Download presentation
Presentation is loading. Please wait.

1
Day 2 Rev

2
Patient Safety First at GSMC!
Rev

3
Contact Beth Chrismer: Executive Director (1298)
")
4
National Focus on Patient Safety
Institute of Medicine report – “To Err is Human” (Nov. 1999) 44,000-98,000 deaths due to medical errors Annual cost $17B-$29B Federal Mandate and Regulatory Requirements -Presidential directive, The Joint Commission, Centers for Medicare & Medicaid Services, State regulations
 44,000-98,000 deaths due to medical errors. Annual cost $17B-$29B. Federal Mandate and Regulatory Requirements. -Presidential directive, The Joint Commission, Centers for Medicare & Medicaid Services, State regulations.")
5
Basics of Patient Safety
Actions undertaken by individuals and organizations to protect health care recipients from being harmed by the effects of health care services.

6
The Case for Patient Safety
Patient safety is a critical component of quality Health care is NOT as safe as it should be People do not come to work with the intent to hurt patients We are human therefore mistakes will occur When mistakes do occur we want there to be no harm Speak-up for patient safety

7
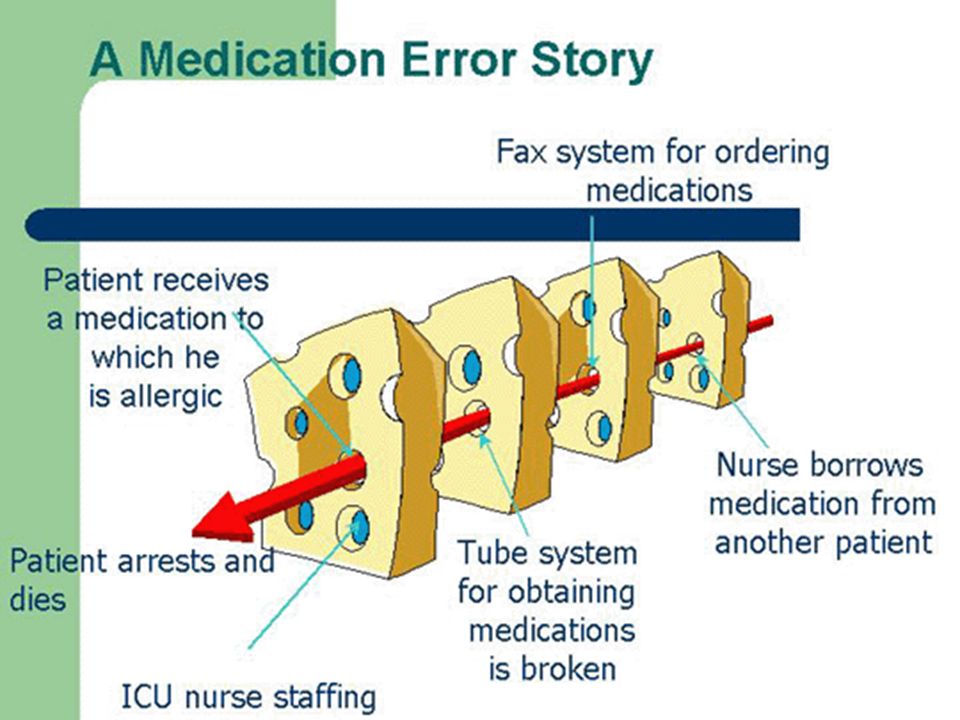
Patient Safety System

8
Patient Safety First at GSMC!
Patient safety is a priority at Good Shepherd Medical Center. Our staff and physicians are committed to improving quality of life and providing safe and healthy surroundings for patients, visitors, and staff. Many procedures are in place to protect the well-being of our patients and to secure the best medical outcome possible. Everyone has a role in patient safety.

9
Safety as Our Core Value

10
The Patient’s Perspective
Don’t hurt me Heal me Be nice to me

11
Culture and Safety Culture Behaviors Outcomes
is the shared values and beliefs of the individuals in the organization (the way we act when no one is looking) Behaviors Outcomes
 Behaviors. Outcomes.")
12
Take Action to Reduce Risk
Proactive: Monitor patient safety and redesign high-risk processes to prevent an event from occurring. Reactive: Investigate significant patient incidents.

13
Culture of Safety Root Cause Analysis Based on findings we:
We intensely analyze any error that does occur. Based on findings we: Redesign systems Test new designs Educate staff on changes Follow-up to see if new design is effective

15
Encourage patients, families, staff and physicians to report safety concerns on the hotline
Close calls, near misses, share ideas Available 24 hours a day, 7 days a week Anonymous Leave name and number for follow-up Ideas of merit qualify for recognition or rewards

16
Rapid Response Team

17
Rapid Response Team The Five Million Lives Campaign by the Institute for Healthcare Improvement encourages healthcare organizations to implement a rapid response team. In 2006 Good Shepherd implemented a rapid response team. The goal is to respond to a “spark” before it becomes a “forest fire.” To prevent deaths in patients who are failing outside intensive care settings.

18
Rapid Response Team Call early, Call often
Call Rapid Response anytime you are worried about the patient! Clinical and non-clinical staff, patients and families can activate the Rapid Response Team. The team can respond and assist with stabilizing the patient before a cardiopulmonary or respiratory arrest occurs. Call early, Call often

19
The Josie King Story Josie King, an 18 month old little
girl, died from medical errors in one of the best hospitals in our country. Josie was the sister of Jack, Relly, and Eva and beloved daughter of Tony and Sorrel. She died as a result of a series of hospital errors and poor communication. Through the creation of a patient safety program, it is the King family’s hope to prevent this from ever happening to another patient.

