Download presentation
Presentation is loading. Please wait.

1
Blood Bank Case Studies
Case Studies from the reference laboratory Jackie Ensley, MLS(ASCP)CMSBB
CMSBB.")
2
Objectives Present various case studies and describe the approach to serologic problem solving and antibody identification. Determine possible causes of pan-reactivity and steps to resolve complex antibody cases. Briefly review serologic and molecular characteristics of antibodies identified and their respective blood group system, including clinical significance. Explain the various techniques and methods used in the case studies for antibody identification.

3
Antibody Identification
Antibody detection and identification is a complex problem-solving process Many techs may have a “gut-feeling” about the antibody before testing completion and intuitively know what needs to be done for antibody identification Be prepared to reevaluate your hypothesis if testing results do not fit with initial assessment

4
Antibody Identification
Use the tools available to help you detect and then identify the antibody: Gel/solid phase Tube testing: saline/PeG/LISS/albumin/Room temperature/4˚C Enzymes such as ficin, papain, trypsin Chemicals such as 0.2M DTT Adsorption/elution Reticulocyte/sickle cell separation Phenotypically similar cells Antisera/rare antigen negative cells

5
Antibody Identification
Know phases of reactivity Some antibodies react best at room temperature/4˚C (M, N, P1, Lewis, etc) Some antigens destroyed by enzymes/chemicals (Ficin destroys Fya, Fyb, M, N, etc) Enzyme treatment of red cells enhances reactivity of some antibodies such as those in the Rh system, Jka, Jkb, Lea, Leb, P1 Know strength/pattern of reactivity Some antigens show variable antigen expression and some antibodies show variable reactivity and may show dosage, such as -Jka/-Jkb and -M/-N Note: different strengths may also indicate more than one antibody is present
 Some antigens destroyed by enzymes/chemicals (Ficin destroys Fya, Fyb, M, N, etc) Enzyme treatment of red cells enhances reactivity of some antibodies such as those in the Rh system, Jka, Jkb, Lea, Leb, P1. Know strength/pattern of reactivity. Some antigens show variable antigen expression and some antibodies show variable reactivity and may show dosage, such as -Jka/-Jkb and -M/-N. Note: different strengths may also indicate more than one antibody is present.")
6
Antibody Identification
Besides using the blood bank techniques available to detect the antibody, also keep in mind these tips to aid you in the identification process: Review patient’s records, including medication, age, gender, race, diagnosis and transfusion history Investigate/repeat any inconsistent or contradictory reactions in the patient’s workup Phenotype the patient to confirm they are antigen negative for the suspected or identified antibodies

7
Case Study 1 Female, 51 years old Caucasian
PATIENT HISTORY Female, 51 years old Caucasian Diagnosis: Anemia and GI bleed The patient was seen on 12/12/ She typed as A Positive and had a negative antibody screen. She was transfused at that time. Current H/H: 7.7/ 24.8 The hospital reports on 2/14/2014 a positive antibody screen in tubes with LISS (3+) with a positive autocontrol. The DAT/IgG is positive (2+). 4 out of 4 units are crossmatch incompatible. Hospital decides to send to the reference laboratory.
 with a positive autocontrol. The DAT/IgG is positive (2+). 4 out of 4 units are crossmatch incompatible. Hospital decides to send to the reference laboratory.")
8
Case Study 1 Reference Lab testing: ABO/Rh performed: DAT Performed:
Anti-A Anti-B Anti-D A1 Cell B Cell ABO/Rh 4+ A Positive Anti-IgG/ Gel Anti-C3/ Gel 3+

9
Plasma + 2+ 1+ D C c E e K k AHG-PeG Cell I II III Auto Room Temp Kpa
Rh System Kell Duffy Kidd Lewis P MNS Lutheran Room Temp AHG-PeG Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub I + 2+ II 1+ III Auto

10
Plasma + 2+ w D C c E e K k M N S s Rh System Kell Duffy Kidd Lewis P
Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub 1 + 2+ 2 3 4 5 6 7 8 9 10 11 w Auto

11
Eluate + 3+ w The Eluate Last Wash is negative D C c E e K k M N S s
Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub 1 + 3+ 2 3 4 5 6 7 8 9 10 11 w The Eluate Last Wash is negative

12
Let’s look at what we know:
Serologic Problem Solving Question to ask yourself: So where do we go at this point? Let’s look at what we know: Phase of reactivity: AHG Strength/pattern of reactivity: pan-reactive, about the same strength. Patient history: recently transfused DAT/autocontrol: positive/reactive Other info: eluate is also pan-reactive with same strength

