Download presentation
Presentation is loading. Please wait.

1
Advanced Directives: Thinking and Talking About the Hard Stuff ~

2
People live longer, die differently
In 1900, average longevity in US was 49.2 years In 2010, was 78 years. Initial gain made through advent of sanitation, childhood immunizations. Since 1960, medical advances allowed lives to be prolonged. Procedures/surgeries, antibiotics, chemotherapy, heart/HTN medications, etc. People live longer, die differently

3
Death causes 1900

4
31% were relatively quick contagious dz, 14% lifestyle dz
Infectious diarrhea pneumonia 31% were relatively quick contagious dz, 14% lifestyle dz

5
Death causes 2004

6
56% are lingering deaths

7
2004 No contagious disease causes in the top 3 causes
56% of top 3 causes mostly lifestyle diseases 2004

8
Is cancer a “lifestyle” disease?
Sometimes cancer just happens Often lifestyle encourages development Lung, bladder, kidney, stomach, esophageal, oral, lymphoma---smoking Breast ---overweight, lack of exercise, high fat diet, ETOH, HRT Pancreas, stomach ---alcohol Colon---low fiber, high fat diet Is cancer a “lifestyle” disease?

9
Enter….the machines Advances in technology: Ventilators
Gastrostomy tubes Dialysis Implantable Cardiac Defibrillators Ventricular Assist Devices Enter….the machines

10
“The Dwindles“

11
The Dwindles --- a cascade of events
Desk-exercise not a priority Spent life watching football instead of playing football Smoke, poor diet, become overweight or obese Knees develop arthritis, ruptured back disk from wt Now can’t exercise if want to Become DM, HTN, COPD Stroke –paralyzed on one side. Can barely walk. Need spouse’s help Too big to care for. Strain on family Stratolounger or bed becomes your world Don’t forget the oxygen Smoking, DM, HTN, isolation---Alzheimer’s Inactive---Pneumonia –hosp—ventilator DM --Kidneys –dialysis Stroke ---MCS---feeding tube Three junctures enact AD.

12
DO WE HAVE THE “RIGHT TO DIE?”
Everyone born has a “right to life,” then what about a “right to die?” Should any law upholding a person’s right to life should inherently include their right to die? DO WE HAVE THE “RIGHT TO DIE?”

13
Court Cases-it’s what started it all.

14
Karen Ann Quinlan -1975

15
Stopping ventilators When 21, overdose of ETOH and 2 Rx drugs
Stopped breathing >15 min Persistent vegetative state, on ventilator Parents wanted removal , hospital fought Protracted court proceedings, tube removed Lived for almost another decade Stopping ventilators

16
Two significant outcomes of her case
development of formal ethics committees in hospitals, nursing homes and hospices and the development of advance health directives

17
Nancy Cruzen-1990

18
After an automobile accident left her in a persistent vegetative state, her family petitioned in courts for three years, as far as the U.S. Supreme Court (Cruzan v. Director, Missouri Department of Health), to have her feeding tube removed. The Court initially denied the family's request, citing lack of evidence of Cruzan's wishes. Went to the U.S. Supreme Court “Right to die”

19
Stopping feeding tubes
The family's request was ultimately granted by providing additional evidence. On December 15, 1990, the tube was removed and she died 12 days later. The courts recognized for the first time a constitutional right to refuse treatment in extraordinary circumstances. Stopping feeding tubes

20
The Birth of the Right to Die
The Cruzan decision spurred considerable interest in "living wills" which clearly express an individuals desire to discontinue treatment or feeding in specified circumstances. The Birth of the Right to Die

21
Terry Schiavo-2005

22
Terri Schiavo collapsed in her home in full cardiac arrest on February 25, She suffered massive brain damage due to lack of oxygen and eventually diagnosed as being in a persistent vegetative state.

23
Normal CT scan---Terri’s CT scan

24
Legal Battles Extraordinaire
Legal battle between her husband and the parents of Terri Schiavo that lasted from 1998 to Lack of a living will caused a protracted series of appeals to determine what Terri’s wishes would have been re. life-prolonging procedures. Legal Battles Extraordinaire

25
Keeping Terri alive became a focal point for the Right to Life movement
MULTIPLE appeals, motions, hearings, etc. Florida legislature Florida governor Bush Florida and U.S. Supreme Court Congressional Republicans President Bush Send in the ____

26
At issue was whether the husband had the right to make decisions to
At issue was whether the husband had the right to make decisions to . The highly publicized and prolonged series of legal challenges presented by the parents and by state and federal legislative intervention effected in total a seven-year delay before life support finally was terminated. What a mess!