20
Josie King Foundation - Condition “H” (Condition Help)
University of Pittsburgh Medical Center - UPMC Shadyside and Children’s Hospital of Pittsburgh worked with the King family to develop the nationally recognized model known as Condition H. Condition H was created to address the needs of the patient/family in case of an emergency or when the patient is unable to get the attention of a healthcare provider in an emergency situation. The call provides immediate help when: they feel they are not receiving adequate medical attention; or if they become concerned with what is happening. The program was designed to be a safety net for patients. In many cases, it is the family who knows the patient better than we do. When Condition H is called, a rapid response team arrives to the patient’s bedside within minutes.

21
Condition “H” (Condition Help) at Good Shepherd
 at Good Shepherd")
22
Partnering for Safety When patients partner with the health care team, it helps us ensure a safer health care experience for all of us. Patients are encouraged to be actively involved in their own care for safety reasons.

23
Involve Patients in Care
Our Patients-Our Partners: One Team, One Goal A few ways we involve patients in care… Educate the patient and/or family about hand hygiene, respiratory hygiene, contact precautions Educate surgical patients about how we prevent adverse events during surgery Inform patients/families how they can report safety concerns by calling Condition H, Patient Safety Hotline (BUZZ), Guest Relations or The Joint Commission
, Guest Relations or The Joint Commission.")
24
2012 National Patient Safety Goals
The purpose of the Joint Commission’s National Patient Safety Goals (NPSGs) is to promote specific improvements in patient safety. The goals are revised on an annual basis and highlight problematic areas in health care and describe evidence and expert-based solutions to these problems. By addressing problems, organizations can promote patient safety and prevent sentinel events. A sentinel event is an unexpected occurrence involving death or serious physical or psychological injury.
 is to promote specific improvements in patient safety. The goals are revised on an annual basis and highlight problematic areas in health care and describe evidence and expert-based solutions to these problems. By addressing problems, organizations can promote patient safety and prevent sentinel events. A sentinel event is an unexpected occurrence involving death or serious physical or psychological injury.")
25
2012 National Patient Safety Goals
Goal 1 Improve the accuracy of patient identification Goal 2 Improve the effectiveness of communication among caregivers Goal 3 Improve the safety of using medications Goal 7 Reduce the risk of healthcare-associated infections Goal 8 Accurately & completely reconcile medications across the continuum of care Goal 15 The hospital identifies safety risks inherent in its patient population UNIVERSAL PROTOCOL: The organization meets the expectations of the Universal Protocol for Preventing Wrong Site Surgery Note: Some goals and requirements appear to be misnumbered or missing from the numerical sequence. This in not a typographical error. Some goals do not or no longer apply to hospitals and therefore have not been included.

26
Improve the Accuracy of Patient Identification
To make sure the right person is receiving the intended care, treatment, and services we must use at least two patient identifiers. Name Birthdate When confirming a patient’s name, staff members should not state the name and ask the patient to confirm it. Instead, staff members should ask the patient to state his or her name and birthdate.

27
Reduce the Risk of Healthcare-Associated Infections
CDC Guidelines Alcohol-Based Hand Sanitizer when hands are not visibly soiled apply to palm of hand and rub hands together covering all surfaces of hands and fingers until hands are dry Soap and Water when hands are visibly soiled patient has Clostridium Difficile (C-Diff) after going to the restroom before eating at least a 15-second scrub Gloves the use of gloves does not eliminate the need for hand hygiene and hand hygiene does not eliminate the need for gloves
 after going to the restroom. before eating. at least a 15-second scrub. Gloves. the use of gloves does not eliminate the need for hand hygiene. and hand hygiene does not eliminate the need for gloves.")
29
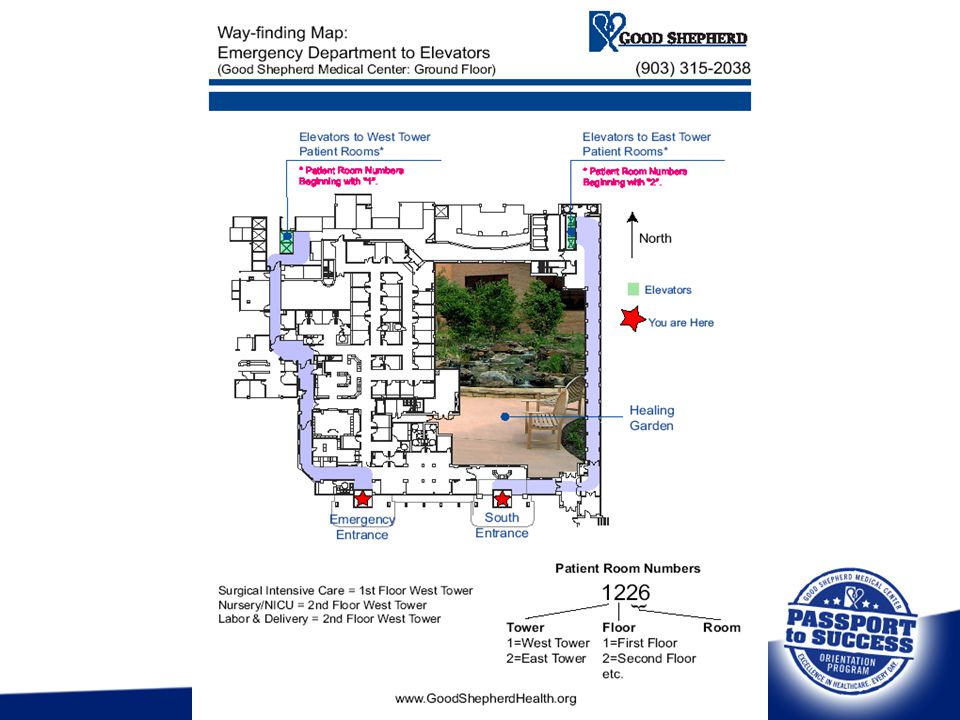
Fall Prevention Patients at risk for falls have a yellow “Fall Risk” armband applied and a magnet placed outside the patient’s door. The patient receives a pair of treaded socks. All efforts are made to move the patient as close as possible to the nurses desk. Family or friends are encouraged to stay with patient, if unable may consider a sitter. Communicate “at risk” patients during patient report and hand off between units.