13
Narrowed down possibilities: Warm autoantibody
Serologic Problem Solving Question to ask yourself: So where do we go at this point? Narrowed down possibilities: Warm autoantibody Multiple antibodies in plasma (and eluate) Antibody to a high incidence antigen
 Antibody to a high incidence antigen.")
14
Why not an adsorption on the eluate?
Next Step: Reference tech decides to perform adsorption on plasma only. Why not an adsorption on the eluate? The patient has been transfused in the last 3 months… Technical Manual States that “newly developed antibodies initially detectable only in the eluate are usually detectable in the serum after about 14 to 21 days”

15
Blood Bank Technique: Adsorption
What is an adsorption? Blood bank technique where red cells and plasma (or eluate) are mixed, causing antibody to be adsorbed onto the red cell surface. Types of Adsorption: Autologous: Patient plasma is mixed with patient cells PATIENT MUST NOT HAVE BEEN TRANSFUSED last 3 months Differential/Allogeneic: Patient plasma is mixed with R1R1, R2R2, and rr donor cells of known phenotypes. Antibodies to high incidence antigens may be adsorbed out
 are mixed, causing antibody to be adsorbed onto the red cell surface. Types of Adsorption: Autologous: Patient plasma is mixed with patient cells. PATIENT MUST NOT HAVE BEEN TRANSFUSED last 3 months. Differential/Allogeneic: Patient plasma is mixed with R1R1, R2R2, and rr donor cells of known phenotypes. Antibodies to high incidence antigens may be adsorbed out.")
16
How is an alloadsorption performed?
Blood Bank Technique: Adsorption Alloadsorption: Patient has been transfused or transfusion is unknown. R1R1 = R2R2 rr Incubate together to adsorb the antibodies onto the donor red cells Patient’s Plasma + Donor RBC’s

17
How is an alloadsorption performed?
R1R1 Adsorption Cells- discard Adsorption Plasma- Test R2R2 = rr Incubation allows any antibody to adsorb onto the red cells (alloantibody or autoantibody) Centrifuge the tubes and separate the adsorbed plasma from the red cells for testing
 Centrifuge the tubes and separate the adsorbed plasma from the red cells for testing.")
18
How is an alloadsorption performed?
R1R1 (D+C+E-c-e+) R2R2 (D+C-E+c+e-) rr (D-C-E-c+e+) Example: anti-E Example: anti-E Run each adsorbed plasma with panel cells to identify any antibodies. Antibodies in adsorbed plasma will depend on the phenotype of the adsorbing cell.
 R2R2. (D+C-E+c+e-) rr. (D-C-E-c+e+) Example: anti-E. Example: anti-E. Run each adsorbed plasma with panel cells to identify any antibodies. Antibodies in adsorbed plasma will depend on the phenotype of the adsorbing cell.")
19
R1R1 Adsorption w + 0√ 1+ 2+ D C c E e K k M N S s Rh System Kell
Rh System Kell Duffy Kidd Lewis P MNS Lutheran X2 PeG- Plasma Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub R1R1 Cell Phenotype + 1 0√ 2 1+ 3 4 2+ 5 6 7 8 9 10 11 w

20
R2R2 Adsorption w + 0√ D C c E e K k M N S s Rh System Kell Duffy Kidd
Rh System Kell Duffy Kidd Lewis P MNS Lutheran X3 GEL-Plasma Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub R2R2 Cell Phenotype + 1 0√ 2 3 4 5 6 7 8 9 10 11 w

21
rr Adsorption w + 0√ D C c E e K k M N S s Rh System Kell Duffy Kidd
Rh System Kell Duffy Kidd Lewis P MNS Lutheran X3 GEL-Plasma Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub r r Cell Phenotype + 1 0√ 2 3 4 5 6 7 8 9 10 11 w

22
R1R1 Adsorption w + 0√ 1+ 2+ D C c E e K k M N S s Rh System Kell
Rh System Kell Duffy Kidd Lewis P MNS Lutheran X2 PeG- Plasma Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub R1R1 Cell Phenotype + 1 0√ 2 1+ 3 4 2+ 5 6 7 8 9 10 11 w

23
Autoantibody Confirmation Testing
Patient had been transfused in the last 3 months so need to perform reticulocyte separation Want to be testing patient cells and not donor cells

24
How is a Reticulocyte Cell Separation Performed?
Blood Bank Technique: Reticulocyte Cell Separation How is a Reticulocyte Cell Separation Performed? Patient has been transfused so need to separate patient cells from donor red cells Stopper one end of the hematocrit tube with clay. Spin the sample down and fill microhematocrit tubes with the red cells.

