Download presentation
Presentation is loading. Please wait.

1
PLME Science Curriculum
Julianne Ip, MD Associate Dean of Medicine (PLME and VIMS) Clinical Associate Professor of Family Medicine Alpert Medical School Brown University
 Clinical Associate Professor of Family Medicine. Alpert Medical School. Brown University.")
2
How will we go from college freshmen
The PLME class of 2008

3
To MD graduates of the Alpert Medical School of Brown University 2012
4 years later….they comprise half the graduating MD class To MD graduates of the Alpert Medical School of Brown University 2012

4
Overload of facts and information, fatigue, loss of compassion and passion for learning, and humanity 50% of what we learn in medical school is “wrong” or has changed by the time we are ready to be residents… As a former dean of mine also said…we forget the other half by the time we graduate as well…

5
HHMI-AAMC report knowledge revises our understanding of sciences
concerns about increasingly rapid rate at which new knowledge revises our understanding of sciences fundamental to medicine Importance of educating future physicians to be “inquisitive” To help them build a strong scientific FOUNDATION… but not overwhelm them with “facts” To equip them with the knowledge, skills and habits to integrate new scientific discovery into their medical practice throughout their lives…

6
Brown’s Baccalaureate-MD program is poised to be a pilot for changes in pre-medical education. We set the admissions standards and competencies required for our curriculum. How many of the BAC-MD programs here have “control” over their admissions requirements?

7
The Warren Alpert Medical School of Brown University
With the addition of the Standard Admissions route providing half of each MD class, there was a concomitant change in the first two years of basic pre-clinical sciences. The emphasis on an integrated curriculum took away the option for PLMEs to 1) take medical school courses early 2. take a reduced load taking 3 years to complete the usual 2 first two years. Similarly there was a shift in emphasis and importance to the US News and World Report rankings and faculty support for AOA. Our first change was to increase the biology competency from one “Foundations of Biology” course, which at least 80% of our freshmen have placed out of, to include a total of 3 biology competencies. There is a list of biology courses from which the students must chose including: Physiology, Cell and Molecular Biology, Vertebrate Embryology, Genetics, Biochemistry, Comparative Vertebrate Anatomy, Microbiology, Developmental Biology and Evolutionary Biology. The only GPA “requirement” of the PLME is that each of the 3 biology courses must be taken for a grade and the student must receive a B or better. Antedotel comparisons between standard and PLMEs has them comparable in performance in the first two years of med school. The Warren Alpert Medical School of Brown University
 take medical school courses early 2. take a reduced load taking 3 years to complete the usual 2 first two years. Similarly there was a shift in emphasis and importance to the US News and World Report rankings and faculty support for AOA. Our first change was to increase the biology competency from one Foundations of Biology course, which at least 80% of our freshmen have placed out of, to include a total of 3 biology competencies. There is a list of biology courses from which the students must chose including: Physiology, Cell and Molecular Biology, Vertebrate Embryology, Genetics, Biochemistry, Comparative Vertebrate Anatomy, Microbiology, Developmental Biology and Evolutionary Biology. The only GPA requirement of the PLME is that each of the 3 biology courses must be taken for a grade and the student must receive a B or better. Antedotel comparisons between standard and PLMEs has them comparable in performance in the first two years of med school. The Warren Alpert Medical School of Brown University.")
8
Basically, assist and teach extremely bright, intelligent, motivated young men and women the skills and fuel their passion to be LIFE-LONG LEARNERS, to practice science-based medicine with greater synergy and efficiency along the continuum of their premedical and medical education.