30
Is Everybody’s Business
Questions?

31
Medical Error Reporting
The Medical Error Hotline is a voic line available 24 hours a day providing complete anonymity. Employees may use this line to report concerns regarding a medical error was not documented, reported or addressed appropriately.

32
Variance Reporting Rev

33
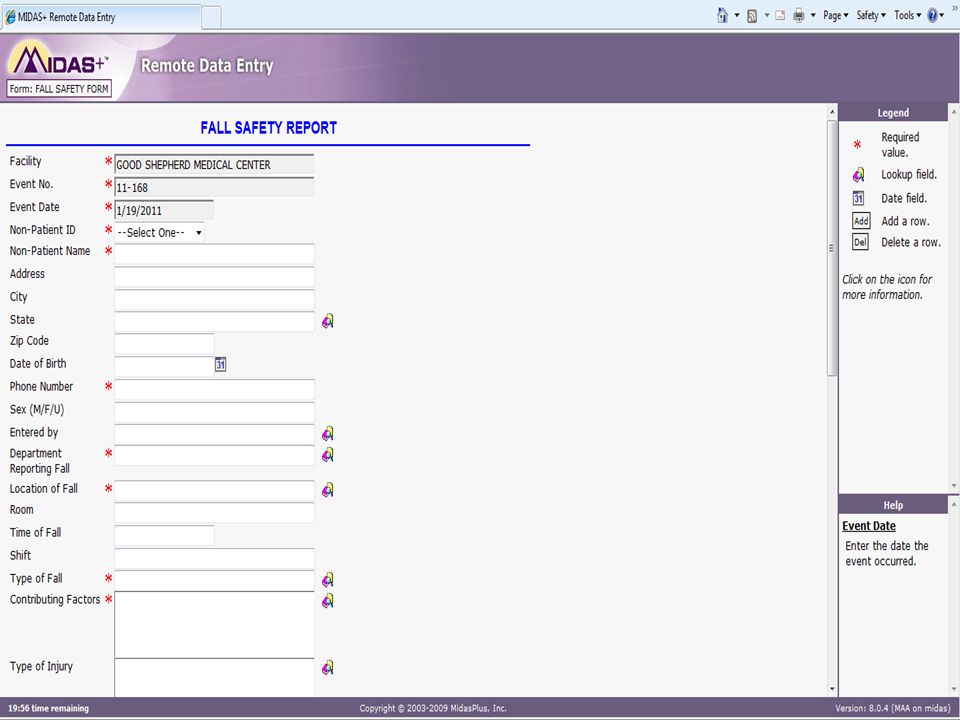
Variance Reporting Hospital employees and medical staff members participate in a hospital wide variance reporting program. Types of Variance Reports: Falls – Fall Safety Report Medication Errors – Medication Safety Report Other occurrences not in the above categories – Variance Report

34
Variance Reporting Variance Reports are to be initiated by hospital staff members or employees involved in or identifying occurrence. All questions or sections of the report must be completed. Descriptions should be brief, factual and objective. Patients, visitors and employees who sustain injuries will receive medical attention. On-line system allows anonymous reporting.

35
Variance Reporting Variances are reported directly from the occurrence area to the supervisor, manager or director. Managers should investigate pertinent issues reported with a brief summary in the online-system Variances are routed to Risk Management within 96 hours of the occurrence. Variance Reports will be trended and reviewed by Risk Management. Variance Report Forms are found on GSnet To Access for – GSnet – Var Rpts Variance Reports are never to be duplicated.

36
Variance Reporting Examples of occurrences that should be reported on the Variance Report: Mishaps due to faulty/defective equipment Unexpected adverse results of professional care or treatment – death, brain damage, physical loss or impairment, etc. Unprofessional, threatening or inappropriate conduct of health professionals or employees Patients leaving against medical advice Thefts, burglaries and vandalism on hospital premises

38
Impaired Provider Rev

39
Impaired Provider What is impairment?
The inability to “practice with reasonable skill and safety” because of: Physical illness or condition Mental disorder Alcohol or drug abuse Disruptive behavior Sexual misconduct/boundary violations Burnout

40
Impaired Provider Examples of disruptive behavior:
Bullying or demeaning behavior Sexual harassment Abusive treatment of patients or staff Profanity or disrespectful language Repeated violations of rules and policies Physical attacks, hitting, pinching Improper comments/illustrations in medical record Threatening to get someone fired

41
Impaired Provider Healthcare Practitioner Code of Conduct
Provides guidance to ensure work is done in ethical manner Also referred to as Code of Ethics

42
Impaired Provider Reporting impaired practitioners and disruptive behavior: Document specific examples and patterns of disruptive behavior Anyone may report an impaired provider or disruptive behavior to Executive Management Complaints are investigated by Human Resources Executive Management may identify involved practitioners to the Committee on Physician Health (CPH) Identity of reporting individual kept anonymous unless individual gives permission to disclose Retaliation against reporting individuals is grounds for immediate referral to the Executive Committee for corrective action.
 Identity of reporting individual kept anonymous unless individual gives permission to disclose. Retaliation against reporting individuals is. grounds for immediate referral to the. Executive Committee for corrective. action.")
43
Safety Sense: Occupational Injury Benefit Plan
Rev

44
What is SAFETY SENSE? Good Shepherd Health System (GSHS) DOES NOT have workers’ compensation insurance coverage for work-related injuries GSHS is a “non-subscriber” to workers compensation, and does provide medical, death, dismemberment and wage replacement benefits to employees who sustain injuries or occupational diseases in the course and scope of their employment. The GSHS plan is called SAFETY SENSE

45
New Plan Effective Aug. 17, 2009 Our new plan was effective 8/17/09 and provides similar benefits to workers Medical care for injured employees will be provided at the GSMC Occupational Medicine Clinic. GSMC Emergency Dept. is for true emergencies. Injuries must be reported within 24 hours of occurrence using the Accident Investigation Report A urine drug screen is required for injuries that need medical treatment.