27
the court finally found that Terri had made reliable oral declarations that she would have wanted the feeding tube removed, allowing her husband’s decision to terminate life support prevail.

28
Patient self determination act of 1991
The Patient Self-Determination Act requires that healthcare institutions receiving Medicare or Medicaid reimbursement provide patients with written information about their legal rights to participate in medical decisions by completing an advance directive. An important goal of the Patient Self- Determination Act is to encourage patients to indicate their preferences for end-of-life care before the need arises, thus allowing healthcare providers to honor individual choices, improve the quality of dying and reduce stress for families and caregivers Patient self determination act of 1991

29
Self-determination is derived from the principle that an adult has the right to decide what happens to his or her body. An advance directive documents the wish of a person to give directions about future medical care or to designate another person to make medical decisions if he or she loses decision-making capacity. The law also mandates that healthcare providers document the presence or absence of an advance directive in the patient’s medical record. A patient’s right to make decisions in an advance directive is protected by federal and state law. What the Law Intends

30
Who has Advanced Directives?
Only 14% of Americans have a written advance directive expressing their personal wishes for end-of-life care. This low percentage has significant implications for the aging U.S. population, as well as for younger adults who often don’t think about the need for an advance directive until they are confronted with a life-threatening terminal medical diagnosis. Living wills and other advance directives aren't just for older adults. Unexpected end-of-life situations can happen at any age, so it's important for all adults to have advance directives.

31
Who needs AD? Answer: everyone over age >=18.
Younger adults do not consider the need for AD, not considering death imminent. This age group known for risky behavior. Yet, main causes of death can lead to brain damage/death and an inability to make AD decisions. Leading causes of death for ages 15-25: Accidents, “unintentional injury”, MVA Homicide suicide Who needs AD?

32
People over age 65 whose heart stops outside the hospital setting have about a 2 percent chance of survival. Of those who survive, half will end up permanently in a nursing home. Only 1 percent will return home . Fully 50 percent of Medicare funds are exhausted caring for patients in the last 6 months of life. The sickest 1 percent utilize 30 percent of allocated Medicare funds while the top 10 percent consume 80 percent of those funds. While most Americans wish to die at home, 75% will die in a hospital or nursing home. The NUMBERS

33
Healthy, robust 86 year old. Walked 6 miles a day, played tennis 3x/wk
Hit by a car while jay walking. Initial injuries-femur (thigh) and ribs fracture, closed head injury, punctured lung. On ventilator. Had a stroke, went into kidney and liver failure. Developed pneumonia and placed on antibiotics. Had a reaction to antibiotics, turned bright red, and skin began to slough. Doctors considered dialysis. NO MPOA. Family could not agree to appropriate interventions. 3 months; much agony, and $1,000,000 later, he finally died. My friend’s father
 and ribs fracture, closed head injury, punctured lung. On ventilator. Had a stroke, went into kidney and liver failure. Developed pneumonia and placed on antibiotics. Had a reaction to antibiotics, turned bright red, and skin began to slough. Doctors considered dialysis. NO MPOA. Family could not agree to appropriate interventions. 3 months; much agony, and $1,000,000 later, he finally died. My friend’s father.")
34
ACUTE- sudden events that require immediate care decisions
Massive stroke Heart attack with/without arrest, heart failure MVA COPD exacerbation/pneumonia Sepsis (massive infection) Traumatic brain injury Defining events I
 Traumatic brain injury. Defining events I.")
35
CHRONIC---no sudden event, no clear line of delineation as when to stop interventions
Dementia/Alzheimer’s Disease “global geriatric decline/debility”—weight loss, falls, frailty, loss of ability to performs Activities of Daily Living (ADLs) “the dwindles” Cancer, neurologic diseases, autoimmune diseases Chronic CHF, COPD, CAD Defining events II
 the dwindles Cancer, neurologic diseases, autoimmune diseases. Chronic CHF, COPD, CAD. Defining events II.")
36
Vegetative states: let’s add to the confusion
A vegetative state is a rare condition, caused by brain damage, in which a person comes out of a coma and is fully awake but they have no sense of awareness. 14,000 people per year Vegetative states: let’s add to the confusion