9
PLME versus Standard Pre-Med
PRE-MED Requirements PLME COMPETENCIES Biology-three semesters (most place out of intro level so have 2 semesters) Inorganic Chemistry-one semester Organic Chemistry-one semester Physics-2 semesters Calculus-one semester (most place out) Humanities/Social Science ( 2 writing courses) No MCATS Biology-2 semesters Inorganic Chemistry-2 semesters Organic Chemistry-2 semesters Physics-2 semesters Calculus-generally 1 semester minimum English-2 semesters MCATS BIG CHANGES coming to pre-medical education. With all the knowledge that is out there learning to think critically, problem solve and apply knowledge is the key now. Less reliance on “courses” but rather interdisciplinary approaches to pre-medical education. Biochemistry will be increasingly important- Social and Behavioral medicine and the “context” of what you are learning.
 Inorganic Chemistry-one semester. Organic Chemistry-one semester. Physics-2 semesters. Calculus-one semester (most place out) Humanities/Social Science ( 2 writing courses) No MCATS. Biology-2 semesters. Inorganic Chemistry-2 semesters. Organic Chemistry-2 semesters. Physics-2 semesters. Calculus-generally 1 semester minimum. English-2 semesters. MCATS. BIG CHANGES coming to pre-medical education. With all the knowledge that is out there learning to think critically, problem solve and apply knowledge is the key now. Less reliance on courses but rather interdisciplinary approaches to pre-medical education. Biochemistry will be increasingly important- Social and Behavioral medicine and the context of what you are learning.")
10
We start with our end product--our Brown MD graduate. What does it take?
Our graduates must be ready to be outstanding residents and future physicians therefore they must be outstanding 3rd- and 4th- year med students Our first- and second-year med students must be prepared for clinical clerkships, clinical electives and decisions about future professional career Therefore, our PLMEs must be prepared for first- and second-year integrated basic medical sciences and the Doctoring course So, why did we decide to consider more changes? Chemistry courses at Brown are notorious for being self appointed gatekeepers. The physics department is better but the underlying premise is that the courses are to prepare or introduce the students to Chemistry or Physics as a potential concentration, not prepare them for medical school. Given the explosion in what students need to learn, this did not seem to be the best use of their education. Couple this with the national discussion about changing MCATs and the HHMI-AAMC report and Brown saw an opportunity to be innovatibve.

11
Initial Proposal Two semester freshmen/sophomore course; integrate Chemistry, Physics, Math pertaining to biological and medical sciences Senior year one semester capstone course: interdisciplinary, integrative case-based promoting a holistic view of the human condition. Emphasis on: - Self-directed learning - Small group learning - Incorporation of ethics, history of medicine, new technology particularly as it pertains to the humanistic aspects of patient care

12
PLME Science/Behavioral –Social Science and Humanities curriculum committee
Associate Dean of Medical Education Director of First and Second year Basic Science Curriculum (eventually the second year assistant director took over) A Cogut Fellow in the Humanities (funded by the Medical School to oversee the writing and development of the curriculum) Associate Dean of the College (for sciences) Associate Dean of Medicine (PLME)
 A Cogut Fellow in the Humanities (funded by the Medical School to oversee the writing and development of the curriculum) Associate Dean of the College (for sciences) Associate Dean of Medicine (PLME)")
13
Contributing Groups PLME Alumni Survey and Focus Group
PLME advising deans Alpert Medical School students survey and focus group PLME survey and focus group Wayland Collegium College funded think tank group Picks one topic/semester Interdisciplinary: included physics, math, biostats, chemistry (both inorganic and organic) and biology faculty Tried to engage the University particularly the Chemists and Physicists through the Wayland Collegium. It was singularly unsuccessful…
 and biology faculty. Tried to engage the University particularly the Chemists and Physicists through the Wayland Collegium. It was singularly unsuccessful…")
14
CHALLENGES At any institution: who will pay and turf wars
Had one year “Wayland Collegium” with representatives from chemistry, physics, math, epi/stats and biology. There was no resolution primarily because of the way the departments are financed and graduate students funded so we could not get buy in from the College. The medical school decided to move ahead and since the PLME is funded by the medical school, this has been feasible.

15
Alpert Medical School takes ownership
Alpert Medical School takes ownership. Uses the HHMI-Scientific Foundations as template. So, we took it on ourselves…

16
White Paper Created a white paper outlining the pedagogical underpinnings of the endeavor

17
PLME 1000 Senior Seminar in Scientific Medicine
This course is an interdisciplinary and integrative science course that will supplement the preparation of both PLME and premedical students for the study of medicine in the 21st century. The course will use a case-based approach to relevant and contemporary subjects in medicine and health care, such as biological systems and their interactions, mechanisms of intra- and intercellular communication, drug therapy optimization, and humanistic aspects of patient care. This course is intended for seniors interested in attending medical school, but will preferentially enroll students in the PLME. This is an S/NC course. Started with the Capstone. Given we worked with the Directors of the first and second year medical school curriculum group, we were able to create a syllabus that we believe will prepare our students for our medical school. Note, that the first cohort, the current PLME senior class, has had 1 semester of inorganic chem, 1 of organic chem, 2 semesters of physics and the one semester of calculus. I am the course leader. It gives me a unique opportunity to get to know almost all the PLME seniors.