25
How is a Reticulocyte Cell Separation Performed?
Blood Bank Technique: Reticulocyte Cell Separation How is a Reticulocyte Cell Separation Performed? Air Excess saline/plasma Buffy Coat Newer Red Cells Older Red Cells Spin the microhematocrit tubes and then cut the tubes to get the reticulocytes Clay Plug

26
Autoantibody Confirmation Testing
Now that we have the retics: DAT/IgG had been positive so perform DAT/IgG on retics: Retics Anti-IgG/ tube 1+ Can not proceed with testing to identify warm autoantibody until the DAT is negative

27
How do we get the DAT/IgG negative?

28
Blood Bank Technique: EGA Treatment
What is EGA? EDTA glycine acid dissociates IgG from red blood cells so the treated red cells can be used for further testing or antigen typing using the AHG phase. Use when direct antiglobulin phase (DAT) is positive Does not impair red cell surface antigens
 is positive. Does not impair red cell surface antigens.")
29
Blood Bank Technique: EGA Treatment
The Process Wash IgG coated red cells thoroughly Suspend cells briefly in EGA solution to dissociate bound IgG antibody Bring mixture to neutral pH Centrifuge and wash cells with saline Test treated cells by performing a DAT Limitation: destroys Kell, Era, Bg antigens

30
Autoantibody investigation
EGA testing performed and DAT negative retics obtained To confirm the antibody is warm autoantibody the DAT negative retics are tested against the plasma and eluate: Retics-Plasma Retics-Eluate Gel 2+ 3+ This is what was expected if the antibody was autoantibody! Further testing is not required, the warm autoantibody has been confirmed.

31
Antibody Confirmation
Lastly need to confirm anti-Jka (JK1) by antigen typing Use retics so that typing patient cells and not donor cells Anti-Jk Tube Patient types Jka negative
 by antigen typing. Use retics so that typing patient cells and not donor cells. Anti-Jk. Tube. Patient types Jka negative.")
32
Results Patient has warm autoantibody and anti-Jka (JK1).
Transfusion recommendations: Transfuse Jka- (JK1), AHG crossmatch least incompatible, red blood cell products.
, AHG crossmatch least incompatible, red blood cell products.")
33
Kidd Blood Group System
Located Chromosome 18 Glycoprotein with 10 membrane spanning domains ·Daniels, G. (2013) Kidd Blood Group System, in Human Blood Groups, 3rd edition, Wiley-Blackwell, Oxford, UK. Kidd antibodies are often difficult to work with and are a common cause of delayed hemolytic reactions
 Kidd Blood Group System, in Human Blood Groups, 3rd edition, Wiley-Blackwell, Oxford, UK. Kidd antibodies are often difficult to work with and are a common cause of delayed hemolytic reactions.")
34
Jka (JK1) Antibody & Antigen
Jka Antibody Characteristics History 1951 Clinical Significance Yes! Clinically significant ·Transfusion Reactions possible, immediate or delayed hemolytic ·HDN possible, mild to moderate Antibody IgG/IgM Other facts ·Jka has been demonstrated on fetal cells as early as 11 weeks ·Antibody fades in vitro and in vivo ·Can show dosage Jka Antigen Characteristics Occurrence Caucasians 77% Blacks 92% Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier.
. The Blood Group Antigen FactsBook, 3rd Edition, Elsevier.")
35
Case Study 2 Female, 38 years old African American DIAGNOSIS:
PATIENT HISTORY Female, 38 years old African American DIAGNOSIS: -Severe Sepsis--blood cultures showed Finegoldia magna (normal flora of the gastrointestinal and genitourinary tract, and can be isolated from skin and the oral; often regarded as a contaminant in cultures) with subsequent cultures after that date with no growth. -Probable pneumonia -Cardiac arrest -Hypertensive -Acute respiratory failure -Acute renal failure -Positive for influenza A
 with subsequent cultures after that date with no growth. -Probable pneumonia. -Cardiac arrest. -Hypertensive. -Acute respiratory failure. -Acute renal failure. -Positive for influenza A.")
36
Case Study 2 PATIENT HISTORY The patient arrived as in-patient on 1/15/2014 and was typed as B Positive with negative antibody screen. Patient was transfused 2 B Positive RBCs at that time. Patient was monitored and was still very ill On 1/24/2014 patient required another transfusion and sample was sent to hospital blood bank.