46
SAFETY SENSE: Benefits Available
Medical care at Occupational Medicine, specialty referrals, therapy, and diagnostic testing, as needed, through Occ Med provider. Light duty accommodations for employees placed on restricted duty Wage replacement at 75% of salary for employees taken off of work after 32 hours of lost time.

47
Acknowledgement of SPD
A Summary Plan Description (SPD) of the SAFETY SENSE Occupational Injury Benefit Plan is provided to you by clicking the link on GSNet under “Work-Related Injury” in the Policies section. Spanish and English versions of the SPD are available on GSNet. Please review the plan, print a copy, if you like. If you are unable to print a copy and desire a copy, one can be provided to you by calling the phone numbers given below. You have been provided with information about the GSHS SAFETY SENSE plan and agree to comply with the Plan. Please contact Beth Chrismer - (903) for questions.
 of the SAFETY SENSE Occupational Injury Benefit Plan is provided to you by clicking the link on GSNet under Work-Related Injury in the Policies section. Spanish and English versions of the SPD are available on GSNet. Please review the plan, print a copy, if you like. If you are unable to print a copy and desire a copy, one can be provided to you by calling the phone numbers given below. You have been provided with information about the GSHS SAFETY SENSE plan and agree to comply with the Plan. Please contact Beth Chrismer - (903) for questions.")
48
Patient Rights Rev

49
Patient Rights When and where are patients informed of their rights? At the time of Registration Rights include: Considerate and Respectful Care Advance Directives Confidentiality Hospital Policy & Procedures Patient Complaint Process

50
Patient Rights Notice of Patient Rights posted in Registration area and available on Ethics Committee – Good Shepherd Medical Center Ethics Committee’s goal is to facilitate ethical reflection and decision making by persons involved in the case, focusing on the patient’s values and wishes versus imposing a decision. Their role is consultative in nature rather than decision making. (consent/refusal to treatment, withholding life support, DNR) Chaplain, nurse, physician and others convene to render decision. Decision can be accepted or denied Contact your Supervisor to convene the Ethics Committee
 Chaplain, nurse, physician and others convene to render decision. Decision can be accepted or denied. Contact your Supervisor to convene the Ethics. Committee.")
51
Environment of Care and Safety
Rev

52
Contact Tina Collins: Medication Safety (3612)
Chris Bland: Safety Manager (5163)
")
53
Environment of Care Disciplines of the Environment of Care Safety
Security Hazardous materials Emergency Management Fire Safety Medical Equipment Utilities

54
Environment of Care The Safety Management Plan at Good Shepherd Medical Center provides a process to effectively manage and reduce safety-related risks to patients, staff, and visitors.

55
Environment of Care Safety Management Goals
Comply with all safety-related regulatory requirements. Provide a safe, secure, and therapeutic environment for patients, staff, and visitors. Integrate safety practices into daily operations. Identify opportunities to improve performances in the safety management program.

56
Environment of Care This facility has an
Environment of Care Committee (EOCC) that monitors training and competence of staff and assesses physical and operational conditions of the infrastructure and grounds and equipment through building inspections, environmental rounds, safety inspections, and various performance improvement initiatives.
 that monitors training and competence of staff and assesses physical and operational conditions of the infrastructure and grounds and equipment through building inspections, environmental rounds, safety inspections, and various performance improvement initiatives.")
57
Healthcare Security Functions of security include the following:
To protect staff, patients, visitors, and property. To investigate and record incidents, thefts, disturbances, vandalism, accidents, and traffic accidents. To provide special services including escorts, battery boosts, and lock and unlock doors. To respond to emergencies such as fire, disaster, and bomb threat.

58
Healthcare Security Phone numbers for Security
Security: ext. 3376/2196 FAX: ext. 1153 If you are inside the hospital, you may dial “0” and ask the operator to call Security on the radio. (Preferred method)
")
59
Healthcare Security Secure your valuables
Lock valuables in work areas. Keep valuables out of sight in your car or trunk. Weapons – No weapons (firearms, clubs, knives with long blades) may be carried on property. Escorts and Parking Lot Safety– always try to walk with a group, rather than alone, to your vehicle. Use the “Buddy System.”
 may be carried on property. Escorts and Parking Lot Safety– always try to walk with a group, rather than alone, to your vehicle. Use the Buddy System.")
60
Healthcare Security Badges – always wear your ID badge.
Badges must be either worn on the upper left chest by being attached to a collar, lapel or shirt pocket or attached to a GSHS approved lanyard. Badges are that are damaged due to misuse, wear and tear or are lost will be replaced at a charge of $5.00 to the employee. Badges are also to be used as access cards for the employee parking lots. Suspicious persons or activities – Report any suspicious persons or activities immediately by calling “0” and alerting the operator or call security at x3376.

62
Fire Safety General Guidelines
To report a fire, call 3000 and report CODE RED Enforce “no smoking” rules. Use only approved extension cords. Keep flammable materials away from ignition sources. Enforce policies about unauthorized appliances and equipment. Keep general housekeeping in order. Report or correct any fire hazards.

63
Fire Safety Extension Cords Use only approved extension cords.
Cords must have a grounded plug. Use the correct cord for the load and protect the cord from traffic. Be sure extension cords are in good working condition. Do not overload electric sockets or extension cords.