18
Assessments Quizzes % You will be a given a brief, five question quiz prior to the beginning of lecture each week. The quizzes will be based on your reading assignment for the week. Participation (class and small group) 10% This class and the learning you will be doing are structured around small group problem-based learning and class discussion. We are looking for thoughtful contributions that refer directly to the readings and lectures at hand. Reflective Narratives % You will be asked to write three reflective narratives during the course. These narratives should be one page in length, single spaced and be in response to topics presented in the course. Prompts for these narratives will be given in class. The due dates of the narratives are: October 15th November 5th December 3rd Midterm Exam 25% The midterm examination will mainly be comprised of single best answer, multiple choice questions but may also contain other questions types (true/false, fill in the blank and essay type questions). Questions on the midterm examination will be drawn from lecture, small group discussions, large group discussions and the readings. Final Exam *same as midterm 35% The exams are specifically Multiple Choice single best answer and actually we use the same scantron bubble sheets as the Medical School. I bring in our learning specialist, who works with not only the PLMEs but also the medical students, to speak during my first presentation. This takes away any stigma of referring any of these students to learn test taking skills, time management skills, test anxiety techniques and even helps identify students with differences in learning style.
 10% This class and the learning you will be doing are structured around small group problem-based learning and class discussion. We are looking for thoughtful contributions that refer directly to the readings and lectures at hand. Reflective Narratives 20% You will be asked to write three reflective narratives during the course. These narratives should be one page in length, single spaced and be in response to topics presented in the course. Prompts for these narratives will be given in class. The due dates of the narratives are: October 15th. November 5th. December 3rd. Midterm Exam 25% The midterm examination will mainly be comprised of single best answer, multiple choice questions but may also contain other questions types (true/false, fill in the blank and essay type questions). Questions on the midterm examination will be drawn from lecture, small group discussions, large group discussions and the readings. Final Exam *same as midterm 35% The exams are specifically Multiple Choice single best answer and actually we use the same scantron bubble sheets as the Medical School. I bring in our learning specialist, who works with not only the PLMEs but also the medical students, to speak during my first presentation. This takes away any stigma of referring any of these students to learn test taking skills, time management skills, test anxiety techniques and even helps identify students with differences in learning style.")
19
Teaching Assistants: There are six teaching assistants for this course. Each student will be assigned one of these teaching assistants for small group work. TA’s are second-year medical students with an interest in medical education; generally are participating in the Teaching Academy and Scholarly Concentration in Medical Education The Teaching Assistants are vital to this course. Each of them took one of the sections and became to “Guru”…they helped develop the multiple choice questions for the quizzes and exams as well as prepared facilitator guides for small group discussion. As noted, they are members of the teaching academy (provide tutoring for medical students and PLMEs) and most are in the Scholarly Concentration in Med Ed.
 and most are in the Scholarly Concentration in Med Ed.")
20
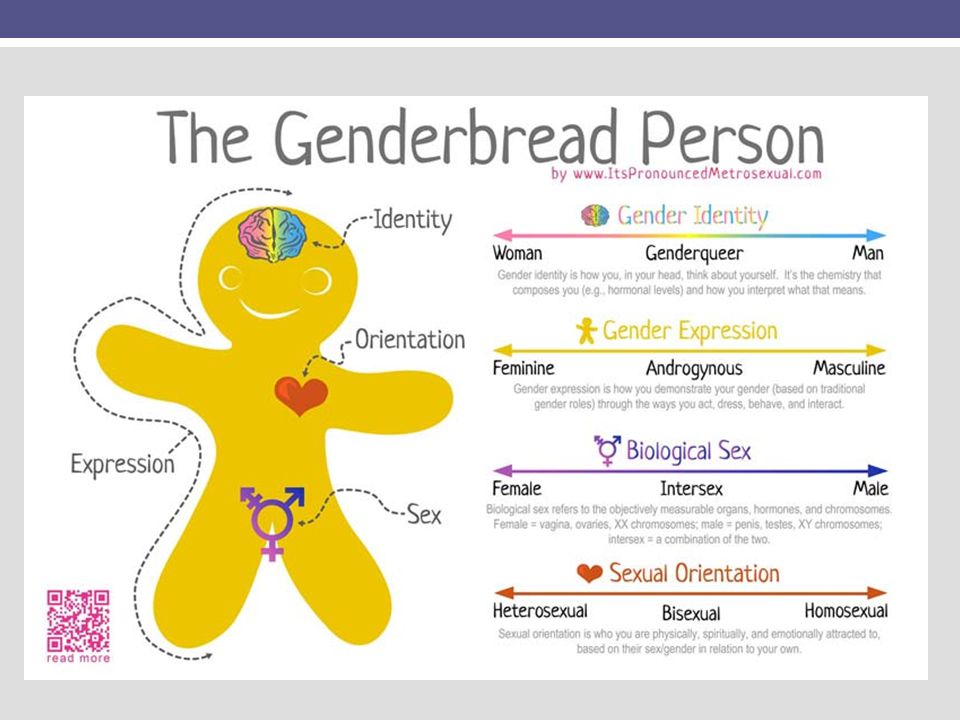
First three weeks of course we start with sex…
Objectives: Describe the molecular biology of androgen insensitivity. Compare and contrast the phenotypic variation seen in androgen insensitivity. Describe the medical management of differences of sex development. Construct an argument for the postponement of surgical management of differences of sex development using ethical principles. Let me walk you through the first 3 weeks of the syllabus…

