. pain airway obstruction intraoral mass d. infection

233
Pediatric Cardiopulmonary Arrests
10% 10% If asystolic, mortality > 90% 80%

234
Age distribution of arrests
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 <7 mos 7-12 mos Age (years)
")
235
Arrive in ER in cardiac arrest (N = 80) Admit PICU (N=43) 54 %
Died in ER (N=37) 46% Mod Deficit (N=3) PVS at 12 mos (N=2) Dead at 12 mos (N=1) Died in ICU (N=37) 46% Schindler M, et al. Outcome of out-of-hospital cardiac or respiratory arrest in children. N Engl J Med 1996;335: 4
 46% Mod Deficit. (N=3) PVS at. 12 mos. (N=2) Dead at. 12 mos. (N=1) Died in ICU. (N=37) 46% Schindler M, et al. Outcome of out-of-hospital cardiac or respiratory arrest in children. N Engl J Med 1996;335:")
236
List at least 10 signs of pediatric Respiratory distress

237
Signs of Respiratory Distress
Tachypnea Tachycardia Grunting Stridor Head bobbing Flaring Inability to lie down Agitation Retractions Access muscles Wheezing Sweating Prolonged expiration Pulsus paradoxus Apnea Cyanosis 15

238
List signs of impending respiratory failure

239
Impending Respiratory Failure
Reduced air entry Severe work Cyanosis despite O2 Irregular breathing / apnea Altered Consciousness Diaphoresis

240
Bruising from abuse Petechial rash Mongolian spots HSP No clue
The photo on the left is a child with many mongolian spots. The right is a child after sustaining “coining” in an attempt to alleviate his illness.

241
Specificity of Fractures for Abuse
High specificity Metaphyseal Posterior rib Scapula Spinous process Sternal Moderate specificity Multiple fractures Fractures of diff. age Epiphyseal Vertebral body Digital Complex skull Low specificity Clavicle Long bone shaft Linear skull

242
Radiographic Dating of Injuries
Soft tissue findings Early 2-5d Peak 4-10d Late 10-21d Periosteal new bone 10-14d 14-21d Loss of Fx line; soft callus Hard callus 21-42d 42-90d Remodeling 3 mos 1 yr 2 yr Peds Clin NA 1996

248

253
Candidiasis -Signs and symptoms
Oral thrush usually produces creamy white lesions on your tongue and inner cheeks and sometimes on the roof of your mouth, gums and tonsils. The lesions, which resemble cottage cheese Nyastatin - works by contact! Perineal/diaper rash candidiasis antifungal cream Keep dry and open to air

255
Speed Round Rashes Go Interns!!
Name the rash and everything you know about it Cause Treatment Prevention

263
Question #1 A 1-week-old infant presents for his first newborn evaluation. He had been discharged apparently well and thriving at 48 hours of age. He now exhibits grouped vesicles on an erythematous base that were not present at birth. Wright stain of scrapings from the floor of the vesicles reveals multinucleated giant cells and balloon cells. Of the following, the MOST likely diagnosis is: A) bullous impetigo B) congenital varicella C) herpes simplex virus infection D) incontinentia pigmenti E) recessive dystrophic epidermolysis bullosa
 bullous impetigo. B) congenital varicella. C) herpes simplex virus infection. D) incontinentia pigmenti. E) recessive dystrophic epidermolysis bullosa.")
264
Skin Lesions (photos: University of California, Australian Herpes Management Forum, and eMedicine)
")
Similar presentations













































































 Lawrence Pike.>")


















 Disease (strep throat, necrotizing fasciitis, impetigo) By: Dr. Awatif Alam.>")