37
Case Study 2 The 2nd sample was collected on 1/24/2014, 9 days after transfusion. Sample was sent to the reference laboratory Hospital Results on 1/24/2014: B Positive All cells reactive 2+ in gel Autocontrol positive

38
Case Study 2 Reference Lab testing: ABO/Rh performed: DAT Performed:
Anti-A Anti-B Anti-D A1 Cell B Cell ABO/Rh 4+ B Positive Anti-IgG/ Gel Anti-C3/ tube W+ 0√

39
Plasma + 1+ 2+ 0√ D C c E e K k AHG-PeG Cell I II III Auto Room Temp
Rh System Kell Duffy Kidd Lewis P MNS Lutheran Room Temp AHG-PeG Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub I + 1+ II 2+ III Auto 0√

40
Plasma + W 2+ W+ D C c E e K k M N S s Rh System Kell Duffy Kidd Lewis
Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub 1 + W 2+ 2 3 4 5 6 7 8 9 10 11 Auto W+

41
Eluate + W 4+ The Eluate Last Wash is negative D C c E e K k M N S s
Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub 1 + W 4+ 2 3 4 5 6 7 8 9 10 11 The Eluate Last Wash is negative

42
Question to ask yourself: So where do we go at this point?
Serologic Problem Solving Question to ask yourself: So where do we go at this point? Let’s look at what we know: Phase of reactivity: AHG Strength/pattern of reactivity: pan-reactive, same strength. Patient history: recently transfused DAT/autocontrol: positive/reactive Other info: eluate is also pan-reactive with same strength

43
Question to ask yourself: So where do we go at this point?
Serologic Problem Solving Question to ask yourself: So where do we go at this point? Narrowed down possibilities: Warm autoantibody Multiple antibodies in plasma and eluate Antibody to a high incidence antigen

44
Why perform an adsorption?
Next Step: Reference tech decides to perform adsorptions on plasma & eluate. Why perform an adsorption? To adsorb out suspected warm autoantibody and determine if there are any alloantibodies hiding under the pan-reactivity.

45
R1R1 Adsorption + W D C c E e K k M N S s Rh System Kell Duffy Kidd
Rh System Kell Duffy Kidd Lewis P MNS Lutheran X3 GEL- Plasma X3 GEL- Eluate Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub R1R1 Cell Phenotype + 1 W 2 3 4 5 6 7 8 9 10 11

46
R2R2 Adsorption + W D C c E e K k M N S s Rh System Kell Duffy Kidd
Rh System Kell Duffy Kidd Lewis P MNS Lutheran X3 GEL-Plasma X3 GEL-Eluate Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub R2R2 Cell Phenotype + 1 W 2 3 4 5 6 7 8 9 10 11

47
rr Adsorption + W D C c E e K k M N S s Rh System Kell Duffy Kidd
Rh System Kell Duffy Kidd Lewis P MNS Lutheran X3 GEL-Plasma X3 GEL-Eluate Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub r r Cell Phenotype + 1 W 2 3 4 5 6 7 8 9 10 11

48
Results Appears to be warm autoantibody
No alloantibodies were detected in the alloadsorbed plasma or eluate Need to confirm warm autoantibody

49
Autoantibody Confirmation Testing
Patient had been transfused 9 days ago so perform reticulocyte separation. DAT/IgG had been positive so perform DAT/IgG on retics: Retics Anti-IgG/ Gel O Proceed with further testing to identify warm autoantibody

50
Autoantibody Confirmation Testing
To confirm the antibody is warm autoantibody the retics are tested against the plasma and eluate: Retics-Plasma Retics-Eluate Gel This is NOT what was expected if the antibody was autoantibody! Further testing is required and now antibody to a high incidence antigen is suspected

51
Narrowed down possibilities: Warm autoantibody
Serologic Problem Solving Question to ask yourself: So where do we go at this point? Narrowed down possibilities: Warm autoantibody Multiple antibodies in plasma and eluate Antibody to a high incidence antigen