21
Readings: Jääskeläinen J. Molecular biology of androgen insensitivity. Molecular and Cellular Endocrinology. In press. Wiesemann C, Ude-Koeller, Sinnecker GHG, Thyen U. Ethical principles and recommendations for the medical management of differences of sex development (DSD)/intersex in children and adolescents. Eur J Pediatr (2010) 169: 671–679. Dreger, A; Chase, C; Souza, A; Gruppuso, P. Frader J: Changing the Nomenclature/Taxomony for Intersex; A Scientific and Clinical Rationale. J Ped Endocrinology and Metabolism (2005) Phornphutkul, C; Fausto-Sterling, A; Gruppsuo, P: Experience and Reason Pediatrics Vol 106 No Hines, M. Sex-related variation in human behavior and the brain Trends in Cognitive Science Vol 14 no Students read up to date scientific articles and the quiz questions come from the readings. The quizzes are posted 4 days before the class which covers the material. The students take the quiz online, CANVAS and submit answers before the class.
/intersex in children and adolescents. Eur J Pediatr (2010) 169: 671–679. Dreger, A; Chase, C; Souza, A; Gruppuso, P. Frader J: Changing the Nomenclature/Taxomony for Intersex; A Scientific and Clinical Rationale. J Ped Endocrinology and Metabolism (2005) Phornphutkul, C; Fausto-Sterling, A; Gruppsuo, P: Experience and Reason Pediatrics Vol 106 No Hines, M. Sex-related variation in human behavior and the brain Trends in Cognitive Science Vol 14 no Students read up to date scientific articles and the quiz questions come from the readings. The quizzes are posted 4 days before the class which covers the material. The students take the quiz online, CANVAS and submit answers before the class.")
22
Quiz on Readings (Ip; 10 minutes)
Monday, September 10th: Session #1 Quiz on Readings (Ip; 10 minutes) Lecture on Androgen insensitivity (Gruppuso, 70 minutes) Wednesday, September 12th: Session #2 Case-based vignettes on diagnosis and treatment of androgen insensitivity (Forcier, 40 minutes) Discussion of the ethics of medical management of sex differentiation (Small Groups, 40 minutes) We spend 10 minutes reviewing the quiz. Then, a faculty member gives a lecture. The faculty has reviewed the articles and often has proposed the articles that the students read. Generally, the first lecture of the week, Monday, is the “science”…includes basic biochem, physics, math or stats as relevant. Students ask questions based on the readings and integrate it with the lecttures.
 Lecture on Androgen insensitivity (Gruppuso, 70 minutes) Wednesday, September 12th: Session #2 Case-based vignettes on diagnosis and treatment of androgen insensitivity (Forcier, 40 minutes) Discussion of the ethics of medical management of sex differentiation (Small Groups, 40 minutes) We spend 10 minutes reviewing the quiz. Then, a faculty member gives a lecture. The faculty has reviewed the articles and often has proposed the articles that the students read. Generally, the first lecture of the week, Monday, is the science …includes basic biochem, physics, math or stats as relevant. Students ask questions based on the readings and integrate it with the lecttures.")
23
Complete Androgen Insensitivity (Testicular Feminization Syndrome)
SRC Mutation in AR gene affecting androgen binding to AR or AR binding to DNA. X-linked recessive disorder, expressed in 46,XY individuals only Mutation in the Androgen Receptor gene Manifests as a disorder of sexual differentiation Breast development and female habitus at puberty; primary amenorrhea; scant or absent pubic and axillary hair Genitalia: female with blind vaginal pouch Wolffian derivatives: usually absent Mullerian derivatives: absent or vestigial Gonads: testes Expectation is that the students understand the molecular biology, genetics, basic anatomy and physiology