37
a traumatic brain injury – caused by a severe head injury such as that sustained during a car accident or a fall from a great distance non-traumatic brain injury – where the injury to the brain is caused by a health condition such as a stroke or Alzheimer's disease Causes

38
Vegetative v.s. MCS 40 % diagnosed with Minimally Conscious State.
there is a condition called "locked-in syndrome" where a person is fully aware but is unable to move any of their muscles, so they are unable to move or speak. Aphasia, spasticity, blind, deaf, epileptic, paralyzed, amnesic Unlike persistent vegetative state, patients with MCS have partial preservation of conscious awareness. Squeeze hands, follow objects on command. Consciousness often fluctuates. Rare, but occasionally awaken (to some degree). Vegetative v.s. MCS
. Vegetative v.s. MCS.")
39
In a young person under the age of 20 who experiences traumatic brain damage, the chances of making a recovery are around 1 in 5. A person over the age of 40, who is an persistent vegetative state due to a non- traumatic brain damage, has an extremely small chance of making a recovery. People who do make a recovery are often likely to have life-long physical and mental disabilities resulting from the damage to their brain. “Recovery?”

40
If you were in a MCS, what would you want?
Both conditions require a feeding tube. If you were in a MCS, what would you want?

41
What treatments would you want?
How important to you is being independent and self-sufficient? What would make your life not worth living? Would you want treatment to extend life in any situation? Would you want treatment only if a cure is possible? Do you have a goal in mind that influences your decision about extending your life? (wedding, graduation). Would you want palliative care or hospice to ease pain and discomfort if you were terminally ill? What treatments would you want?
. Would you want palliative care or hospice to ease pain and discomfort if you were terminally ill What treatments would you want")
42
Interventions I Resuscitation Ventilators
Resuscitation. Restarts the heart when it has stopped beating (cardiac death). Determine if and when you would want to be resuscitated by cardiopulmonary resuscitation (CPR) or by a device that delivers an electric shock to stimulate the heart. Can lead to cardiac assist devices (balloon pump) and medications to maintain BP, kidney function. Mechanical ventilation. Takes over your breathing if you're unable to do so. Consider if, when and for how long you would want to be placed on a mechanical ventilator. Interventions I
. Determine if and when you would want to be resuscitated by cardiopulmonary resuscitation (CPR) or by a device that delivers an electric shock to stimulate the heart. Can lead to cardiac assist devices (balloon pump) and medications to maintain BP, kidney function. Mechanical ventilation. Takes over your breathing if you re unable to do so. Consider if, when and for how long you would want to be placed on a mechanical ventilator. Interventions I.")
43
Interventions II Nutrition/hydration Dialysis
Nutritional and hydration assistance. Supplies the body with nutrients and fluids intravenously or via a tube in the stomach. Decide if, when and for how long you would want to be fed in this manner. IV fluids-basic hydration “TPN”-IV protein, carbs, fats, fluids Gastrostomy tube- surgically placed tube for feeding directly into stomach. Dialysis. Removes waste from your blood and manages fluid levels if your kidneys no longer function. Determine if, when and for how long you would want to receive this treatment. Treatments 3x/wk for 4- 6 hrs Interventions II

44
Interventions III Pericardial tap Paracentisis Thorocentesis Surgery
? comfort versus treatment Interventions III

45
Emergency care---do you wish to be hospitalized for further interventions?
Antibiotics -– do you wish to be treated for a pneumonia or sepsis (blood poisoning)? Do you just wish to remain comfortable and in your own home in your last days? Is hospice or home-based Palliative Care a better choice ? Interventions IV
 Do you just wish to remain comfortable and in your own home in your last days Is hospice or home-based Palliative Care a better choice Interventions IV.")
46
Your most important asset is a trusted MD who can provide you with realistic choices/outcom e/expectations MD role

47
Example: COPD Can be treated, but not cured Will get worse over time
Get pneumonia a lot Repeat hospitalizations Wearing oxygen Debilitating, reducing quality of life What’s it like to be intubated, air hungry? Example: COPD

48
What are your goals? What are your thoughts about dying?
Do you want to avoid pain at all costs or do you want to be awake/alert? What kind of quality of life is acceptable? What are your goals? Wedding/graduation? What are your goals?