52
Some Techniques/Options Available:
Next Step: Use blood bank techniques, reagents and cells to try and determine the antibody Some Techniques/Options Available: Enzymes (ficin, papain, trypsin, etc) Chemicals such as DTT Phenotype Patient Rare antisera Rare cells
 Chemicals such as DTT. Phenotype Patient. Rare antisera. Rare cells.")
53
Ficin Panel + W 2+ 3+ W+ 1+ GEL-Ficin GEL D C c E e K k M N S s
Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL GEL-Ficin Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub 1 + W 2+ 3+ 2 3 4 5 6 7 8 9 10 11 Auto W+ 1+

54
0.2 M DTT Panel + W 2+ W+ D C c E e K k M N S s Rh System Kell Duffy
Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL GEL-0.2M DTT Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub 1 + W 2+ 2 3 4 5 6 7 8 9 10 11 Auto W+

55
Consider the race of patient and start with the easiest to test for
Case Study 2 Ficin and DTT testing has helped narrow down the possibilities. Some high incidence antigens resistant to Ficin and 0.2M DTT Treatment: Lan ABTI PEL U Fy3 Ata MAM Dib Ge3 Fy5 Emm Oka Wrb EnaFR Era Sda (Ficin enhanced0 Coa CO3 Vel (Ficin enhanced) Jra (Ficin enhanced) The list is not all-inclusive. Refer to The Blood Group Antigen FactsBook by Marion E Reid and Christine Lomas-Francis for support regarding antigen/antibody reactivity. Consider the race of patient and start with the easiest to test for
 Jra (Ficin enhanced) The list is not all-inclusive. Refer to The Blood Group Antigen FactsBook by Marion E Reid and Christine Lomas-Francis for support regarding antigen/antibody reactivity. Consider the race of patient and start with the easiest to test for.")
56
Patient is antigen typed with the retics and is U-
Selected Cells Run Plasma Testing Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL Donor D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub U D1083 + N1727 Eluate Testing Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL Donor D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub U D1083 + N1727 Patient is antigen typed with the retics and is U-

57
BioArray Molecular Results
Rh c + Duffy Fya Dombrock Doa C Fyb Dob e MNS M Joa E N Hy Kell K S LS LW Lwa k s Lwb Kpa Lutheran Lua Scianna Sc1 Kpb Lub Sc2 Jsa Diego Dia Hemoglobin S HbS Jsb Dib U (-) Kidd Jka Colton Coa Jkb Cob
 Kidd. Jka. Colton. Coa. Jkb. Cob.")
58
Results The antibody is anti-U (MNS5), not a warm autoantibody as was suspected at first.
, not a warm autoantibody as was suspected at first.")
59
Antigen Negative Units Requested:
Two U- (MNS5) units were deglycerolized and sent to hospital Deglycerolization Red cells are frozen with glycerol, a cryoprotective agent that prevents cellular damage and hemolysis as well as allows them to be frozen at < -65°C for 10 years. To deglycerolize, the red cells are warmed and then washed with decreasing % NaCl to remove the glycerol and then suspended for transfusion. Once thawed they have a shelf life of 24 hours (if an open system was used).
 units were deglycerolized and sent to hospital. Deglycerolization. Red cells are frozen with glycerol, a cryoprotective agent that prevents cellular damage and hemolysis as well as allows them to be frozen at < -65°C for 10 years. To deglycerolize, the red cells are warmed and then washed with decreasing % NaCl to remove the glycerol and then suspended for transfusion. Once thawed they have a shelf life of 24 hours (if an open system was used).")
60
U Antibody Characteristics
U (MNS5) Antibody U Antibody Characteristics History Anti-U was first described by Wiener et al in It was called “U” for the universal distribution of the antigen. Not ‘naturally occuring’ Clinical Significance ·Yes! Clinically significant ·Transfusion Reactions possible, mild to severe ·HDN possible, mild to severe Antibody ·IgG, reacts best at 37°C/AHG ·Autoanti-U is possible Other facts Some examples of anti-U are not compatible with all U- red cells. This is because some U- red cells are actually U variant and so have small quantities of U antigen. Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier.
 Antibody. U Antibody Characteristics. History. Anti-U was first described by Wiener et al in It was called U for the universal distribution of the antigen. Not ‘naturally occuring’ Clinical Significance. ·Yes! Clinically significant. ·Transfusion Reactions possible, mild to severe. ·HDN possible, mild to severe. Antibody. ·IgG, reacts best at 37°C/AHG. ·Autoanti-U is possible. Other facts. Some examples of anti-U are not compatible with all U- red cells. This is because some U- red cells are actually U variant and so have small quantities of U antigen. Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier.")
61
U Antigen Characteristics
U (MNS5) Antigen U Antigen Characteristics Occurrence Caucasians 99.9% Blacks 99% Well developed at birth Other Facts ·All U- individuals are S-s- but not all S-s- individuals are U-. ·The S-s- phenotype not common in the Caucasian population ·U negative phenotype is associated with absence of Glycophorin B (GPB) Variants U variant is possible Sources for further reading: ·Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier. ·Daniels, G. (2013) MNS Blood Group System, in Human Blood Groups, 3rd edition, Wiley-Blackwell, Oxford, UK.
 Antigen. U Antigen Characteristics. Occurrence. Caucasians 99.9% Blacks 99% Well developed at birth. Other Facts. ·All U- individuals are S-s- but not all S-s- individuals are U-. ·The S-s- phenotype not common in the Caucasian population. ·U negative phenotype is associated with absence of Glycophorin B (GPB) Variants. U variant is possible. Sources for further reading: ·Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier. ·Daniels, G. (2013) MNS Blood Group System, in Human Blood Groups, 3rd edition, Wiley-Blackwell, Oxford, UK.")
62
Genetics and Biochemistry
Genes encoding MNS system antigens reside on chromosome 4 Responsible for the production of glycophorin A (GPA) and glycophorin B (GPB) on red cells Photo:
 and glycophorin B (GPB) on red cells. Photo:")
63
Genetics and Biochemistry
Glycophorin A (GPA) M and N antigens GPA and GPB are the major sialic acid containing structures of the red cell membrane. Glycophorin B (GPB) S, s and U antigens Photo Source:
 M and N antigens. GPA and GPB are the major sialic acid containing structures of the red cell membrane. Glycophorin B (GPB) S, s and U antigens. Photo Source:")
64
U variants S-s-U+ or S-s-U+var
Almost exclusively in those of African Origin About 50% of S-s- are U+var Strength of expression is variable; adsorption/elution tests may be needed to detect the U antigen Strong correlation of U variant antigen cells being He+ (low frequency MNSs antigen).
.")
65
U vs U variants Reactivity GPB of the cell
The anti-U of S-s-U- will react with S-s-U+var The anti-U of U variants will not react with S-s-U- cells. GPB of the cell U- cells are totally GPB-deficient U variants have a variant GPB molecule that doesn’t express S or s