24
Steroid Hormone Biosynthesis
7-dehydrocholesterol cholesterol cortisol progesterone aldosterone androstenedione estrone testosterone estradiol Gonads Target tissues 5a-dihydrotestosterone

25
Awareness of Gender Identity
Between ages 1 and 2— Children become conscious of physical differences between sexes At 3 years old— Can label themselves as girl or boy The second lecture of the week brings in the more clinical aspects…behavioral and social science and often the ethical issues facing a physician. By age 4 Gender identity is stable, for many/most Recognize that gender is constant

27
Small group discussion…TA Guru
What is sex? What is gender? Who defines them? Are they binaries? How much does culture play a role in gender? Does it at all? Are there differences across countries/regions? Does sex determine gender? How much does nature play a role in gender? How about nurture? Greenspan seems to suggest at the end of the reading that androgens may play a role in gender identification—do you agree? Where do individuals with DSD fall? How much does gender define you? Is it a large part of your identity? Do you feel you fall into the gender binary? How do we understand individuals that don’t quite fit into the gender binary (ie tomboys)? Is there a stigma associated with not conforming to your culturally expected gender? Does it differ for males and females? (ie is it worse to be a feminine guy or a masculine girl? Does this influence how you think of DSD individuals or what you would recommend to them? This is a sample of the detail that is covered in the small group discussions
 Is there a stigma associated with not conforming to your culturally expected gender Does it differ for males and females (ie is it worse to be a feminine guy or a masculine girl Does this influence how you think of DSD individuals or what you would recommend to them This is a sample of the detail that is covered in the small group discussions.")
28
Week 2-Evidenced-based medicine; biostatistics learning the terms
To get everyone at the same level in reading the primary literature, we gave 2 weeks of evidence based medicine and biostatistics…didn’t start with it or the students might have all left the class but they really engaged with this given how we started with …sex.

29
Biostatistics: group problem solving
In a population of 1000 women, 250 are on tamoxifen to prevent breast cancer. 25 of the women on tamoxifen develop breast cancer. Of the 750 women not on tamoxifen, 200 develop breast cancer. What is the number needed to treat with tamoxifen to prevent one case of breast cancer? (Outcome +) +Breast Cancer (Outcome -) - Breast Cancer (Exposure +) +Tamoxifen A=25 B=225 (Exposure –) - Tamoxifen C=200 D=550 Understanding the use of terms and biostats in a clinical application was key. Risk of developing breast cancer on Tamoxifen: 25/250 Risk of developing breast cancer not on Tamoxifen: 200/750 Absolute risk reduction = 25/250 – 200/750 NNT = 1/ARR = 5.88 (round up to 6)
 +Breast Cancer. (Outcome -) - Breast Cancer. (Exposure +) +Tamoxifen. A=25. B=225. (Exposure –) - Tamoxifen. C=200. D=550. Understanding the use of terms and biostats in a clinical application was key. Risk of developing breast cancer on Tamoxifen: 25/250. Risk of developing breast cancer not on Tamoxifen: 200/750. Absolute risk reduction = 25/250 – 200/750. NNT = 1/ARR = 5.88 (round up to 6)")
30
Breast Cancer Screening and Overview of Breast Cancer: Goals
Review current guidelines for breast cancer screening, including screening of high risk patients with MRI Highlight controversy surrounding screening mammography Overview of the management of malignant breast diseases Identify who and how to screen for familial breast and gynecologic cancers We then moved onto areas where knowledge required thought and application….so, controversy and how to approach this as a future physician

31
Mammography, when to start?
Sensitivity: 77%-95% Specificity: 94%-97% Seven statistical models showed screening mammography reduces the rate of death from breast cancer by 7 to 23 percent, with a median of 15 percent. Meta-analysis of 8 randomized trials Reduction of rate of death for women > 40 y Reduction of mortality by 15 to 20% for ages 40 to 49 yr Reduction of mortality by 16 to 35% for ages 50 to 69 yr NB: Results reported for women ‘invited to screen’. Advocates suggest women ‘actually screened’ probably benefit even more. The students immediately noted the use of the biostats that they just learned and now “interpretation” of the data is not black and white.