49
First, what exactly DO you want?
Let’s start with choosing an MPOA. First, what exactly DO you want?

50
Medical power of attorney (MPOA) aka “Healthcare Proxy”
Medical or health care power of attorney (MPOA). The medical POA is a legal document that designates an individual — referred to as your health care agent or proxy — to make medical decisions for you in the event that you're unable to do so. It is different from a power of attorney authorizing someone to make financial transactions for you. Medical power of attorney (MPOA) aka “Healthcare Proxy”
. The medical POA is a legal document that designates an individual — referred to as your health care agent or proxy — to make medical decisions for you in the event that you re unable to do so. It is different from a power of attorney authorizing someone to make financial transactions for you. Medical power of attorney (MPOA) aka Healthcare Proxy")
51
MPOA—your most important decision
Trust is the most important element in choosing an MPOA . Feel free to say what you want and how you feel about End of Life issues. Prefer a committed, able MPOA who knows what it is to be an agent. It’s not about what the MPOA wants. MPOA—your most important decision

52
Don’t chose someone out of a feeling of guilt or obligation.
Choosing a person to act as your health care agent is possibly the most important part of your planning. You need to trust that this person has your interests at heart, understands your wishes and will act accordingly. He or she should also be mature and levelheaded, and comfortable with candid conversations. Good communication is essential! Don’t chose someone out of a feeling of guilt or obligation. Choosing an MPOA

53
Your health care agent doesn't necessarily have to be a family member
Your health care agent doesn't necessarily have to be a family member. You may want your health care decision maker to be different from the person you choose to handle your financial matters. It may be helpful, but it's not necessary, if the person lives in the same city or state as you do. Share your wishes with your family. Choosing an MPOA

54
Who is an incapacitated adult?
An adult “who is unable to effectively receive or evaluate information or both or make or communicate decisions to such an extent that the individual lacks the ability to satisfy essential requirements for physical health, safety, or self-care, even with appropriate and reasonably available technological assistance. Who is an incapacitated adult?

55
Group of “interested parties” get together and choose one of the group to be a Proxy Decision Maker.
Medical Healthcare Proxy form : Uh-Oh! No MPOA!

56
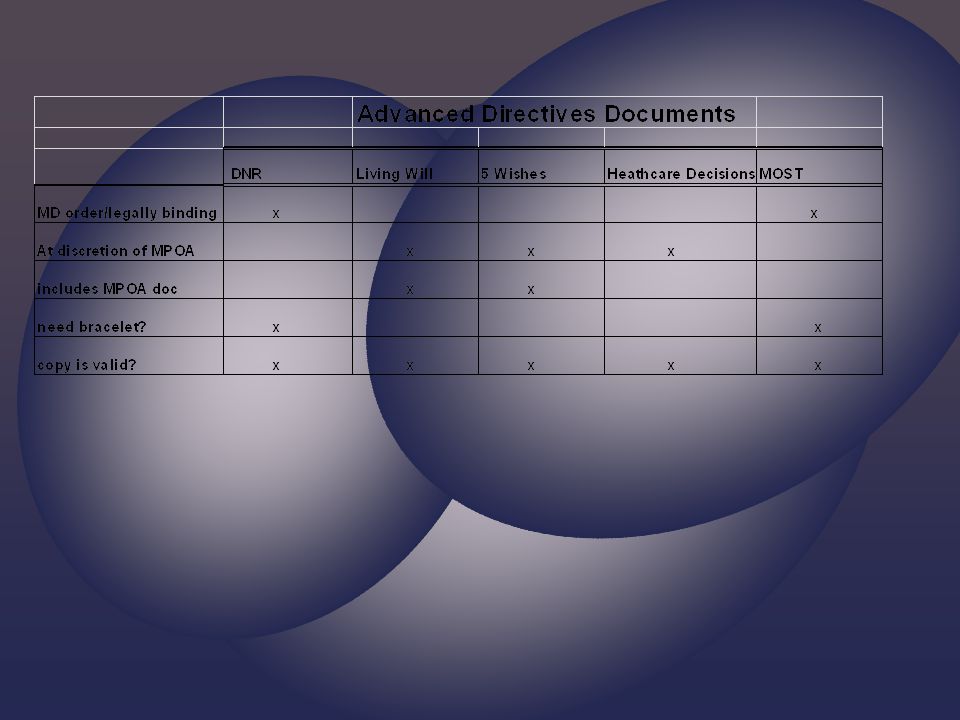
Do not resuscitate (DNR) order
Do not resuscitate (DNR) order. This is a request to not have cardiopulmonary resuscitation (CPR) if your heart stops or if you stop breathing. Advance directives do not have to include a DNR order, and you don't have to have an advance directive to have a DNR order. Your doctor can put a DNR order in your medical chart It is a legal, binding physician order. Does not expire. DNR
 order. This is a request to not have cardiopulmonary resuscitation (CPR) if your heart stops or if you stop breathing. Advance directives do not have to include a DNR order, and you don t have to have an advance directive to have a DNR order. Your doctor can put a DNR order in your medical chart. It is a legal, binding physician order. Does not expire. DNR.")
57
Notifying your DNR status
File of Life or envelope on your fridge ID bracelet or necklace Documentation on your person? Tattoo? Notifying your DNR status