64
Fire Safety Flammable Materials
Keep flammable materials away from ignition sources. Class A fires involve normal combustibles such as wood, cloth, paper, rubber, upholstery, and plastics. Class B fires are related to flammable liquids, gases and greases, such as oils, paints, and gasoline. Class C fires are related to electrical equipment such as fuse boxes, circuit breakers, machinery, and appliances… computers, televisions and mechanical equipment.

65
Fire Extinguishers Fire Safety
All extinguishers in this hospital are rated for Class A, Class B, or Class C fires. Good Shepherd uses the PASS method of operating a fire extinguisher: Pull the pin Aim at the base of the flame Squeeze the handle Sweep from side to side

66
Fire Safety Good Shepherd uses the RACE method of dealing with a fire: Rescue (Move Patients past 1st Fire Door) Alarm (Pull Station or Call Operator) Contain Fire Extinguish/Evacuate
 Alarm (Pull Station or Call Operator) Contain Fire Extinguish/Evacuate")
67
Emergency Preparedness
Code Words Emergency number 3000 use for all emergencies Operation Baker – Emergency Evacuation Code Gray – Bomb Threat Code Adam – Abduction in the hospital Code Yellow – Bioterrorism event Code Black – Tornado Code Red – Fire Code Blue – Cardiac Arrest Code Pink – Neonatal Resuscitation Code Stroke – Reponse to Stroke Patient Operation Able – Mass Casualty Charlie Brown – Combative individual Duress Word – ADVICE

68
Operation Baker - Evacuation
Operation Baker is the implementation of strategic or urgent evacuation of patients and other persons from the Medical Center or grounds. Assist all patients and visitors out of the building. Be aware of all evacuation routes in your area.

69
Bomb Threat Code Gray

70
Bomb Threat – Code Gray Employees in the immediate area of the bomb should remember: Search for and report any suspicious objects. DO NOT move, jar, or touch the object or anything attached to it. Check public access areas, such as restrooms, telephone booths, ER, lobby, and patient rooms first. DO NOT turn lights on or off. Turn off all two-way radios, cell phones and pagers.

71
Abduction in the Hospital - Code Adam
Denotes an abduction from the hospital If an employee suspects an abduction, they should call 3000 and report Code Adam with a description of the person who was abducted (age, sex, race, etc.) All employees should search the area and detain visitors until an all clear is announced. NATIONAL CENTER FOR MISSING AND EXPLOITED CHILDREN says “Prevention is the best defense against infant abductions” HUGS Infant Security System
 All employees should search the area and detain visitors until an all clear is announced. NATIONAL CENTER FOR MISSING AND EXPLOITED CHILDREN says. Prevention is the best defense against infant abductions HUGS Infant Security System.")
72
Bioterrorism - Code Yellow
A substantial influx of patients with illnesses that are uncommon in nature should be suspect. Code Yellow will be called when it is determined these illnesses are a result of a bioterrorist event (such as anthrax, etc.). Infection control should be notified immediately, and all personnel in areas that provide initial treatment to patients should be aware of department specific treatment protocols.
. Infection control should be notified immediately, and all personnel in areas that provide initial treatment to patients should be aware of department specific treatment protocols.")
73
Code Black can be proceeded by : Operation Weather Watch
Tornado - Code Black A tornado has been spotted within a five mile radius of the Medical Center. Patients should be moved to inside corridors and away from windows until an all clear is announced. Code Black can be proceeded by : Operation Weather Watch move to state of readiness alert visitors to weather conditions review Code Black procedures

74
Fire - Code Red Fire or smoke situation which requires activation of the fire response plan. Respond to a fire by calling the emergency number 3000 or activate the fire pull in your area. Locate all exits and evacuation plans for your work area to be prepared for an emergency.

75
Cardiac Arrest - Code Blue
Code Blue is called when a patient suffers cardiac arrest. This code is called by calling 3000 and stating Code Blue and the location or patient room. The Code Blue team reports to the location announced and starts resuscitation efforts.

76
Mass Casualty – Incident Operation Able
Hospital expects large number of patients to be treated due to the incident. Major Disaster Response Plan will be implemented upon announcement of “Operation Able”. All departments should implement their department-specific response plans for appropriate action.

77
Combative Individual – Code Charlie Brown
Charlie Brown alert is issued for a combative individual with security responding to subdue the individual. Employees should balance or offset the person’s behavior with a helpful, calming response. If the behavior becomes violent, call the emergency response team by contacting 3000, stating “Charlie Brown” and giving them the location of the event.

78
Emergency Response Team
The staff member initially involved with the combative person and the Charge Nurse become team leaders. Uses the least force necessary to physically quiet or restrain combative individual. Notify treating physician or ER physician to secure order for restraint and/or medication. The team leader or their designated staff notifies the hospital operator of the situation and location by calling “Charlie Brown” to x3000.

79
Duress Word – “Advice” Hostage situation – The duress word to alert the operator of a hostage situation is ADVICE. All calls should include the word ADVICE and the CEO’s name with as many details possible – number of people, weapons, number of attackers, etc. (Example: This is Mr. Williams. I am in the Personnel Office with four people. Please contact Mr. Banos. I need his Advice. Have Mr. Banos contact me at this phone number, 2130, with the advice.)
")
80
Hostage Situations Immediately notify appropriate department to report situation and its location. Remove people from the area if it can be done in a safe manner without drawing attention to the hostage taker. Assist in preventing other staff, visitors, and/or patients from entering the area. Identify number of hostages and any suspects. DO NOT call out the emergency code. Call Executive Management and use code word ADVICE.