32
Standard Mammography views; Cranio-caudal and Midline Oblique
The physician lecturer pointed out the technology behind the use of X-ray mammography and tied it into physics…

33
Screening Guidelines In USA, most recommend screening at 40 years
Between years: ACS: annually ACR: annually ACOG: every 1-2 years NCI: every 1-2 years USP-STF (2009): not recommended Canadian Task Force on Preventive Health Care: not recommended Annual screening > 50 years: Most organizations USP-STF (2009): every 1-2 years Discussion centered on the differences in guidelines…what would YOU future physician do???
: not recommended. Canadian Task Force on Preventive Health Care: not recommended. Annual screening > 50 years: Most organizations. USP-STF (2009): every 1-2 years. Discussion centered on the differences in guidelines…what would YOU future physician do")
34
Sample Midterm Multiple Choice Question
Choose single best answer; bubble into scantron sheet A new patient, a 28 year old single female comes to your office for a first time physical. She is otherwise healthy and has no risk factors for any illness including a negative family history for cancer, cardiovascular disease, hypertension or any other major illness. She asks you about her chances of developing breast cancer over her lifetime. You tell her that: A:Every patient is different so you cannot answer B:One in eight women will develop breast cancer C:One in every one hundred women has breast cancer D:Given she has no risk factors she will not develop breast cancer Exam questions try to emulate first and second year med school exams and give the PLMEs a taste of USMLE. Given the PLME does not require MCATS, there is a long span between SAT/ACTs and the first high stakes USMLE exam.

35
Narrative Reflection Prompts
You are a primary care physician who is part of the new system of "capitation" on your group practice mandated by the changes after the election of 2012 in the "New" Affordable Health Plan. This capitation is similar to the United Kingdom system of having a set amount of funds to care for all your patients; so no matter what tests, procedures or exams you perform on your panel of patients, this is ALL the funds you will have. You receive $1,000,000 for the care of your 2500 patient panel, all ages. One of your patients is a 27 year man who gets convicted of first degree murder and is incarcerated for life (no parole). He needs a liver transplant. This transplant will cost $350,000 of your funds which will leave far less to care for the rest of your patients. Do you put the patient on the transplant list? Why or why not? What if you have an active 80 year old who is still functioning at full capacity; he volunteers at the local school tutoring science and works out by running 1 mile per day. He has a wife who is healthy and 3 healthy children and 4 grandchildren who he often takes care of on a regular basis. He needs a liver transplant. This will cost $350,000 of your funds as well. Do you put him on the transplant list? Why or why not? What if you had to CHOOSE between the two patients (given your limited funding)...how might you make this decision? If you HAD to choose one person, which would you choose and why? Reflections mirror our Doctoring reflections asking students to consider their own values in considering issues. The TAs and I read and send back questions to hopefully get the students to think deeper. No right or wrong…just delving into the role of a future physician.
. He needs a liver transplant. This transplant will cost $350,000 of your funds which will leave far less to care for the rest of your patients. Do you put the patient on the transplant list Why or why not What if you have an active 80 year old who is still functioning at full capacity; he volunteers at the local school tutoring science and works out by running 1 mile per day. He has a wife who is healthy and 3 healthy children and 4 grandchildren who he often takes care of on a regular basis. He needs a liver transplant. This will cost $350,000 of your funds as well. Do you put him on the transplant list Why or why not What if you had to CHOOSE between the two patients (given your limited funding)...how might you make this decision If you HAD to choose one person, which would you choose and why Reflections mirror our Doctoring reflections asking students to consider their own values in considering issues. The TAs and I read and send back questions to hopefully get the students to think deeper. No right or wrong…just delving into the role of a future physician.")
36
Chronic Renal Disease Renal Transplantation
Autism and Vaccines Pharmacology and Toxicology In the 13 week semester, we will end up covering these topics in addition to those mentioned before. Prostate Cancer Clinical Arts and Humanities Health Care Financing: US and International