58
In hospital setting-is honored as documentation readily available and can ID pt.
Validity of DNR and identity of person need to be confirmed ~any ?~CPR The reality of DNR

59
Advantages: At home –paramedics often follow if documentation readily available Deficits: Specific only to resuscitation efforts In the field---rarely gets followed. DNR

60
Living will. This written, legal document spells out the types of medical treatments and life- sustaining measures you want and don't want, such as mechanical breathing (respiration and ventilation), tube feeding or resuscitation in the event you are incapacitated. Not a physician order, rather a directive. A living will needs an MPOA to enact your wishes Living Wills

61
Living Wills Advantages: Short and sweet
Gives specific time parameters Can be strictly interpreted but is mostly a guide for MPOA Deficits: Not very detailed No DNR Almost never happens—MPOA steps in Living Wills

62
Wish 1: The Person I Want to Make Care Decisions for Me When I Can't
This section is an assignment of a health care agent (also called proxy, surrogate, representative or health care power of attorney). This person makes medical decisions on your behalf if you are unable to speak for yourself. Wish 2: The Kind of Medical Treatment I Want or Don't Want This section is a living will—a definition of what life support treatment means to you, and when you would and would not want it. Wish 3: How Comfortable I Want to Be This section addresses matters of comfort care— what type of pain management you would like, personal grooming and bathing instructions, and whether you would like to know about options for hospice care, among others.. 5 wishes
. This person makes medical decisions on your behalf if you are unable to speak for yourself. Wish 2: The Kind of Medical Treatment I Want or Don t Want. This section is a living will—a definition of what life support treatment means to you, and when you would and would not want it. Wish 3: How Comfortable I Want to Be. This section addresses matters of comfort care— what type of pain management you would like, personal grooming and bathing instructions, and whether you would like to know about options for hospice care, among others.. 5 wishes.")
63
5 Wishes Wish 4: How I Want People to Treat Me
This section speaks to personal matters, such as whether you would like to be at home, whether you would like someone to pray at your bedside, among others. Wish 5: What I Want My Loved Ones to Know This section deals with matters of forgiveness, how you wish to be remembered and final wishes regarding funeral or memorial plans. 5 Wishes

64
5 Wishes Advantages: Comprehensive Contains place for MPOA designation
Deficits A bit long As with Living Will—guide for MPOA $ agingwithdignity.org 5 Wishes

65
My Healthcare Decisions
What do you want to know about your condition ? Strict adherence or interpretation? Where to die? Quality of life? Treatment options Spirituality Organ donation Body treatment after death My Healthcare Decisions

66
My Healthcare Decisions
Advantages: Can personalize and add narrative Comprehensive Asks smart questions Deficits Still need to assign an MPOA separately Does not contain a DNR My Healthcare Decisions