66
Case Study 3 Female, 65 years old African American DIAGNOSIS: stroke
PATIENT HISTORY Female, 65 years old African American DIAGNOSIS: stroke Patient had 45 minute seizure at nursing home before being transported to hospital. Speech was slurred upon arrival to emergency department with facial drooping. Patient has history of seizures, hypothyroidism, GERD, severe anemia, hypertension, congestive heart failure, etc. H/H: 9.9/ 32.1 Last transfusion was 10/27/2012 (>3 months)
")
67
Case Study 3 The sample was collected on 01/30/2013
Sample was sent to the reference laboratory Hospital Results on 1/30/2013: O Positive All cells reactive 2+ in gel Autocontrol not tested Additional history includes anti-Chido and antibody in Knops system from another facility.

68
Case Study Reference Lab testing: ABO/Rh performed: DAT Performed:
Anti-A Anti-B Anti-D A1 Cell B Cell ABO/Rh 4+ 0 Positive Anti-IgG/ tube Anti-C3/ tube 0√

69
Plasma + 1+ w+ 0√ D C c E e K k AHG-PeG Room Temp Kpa Kpb Jsa Jsb Fya
Rh System Kell Duffy Kidd Lewis P MNS Lutheran Room Temp AHG-PeG D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub + 1+ w+ 0√

70
Plasma + 1+ 2+ D C c E e K k M N S s Rh System Kell Duffy Kidd Lewis P
Lutheran GEL Cell D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub 1 + 1+ 2 3 4 2+ 5 6 7 8 9 10 11 Auto

71
Question to ask yourself: So where do we go at this point?
Serologic Problem Solving Question to ask yourself: So where do we go at this point? Let’s look at what we know: Phase of reactivity: AHG Strength/pattern of reactivity: pan-reactive, different strengths. Patient history: not recently transfused DAT/autocontrol: negative