37
Next Steps Goals for the Redesigned PLME Year 1 Courses
Focus on the scientific competencies as detailed in the AAMC-HHMI report. Develop interdisciplinary science courses that more effectively engage students interested in a career in medicine. Integrate the sciences and non-science disciplines. An example is the incorporation of ethics or history of science into any discussion of new technologies. Another example is an emphasis on the humanistic aspects of patient care whenever discussing application of new knowledge or technology. Incorporate an inquiry-based approach into premed education. Enhance the ability of all PLME’s to succeed in medical school, but especially members of underrepresented groups. Members of underrepresented groups typically fare worse in the courses listed above. The integrated courses will include periodic exams and regularly scheduled tutorials for students who need help. Now the “harder” part…redesigning the freshmen/sophomore sequence to “replace” the traditional chemistry, math and physics requirement.

38
PLME Freshman Course Sample Teaching Module
Overall Strategy: Central topic, a young boy with hereditary fructose intolerance, a disorder of fructose metabolism that results from a mutation in the gene that encodes the enzyme, Aldolase B. The proposed strategy is to use this case study as a means to address basic concepts in quantitative reasoning, physics and chemistry through an emphasis on enzyme catalysis. Again, use cases.

39
Case Presentation: Danny, a 3 year old boy was brought in for evaluation of failure to thrive (poor growth and weight gain). His medical history included a profound aversion for sweet foods. In fact, it was described that he would retch when offered candy, other sweets, fruit juice, or fruit. Once, after drinking fruit juice, he vomited and had a near loss of consciousness for a short period of time. Based on this history, a it was suspected that Danny had hereditary fructose intolerance. This is a disorder that is inherited because it is due to a mutation in an enzyme. The enzyme, aldolase B, is involved in the metabolism of the dietary sugar, fructose. To confirm the diagnosis, Danny was admitted to the hospital and given an oral fructose load. During the test, he became sleepy and had a low blood sugar. Laboratory tests confirmed the diagnosis. Note the bolded terms…these are the key concepts that will be addressed in class.

40
Background Biology What is fructose? (Discuss the major nutrients - carbohydrate, protein and fat - and the major dietary carbohydrates - glucose, fructose, sucrose, galactose and lactose) What is an enzyme? (Discuss the concept of catalysis) What is a mutation? (Review the central paradigm: DNA to RNA to protein)
 What is an enzyme (Discuss the concept of catalysis) What is a mutation (Review the central paradigm: DNA to RNA to protein)")
41
Working with the Inorganic and Organic Chemists particularly as the material relates to biochemistry…how much do the students “need?” Chemistry as “gatekeepers” to medical school? Links to Important Principles in Chemistry and Physics: Chemistry Principles involved (pending review) Organic Molecule Structure (connectivity, shape, conformation - e.g., why are glucose and galactose different molecules? Can they interconvert? What about fructose and glucose?) Metabolism = chemical reactions of nutrients Kinetics - why are the adverse effects short lived as opposed to permanent? Since the National Chemistry Association published their report stating that even the chemists have to address the changes in pre-medical and basic chemistry teaching…and in conjunction with the “buy-in” we have from the Dean of the College, our new Provost and already our President, our committee includes a physicist and a chemist.
 Organic Molecule Structure (connectivity, shape, conformation - e.g., why are glucose and galactose different molecules Can they interconvert What about fructose and glucose ) Metabolism = chemical reactions of nutrients. Kinetics - why are the adverse effects short lived as opposed to permanent Since the National Chemistry Association published their report stating that even the chemists have to address the changes in pre-medical and basic chemistry teaching…and in conjunction with the buy-in we have from the Dean of the College, our new Provost and already our President, our committee includes a physicist and a chemist.")
42
Working with the General Physics professors on these cases
Working with the General Physics professors on these cases. How much is “enough?” Their opinion or ours? Physics principles involved (pending review) Coulomb’s law Electric fields and potentials Electric dipoles Dielectrics and solubility Torque Newton’s Laws Energy Conservation
 Coulomb’s law. Electric fields and potentials. Electric dipoles. Dielectrics and solubility. Torque. Newton’s Laws. Energy Conservation.")
43
Work in Progress…Questions??? Thank you

Similar presentations