81
Electrical Safety When normal power is interrupted, and emergency power system takes over. The system is powered by diesel-fueled generators. The emergency power system comes online within 10 seconds when normal power is interrupted. Plugs for emergency power are to be easily seen. (red-outlets) Ivory outlets: Normal power-general purpose.
 Ivory outlets: Normal power-general purpose.")
82
Utilities Management Utilities at Good Shepherd are protected by back up provisions in case they fail. Emergency Power System – takes over when normal power is interrupted. Emergency system is powered by seven generators – four in the hospital and two in the Medical Plaza and one in the Customer Service Center. Plugs for emergency power are either red or labeled appropriately.

83
Utilities Management Water Outage – follow the Emergency Water Supply Plan in your Safety Manual to minimize the impact on patients.

84
Utilities Management Fire Detection System
The Plant Operations Department has a fire detection system that is computerized and monitored 24 hours a day. These systems are routinely inspected and tested annually. On the individual unit or floor, you have a: Pull station Smoke detector Fire extinguisher Chiming light or horn and light Fire doors

85
Other Utilities-Elevators
30 Elevators in use in the facility Elevators are a very safe mode of transportation Always practice proper elevator etiquette.

86
Medical Equipment Management
Know where the shut-off valves and zone valves are located when working with oxygen, vacuum, and medical air. Be prepared to shut off valves as instructed during a fire.

87
Safe Medical Device Act
Medical Equipment Management Safe Medical Device Act A means for reporting equipment that could or has caused or contributed to the death or permanent injury to a patient. When discovered, immediately notify supervisor and/or the Risk Manager. The equipment must be reported to the FDA within 10 days.

88
Medical Equipment Management
If there is any chance the equipment has harmed a patient in any way remove the item from service immediately, with accessories. label it as defective complete an incident report. DO NOT try to repair it yourself, and do not allow it to be worked on or examined by someone else. Immediately report malfunctioning equipment to BioMed at x4532.

89
Medical Equipment Management
All equipment is inspected periodically by Bio-Medical Services. The Biomed Shop contains a library of operator and service manuals for equipment and spare parts for critical life support equipment CALL x4532 7:00 a.m. to 4:30 p.m. M-F After hours, On-Call BMET is available by calling the operator

90
When are Interim Life Safety Measures Taken?
Construction areas Locations near construction All buildings that do not meet current life safety codes Implemented if construction restricts, impedes or changes personnel emergency exit routes or affects fire detection/suppression systems.

91
Hazard Communication All hazardous materials have a Material Safety Data Sheet (MSDS) available through your department, your supervisor or on GSnet Right to Know assures employees are aware of possible exposures in their work environment All hazardous materials must have a label naming the chemical and have adequate hazard warning. Report any unlabelled containers to your supervisor.

92
Hazard Communication The National Fire Protection Association’s (NFPA)
placard system provides a simple system of hazard identification. The placard is diamond in shape. (blue, red, white, yellow) Color coded for type of hazard. Number coded for severity of the hazard.
 Color coded for type of hazard. Number coded for severity of the hazard.")
93
Hazard Communication Keep disposable empty compressed gas cylinders separate from other trash and secured in the proper location for your area. Cylinders should be chained or secured when not in use Dispose of cylinders as directed at your facility.

95
Spills or Leaks of Known Hazardous Substances
Hazard Materials Spills or Leaks of Known Hazardous Substances Take the following actions for spills or leaks of a known substance: Immediately secure the area Request assistance from Environmental Services Environmental Services has trained personnel to clean spills – hazardous and unknown. They will obtain special equipment (spillkits, mops, towels, etc.

96
Spills or Leaks of Unknown Substances
Hazard Materials Spills or Leaks of Unknown Substances For spills or leaks of an unknown substance, you should: Isolate the area from public and all non-essential persons. Secure the area Request assistance Determine the nature of the material Contain the spill or leak

97
Hazardous Material Response Team
The team is responsible for responding to all spills housewide 24 hours a day. The team is comprised of: EVS Personnel Safety Manager Security Lab Plant Operations (if spill is on grounds) Other Personnel as needed
 Other Personnel as needed")
98
Hazardous Material Response Team
Good Shepherd has policies on GSNet in the HazMat Manual on hazardous materials and spills. Nursing has policies on GSNet regarding chemotherapy safe handling and usage.

99
HOW DO CHEMO SPILLS AFFECT ME?
Environmental Services -Cleans spills greater than 5cc Nursing - Cleans spills less than or equal to 5 cc & reports spills greater than 5cc by calling 3000.

100
Blood or Body Fluid Spills
Hazard Materials Blood or Body Fluid Spills Minimize your risk of exposure by containing, removing, and disinfecting all blood or body fluid spills as quickly and effectively as possible. Wear gloves and other appropriate Personal Protective Equipment (PPE). Use a dry absorbent material to Solidify larger fluid volumes Transform them into an easily handled semi-solid state
. Use a dry absorbent material to. Solidify larger fluid volumes. Transform them into an easily handled semi-solid state.")
101
Hazard Materials Eyewash Station
Employees who may be exposed to hazardous corrosive chemicals should know how to use emergency eyewash equipment. If the spill is on protective equipment, remove the equipment (gloves, glasses, goggles, clothing) after the eyewash is activated. Rinse away chemicals remaining on the equipment.
 after the eyewash is activated. Rinse away chemicals remaining on the equipment.")
102
Radiation Safety Distance and Shielding
Two techniques for reducing dose rate are Distance Shielding Mobile units - six feet Maximizing the distance between the source and the worker decreases exposure significantly.