72
Narrowed down possibilities: One antibody with different strengths
Serologic Problem Solving Question to ask yourself: So where do we go at this point? Narrowed down possibilities: One antibody with different strengths Multiple antibodies in plasma Keep in mind that patient has history of anti-Chido or antibody in Knops system

73
Some Techniques/Options Available:
Next Step: Use blood bank techniques, reagents and cells to try and determine the antibody Some Techniques/Options Available: Enzymes (ficin, papain, trypsin, etc) Chemicals such as DTT Phenotype Patient Rare antisera Rare cells
 Chemicals such as DTT. Phenotype Patient. Rare antisera. Rare cells.")
74
Patient phenotype Rh c + Duffy Fya C Fyb e MNS M E N Kell K S Kidd Jka
C Fyb e MNS M E N Kell K S Kidd Jka s Jkb Lewis Lea Leb

75
Some of the Selected Cells
Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub + 1+ Co(b+) 2+ w+
 2+ w+")
76
Ficin Panel + 1+ 2+ w+ D C c E e K k M N S s Rh System Kell Duffy Kidd
Lewis P MNS Lutheran GEL GEL-Ficin D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub + 1+ 2+ w+ Auto

77
0.2M DTT Panel + 1+ 2+ w+ D C c E e K k M N S s Rh System Kell Duffy
Kidd Lewis P MNS Lutheran GEL GEL-Ficin GEL-DTT D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub + 1+ 2+ w+ Auto

78
Patient History anti-Chido Knops Reactivity Ficin DTT Negative
Reactive Reactivity Ficin DTT Weakened Negative

79
Knops System Kna Knb McCa McCb Sla (Sl1) Yka Vil (Sl2) Sl3 Antigen
Occurrence Caucasian Blacks Kna 98% 99% Knb 4.5% <.01% McCa 94% McCb 0% 45% Sla (Sl1) 50-60% (30% West Africans) Yka 92% Vil (Sl2) 80% Sl3 100% Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier.
 50-60% (30% West Africans) Yka. 92% Vil (Sl2) 80% Sl3. 100% Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier.")
80
Available Selected Knops Cells
Rh System Kell Duffy Kidd Lewis P MNS Lutheran GEL D C c E e K k Kpa Kpb Jsa Jsb Fya Fyb Jka Jkb Lea Leb P1 M N S s Lua Lub + Yk(a-) 1+ Sl(a-) Appears to be anti-Sla but due to known weak reactivity of the antibody do molecular to confirm
 1+ Sl(a-) Appears to be anti-Sla but due to known weak reactivity of the antibody do molecular to confirm.")
81
Molecular Testing Rh c + MNS M Dombrock Doa C N Dob e S Joa E s Hy
MNS M Dombrock Doa C N Dob e S Joa E s Hy Kell K Lutheran Lua LW Lwa k Lub Lwb Kpa Diego Dia Scianna Sc1 Kpb Dib Sc2 Jsa Cromer Cra Jsb Colton Coa Knops Kna Knb Kidd Jka Cob McCa Jkb Cartwright Yta McCb Duffy Fya Ytb Sl1 Fyb Hemoglobin S HbS Sl2