67
MOST FORM Does not need an MPOA consult and to enact.
It is a legal, binding physician order. Covers resuscitation status Medical interventions such as full, limited, and comfort measures Antibiotics IV therapy Tube feeding MOST FORM

68
The MOST form Basically 4 parts DNR
Level of medical interventions –level of airway management Antibiotics Artificial nutrition The MOST form

69
MOST Advantages: MD order Comfort measures never optional
More comprehensive than DNR Deficits: Not flexible MOST

70
All Advanced directives documents can be changed or rescinded at any time.
Change your mind?

72
Multiple choice questions
Do you need a A. DNR B. Living Will C. 5 wishes D. MPOA E. MOST F. All of the above ? Multiple choice questions

73
What do you need? Most important—MPOA you trust!
Do you want something definitive – DNR/MOST? (no MPOA needed) Do you want resuscitation then decision by your MPOA? Most EOL decisions will be made by your MPOA What do you need?
 Do you want resuscitation then decision by your MPOA Most EOL decisions will be made. by your MPOA. What do you need")
74
Issues that might come up
Your MPOA chooses not to follow your wishes Disagreements within family and between the MPOA (MPOA has final decision) The 23 year old who sees his grandfather die on a ventilator and acts impulsively in completing a DNR or MOST Issues that might come up
 The 23 year old who sees his grandfather die on a ventilator and acts impulsively in completing a DNR or MOST. Issues that might come up.")
75
Talking with your doctor
Healthcare Affordability Act now allows for one free visit with your primary care physician to discuss AD. Once you've filled out the forms, give copies to your doctor, the person you've chosen as your health care agent and your family members. Keep another copy in a safe but accessible place. You might also want to keep a card in your wallet that says you have a living will and where it can be found. Talking with your doctor

76
Barriers to Completing Advance Directives
Patient and provider reluctance Time constraints Assumptions about treatment preferences Denial and procrastination Unrealistic expectations Delaying until a crisis Discomfort with palliative care planning Lack of documentation of medical orders Cultural and health system barriers Lack of knowledge about the Patient Self-Determination Act and advance directives among community members Source: Butterworth AM. Reality check: 10 barriers to advance planning. Nurs Pract. 2003;28(5):42-43 Barriers
: Barriers.")
77
1.Even when patients have advance directives, they are often vague, incomplete, disregarded by family members or unacknowledged by caregivers. 2.When family members can’t agree on what should be done. 3. Hospitals and physicians often pursue the most aggressive treatment plan possible, even when the patient is close to death. 4. Deciding to curtail treatment in critical care settings poses unique problems. 5. Many patients and their families have had little or no experience with critical care before they face end-of-life care choices. 6. It may be difficult to convince some families that the aim of withholding or withdrawing treatment is to alleviate suffering. “Intervention at all costs.” Other obstacles

78
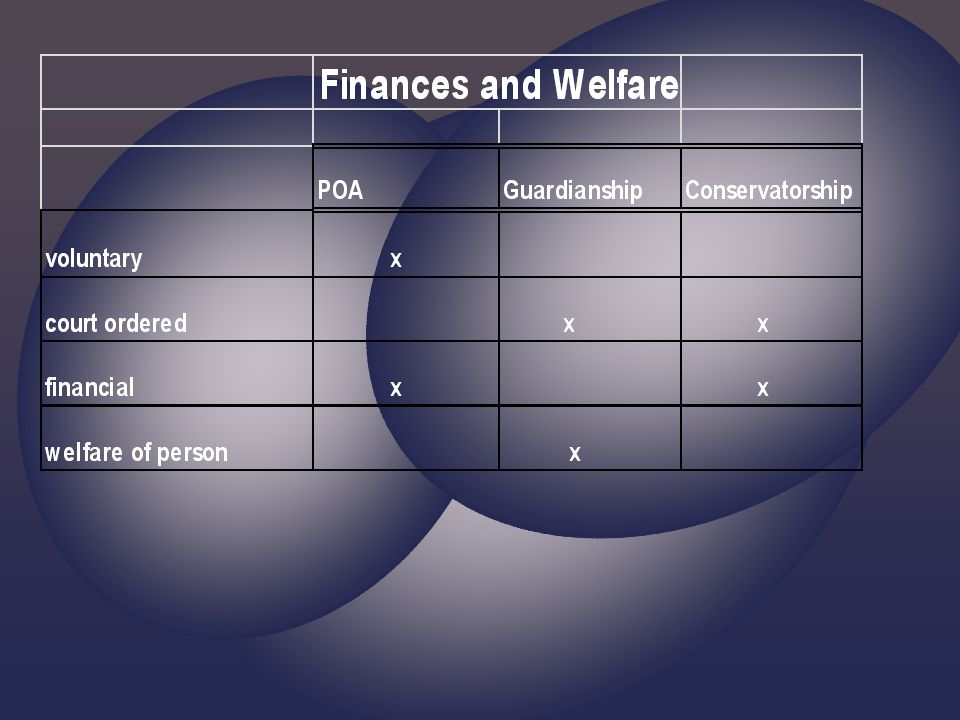
Durable Power of Attorney (DPOA)
Through this type of advance directive, an individual executes legal documents that provide the power of attorney to others in the case of an incapacitating medical condition. The durable power of attorney allows an individual to make bank transactions, sign social security checks, apply for disability, or simply write checks to pay the utility bill while an individual is medically incapacitated. Durable Power of Attorney (DPOA)
")
79
A word about Guardianship
A guardian is a person or persons appointed by a court to assist with the personal affairs and make decisions on behalf of a minor or an adult who is incapacitated. A person under a guardianship is called a ward. Court ordered A word about Guardianship