103
Radiation Safety Dosimeters
Leave the badge at work in a specified location at the end of each day. (one month wear) Use dosimeters only for measuring an occupational dose. Do not wear the dosimeter if you are receiving medical or dental exposures as a patient. Protect from extreme temperature changes, humidity and chemicals Do not expose to water or liquid
 Use dosimeters only for measuring an occupational dose. Do not wear the dosimeter if you are receiving medical or dental exposures as a patient. Protect from extreme temperature changes, humidity and chemicals. Do not expose to water or liquid.")
104
Body Mechanics Injuries on the job can be prevented by using the Five Principles of Body Mechanics. 1. Posture – keep your chin level and slightly tucked, keep chest up but not out, stomach muscles tight, knees not locked 2. Keep objects close to your body 3. Face the object 4. Symmetry – use both sides of your body equally, use both hands whenever possible 5. Wide base of support Standing – Legs should be at least shoulder-width apart. They can be either side to side or one in front of the other. Sitting – Keep weight evenly distributed.

106
Respecting Cultural Diversity
Rev

107
Contact Joey Sutton: Care Direct Coordinator (3612)
Jeanie McKay: Director of Organizational Development (5276)
")
108
Cultural Diversity Good Shepherd Medical Center represents a diverse population of people from our staff to our patients. You will be asked to take a new look at the population served by learning about cultural values, beliefs, norms, and practices of particular cultural groups.

109
Cultural Diversity Keys to Success:
Communication Styles – be sensitive to body language when addressing patients: Facial expressions – frowning, smiling, etc. Gestures – pointing, hand signals, etc. Example: American people widen their eyes to show anger, Chinese people narrow theirs. Some cultures view making eye contact as rude versus being polite. Personal Space – be aware of the dynamics of your impact on: Distance - backs a way Touch – May want or not want to be touched Example: American culture expects people to stand about an arm’s length apart when talking, Hispanics favor being closer and moving away might be perceived as being “cold.” Relevance of Time Immediate versus later Recognize that differences in time consciousness may be cultural and not a sign of laziness or resistance.

110
Cultural Diversity GSMC supports Cultural Diversity by:
Religion -Chaplaincy services available for all denominations Language – Cyracom telecommunication for over 300 languages, ASL, interpreters. Food Requests – Special diets available on request.

111
Cultural Diversity All people are NOT alike regardless if they are of the same culture. Avoid stereotyping people.

112
Population Specific Rev

113
Population Specific AGE GROUPS: Neonates - birth – 6 months
Infants – 6 months – 12 months Toddlers – 1 year – 4 years Preschooler – 4 years – 6 years School age – 6 years – 12 years Adolescent – 13 years – 18 years Adult - 19 years – 65 years Geriatric – 65 years old and beyond

114
Population Specific Neonates: birth – 6 months Smile
Follow objects with eyes Maintain head control

115
Population Specific Infants: 6 months – 12 months
Increased development of the arms and legs Babies become familiar with their bodies by putting hands and feet in mouth

116
Population Specific Toddlers: 1 year – 4 years
Significant people are parents May appear afraid of strangers Very active Use play to learn

117
Population Specific Preschooler: 4 years – 6 years
Short attention spans and a lot of energy Curious and imaginative Afraid of being in hospital, the dark, and pain

118
Population Specific School age: 6 years – 12 years
Knows the difference between fantasy and reality Have a strong need to follow rules Act younger than they are

119
Population Specific Adolescent: 13 years – 18 years
Do not like to ask questions for fear of appearing “stupid” Can react with anger when frustrated Peer identity is very important

120
Population Specific Adult: 19 years – 65 years
Early Adulthood – Manages a household, rears children, develops career Middle Adulthood – Accepts physical changes, maintains a healthy lifestyle, plans for retirement

121
Population Specific Geriatric: 65 years old and beyond
Bones become more fragile and fracture more easily May have decreased vision and hearing May be depressed related to a decrease in their physical abilities

122
Population Specific Population specific skills are the skills used to give the care and attention that meets an individual’s needs. Each individual has his or her own likes and dislikes, feelings, thoughts, beliefs, life experiences and abilities. Experts have determined that these qualities are similar according to a person’s age or stage of life. When we understand these stages of life, we improve the care and attention given to patients, families, and visitors.

123
Spiritual Care Rev

124
Offered to all patients, families, staff and volunteers:
Spiritual Care Offered to all patients, families, staff and volunteers: Non-denominational spiritual counselor providing spiritual support and counseling Bereavement support Sacraments On-call clergy available for pastoral care Stress management Services for special occasions Chapel – First floor, across from Waiting area

125
Offered to all patients, families, staff and volunteers:
Spiritual Care Offered to all patients, families, staff and volunteers: Pre-operative patients and family members Patients who have religious/spiritual requests Patients, families and/or staff experiencing emotional/spiritual distress

126
Spiritual Care A spiritual care consult can be obtained by:
Physician Order Employee/Volunteer request Patient/Significant other request Consult the Chaplain through phone extension 2636, Pager # Or Through the hospital operator

127
Death and Dying Rev

128
Palliative Care Starts in the initial phase of the disease process, and continues through this process until cure, remission, or death occurs. In palliative care, no specific treatment is excluded, from curative treatments to resuscitation; however, emphasis remains on comfort care of the patient and the needs of the family dealing with a life-altering disease process.

129
Hospice Care Hospice is primarily a concept of care, not specific place of care. Hospice emphasizes palliative rather than curative treatment; quality rather than quantity of life. Professional medical care is given, and sophisticated symptom relief provided. The patient and family are both included in the care plan and emotional, spiritual and practical support is given based on the patient’s wishes and family’s needs.