82
Knops System Knops antigens are located on complement receptor 1 (CR1)
CR1 gene resides on chromosome 1

83
Complement Receptors

84
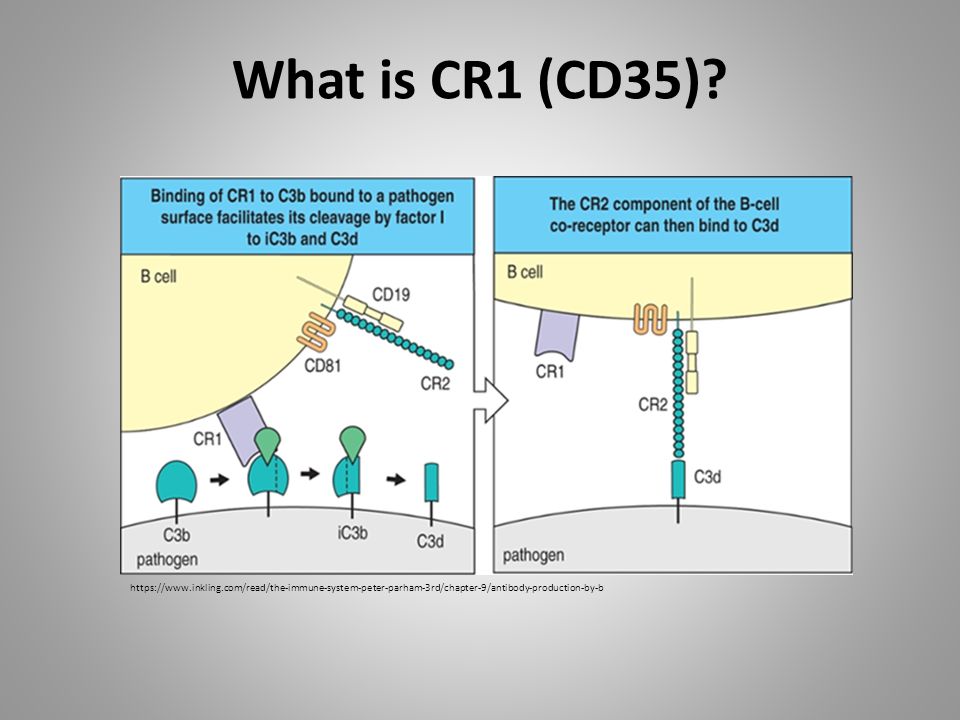
What is CR1 (CD35)? CR1 is a glycoprotein on cells that binds particles coated with C3b and C4b Neutophils and monocytes then phagocytize those particles and processes the immune complexes. These are transported to the liver/spleen for removal from circulation. Has inhibitory effect on complement activities by classical and alternative pathways so it protects the red cells from autohemolysis

85
What is CR1 (CD35)?
86
Structure of CR1 glycoprotein (CD35)
Knops system Structure of CR1 glycoprotein (CD35)
")
87
Knops system characteristics
Variation in antigen strength, related to CR1 red cell levels Generally, a reduction in antigen strength with storage of red cells as the CR1 copy per RBC may be decreased in stored samples High titer low avidity (HTLA) has been used to describe the antibodies Difficult to adsorb out antibodies Can be hard to distinguish antigen negative from weakly positive cells Clinically benign but can mask other significant antibodies
 has been used to describe the antibodies. Difficult to adsorb out antibodies. Can be hard to distinguish antigen negative from weakly positive cells. Clinically benign but can mask other significant antibodies.")
88
Knops antigens can be depressed in
Knops System Knops antigens can be depressed in cutaneous lupus erythematosus (CLE) Cold Hemagglutinin Disease (CHAD) Paroxysmal nocturnal hemoglobinuria (PNH) hemolytic anemia insulin-dependent diabetes AIDS some malignant tumors any condition with increased clearance of immune complexes Null phenotype: Kn(a-b-), McC(a-), Sl(a-), Yk(a-) aka Helgeson type
 Cold Hemagglutinin Disease (CHAD) Paroxysmal nocturnal hemoglobinuria (PNH) hemolytic anemia. insulin-dependent diabetes. AIDS. some malignant tumors. any condition with increased clearance of immune complexes. Null phenotype: Kn(a-b-), McC(a-), Sl(a-), Yk(a-) aka Helgeson type")
89
Sla Antibody Characteristics
History Reported in 1980 and named after Swain and Langely, the first two antibody producers. Clinical Significance No! Clinically insignificant ·No Transfusion Reactions ·No HDN Antibody ·IgG, reacts best at 37°C/AHG Other facts May be confused with anti-Fy3 because most Fy(a-b-) red cells are likely to be Sl(a-). Common antibody made by blacks. Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier.
 red cells are likely to be Sl(a-). Common antibody made by blacks. Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier.")
90
Sla Antigen Characteristics
Occurrence 98% 50-60% (30% West Africans) Other Facts Also known as Sl1 Disease processes causing red cell CR1 deficiency can lead to false negative antigen typing. Also, variability in antigen strength has been described. Sources for further reading: ·Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier. ·Daniels, G. (2013) MNS Blood Group System, in Human Blood Groups, 3rd edition, Wiley-Blackwell, Oxford, UK.
 Other Facts. Also known as Sl1. Disease processes causing red cell CR1 deficiency can lead to false negative antigen typing. Also, variability in antigen strength has been described. Sources for further reading: ·Reid, Marion and Christine Lomas-Francis (2012). The Blood Group Antigen FactsBook, 3rd Edition, Elsevier. ·Daniels, G. (2013) MNS Blood Group System, in Human Blood Groups, 3rd edition, Wiley-Blackwell, Oxford, UK.")
Similar presentations

 and Elution/Eluate Testing>")











SBB Blood Centers of the Pacific>")





>")