80
My patient, Delores

81
No Advanced Directives for medical/financial
Small house in Longmont Filthy—never cleaned, fridge science experiment Dogs --vet Significant dementia Drove –Kansas, Wyoming, Boulder Gero-psych unit Placement Guardianship by son

82
A word about Conservatorship
A conservator is a person, or persons, appointed by a court to manage finances and property for an adult who is incapacitated, and whose assets may be wasted or dissipated unless management is provided. (Usually there is dementia or emotional instability). Charities Scams Unscrupulous family members Poor buying choices A word about Conservatorship
. Charities. Scams. Unscrupulous family members. Poor buying choices. A word about Conservatorship.")
83
More about conservatorship
Different than MPOA as this is after the fact and is court-ordered. More about conservatorship

85
You can also specify in your advance directives any wishes you have about donating your organs, eyes and tissues for transplantation-sign up online in the Colorado Organ and Tissue Donor Registry at Indicate your wishes on your driver’s license or state ID when you apply for or renew it. Let your MPOA and family know your wishes. Desire to donate needs to be documented prior to death. Organ donation

87
. If you wish to donate your body for scientific study:
Colorado State Anatomical Board P.O. Box 6511, MS 8501 Aurora, CO 80045 Phone: URL: eges/medicalschool/departments/CellDevelop mentalBiology/anatomicalboard/Aboutus/Page s/default.aspx WHOLE BODY DONATION

88
Website Resources Website Resources
“Put It in Writing” — uses a Q and A format to help patients learn about types of advance directives and their importance. Partnership for Caring — provides information about end-of-life options and how to document them. Aging with Dignity — publishes Five Wishes, a tool that helps patients consider their medical, personal, emotional and spiritual needs in planning end-of-life choices. ml MOST form –State of Colorado- OST_Form_ pdf Website Resources

89
Growing old is not for sissies.

90
What is it to live a full and meaningful life?

92
The 5 Secrets What must we discover before we die?
What do those at the end of their lives have to teach us? Why do some people find meaning and die happy? What does it mean to live a full and meaningful life? The 5 Secrets

93
This is what they said……
Izzo asked 15,000 people to sent in names of wise elders 1,000 responses received Interviewed 235 ‘wise elders’ ages This is what they said……

94
Be true to yourself –am I following my heart
Be true to yourself –am I following my heart? Am I focused on things that really matter? Am I being the person I want to be? Leave no regrets –constantly asking—“ When I get old and ready to die will I regret the step I am about to make?’ Become love—love yourself, treat others w kindness The Wisdom

95
Live in the moment—every day, every moment is a gift
Live in the moment—every day, every moment is a gift. Chose to be in the moment. Give more than you take---make the world a better place. Leave a legacy.

97
More questions, comments, or for a great green chili recipe:

Similar presentations