130
Abuse and Neglect Rev

131
Abuse, Neglect & Exploitation
As a skilled caregiver your responsibility includes: To know when you see a victim of abuse To offer the care needed To report: Social Services Nursing Supervisor Texas Department of Protective Services

132
Abuse, Neglect & Exploitation
Forms of Abuse Self – does not care for basic needs , unfilled prescriptions, does not eat properly or has poor grooming habits Caretaker – Neglect or dependent child/adult Emotional –Spoken threats, aggressive behavior Physical- Hitting, kicking, throwing Sexual – Sexual harassment, sexual assault Exploitation – Taking advantage of or misuse of patients personal belongings, including finances

133
Abuse, Neglect & Exploitation
Signs of Neglect Poor hygiene Body lice Dehydration Unfilled prescriptions Malnutrition Failure to thrive Basics – necessities of life, housing, clothing, nutrition, medical care, needs supervision Munchausen Syndrome by proxy

134
Violence in the Workplace
Rev

135
Violence Cycle of Violence Tension Building Phase Honeymoon Phase

136
Domestic Violence A Healthcare Issue
25-30% of women presenting to the ER are current or formerly battered women 2.2 – 3.1% of patients (700,000 – 1.1 million) in the ER present with abuse related trauma Abused woman account for 64% of all female psychiatric inpatients 18 – 32% of pregnant women are abused
 in the ER present with abuse related trauma. Abused woman account for 64% of all female psychiatric inpatients. 18 – 32% of pregnant women are abused.")
137
Violence All adult patients in the ED and in the Inpatient Units are screened for domestic violence Victims are offered the resources of the Women’s Center and Shelter or the Texas Department of Protective Services.

138
Violence in the Workplace
Health care and social service workers face an increased risk of work-related assaults stemming from several factors, including: The prevalence of handguns and other weapons among patients, their families or friends. The increasing number of acute and chronically mentally ill patients now being released from hospitals without follow-up care, who now have the right to refuse medicine and who can no longer be hospitalized involuntarily unless they pose an immediate threat to themselves or others.

139
Violence in the Workplace
Additional risk factors of work-related assaults, include: The availability of drugs or money at hospitals, clinics, and pharmacies, making them likely robbery targets. Situational or circumstantial factors; the increasing presence of gang members, drug or alcohol abusers, trauma patients, or distraught family members, long waits in the ED, all leading to client frustration.

140
Violence in the Workplace
Why is workplace violence prevalent in healthcare? Healthcare workers deal with people on a daily basis who: Are scared – they do not know what is happening or they know that what may happen will be unpleasant Are feeling loss of personal power – they need to show that they are still in control and can act as an individual Are angry – they are angry at the situation which has placed them in the healthcare workers’ care; they are angry that their loved ones are hurting or are ill or dying Are in pain or are sick

141
Violence in the Workplace
Workplace Violence Prevention GSMC is committed to the prevention of all forms of violence in the workplace, and to providing a safe and secure work environment for all employees. Report warning signs of potential violence as soon as possible to a security officer or supervisor.

142
Violence in the Workplace
Workplace Violence Prevention Practice Non-Violent Crisis Intervention Recognize the signs of someone in an agitated state Stay in control of your own behavior Do not handle crisis alone Practice tension reduction and therapeutic rapport

143
Patient Confidentiality, Rules & Regulations
Rev

144
Contact Deb Stewart: Mgr. Privacy Officer (2684) dstewart@gsmc.org
Compliance Hotline:

145
Background: Federal Privacy Protections
Health Insurance Portability and Accountability Act of 1996 (HIPAA) Applies to: Hospitals, physician practices, and other providers Health insurance companies Protects the confidentiality of health information Gives patients certain rights with respect to their health information
 Applies to: Hospitals, physician practices, and other providers. Health insurance companies. Protects the confidentiality of health information. Gives patients certain rights with respect to their health information.")
146
Background: State Privacy Protections
State laws and regulations also protect patient privacy State laws may apply to information about sexually transmitted diseases, HIV, genetic testing, or other conditions Providers must comply with both federal and state laws

147
Background: Protected Health Information (PHI)
HIPAA is designed to protect information that: Identifies individual patients, including demographic information Relates to the past, present, or future physical or mental health of a patient Relates to the past, present, or future payment for a patient’s healthcare services

148
How the HIPAA Privacy Regulations Impact Our Daily Practices
Rev

149
Dr. Jones’ office contacts the hospital to schedule an admission for Mr. Smith. He will be admitted for surgery to repair a fractured ankle. The Hospital Must: Provide a notice of Privacy Practices if this is the patient’s first admission. Make a “good faith” effort to obtain a written acknowledgment from the patient that he has received the Notice of Privacy Practices Tell him that information will be put in the facility directory and allow him an opportunity to object.

150
A few weeks after his discharge, Mr
A few weeks after his discharge, Mr. Smith returns to the hospital and requests a copy of his records. Under HIPAA, patients have the right to access their records in designated record sets and obtain copies of them. This right extends for as long as the hospital keeps the records. Designated record set for providers includes: -Medical Records -Billing Records -Diagnostic images such as X-Rays, EKGs and scans

151
A few weeks after his discharge, Mr
A few weeks after his discharge, Mr. Smith returns to the hospital and requests a copy of his records. May charge a reasonable cost-based fee for making copies and for postage. May not charge a fee for retrieving records for review. Most providers do not charge for copies sent to other providers or given to the patient for continued care.

152
Mr. Smith wants to know to whom the hospital has released information from his records.
Individuals have the right to request an “accounting of disclosures” of PHI for six years prior to the request. Exceptions: Payment, treatment, or operations To the patient or someone authorized by the patient To those involved in the patient’s care For national security or intelligence purposes To correctional institutions and law enforcement Before April 2003

153
Patients have the right to request an amendment:
After reviewing his records, Mr. Smith finds information he believes is incorrect. He asks to have the record amended. Patients have the right to request an amendment: In a designated record set For as long as the hospital maintains the records Most providers require a written request with rationale. Providers have 60 days to act (with a possible 30-day extension). If the request is granted, the hospital must: Notify patient that amendment was accepted Inform relevant persons identified by patient. Amendment requests in our facility must be referred to the privacy officer.
. If the request is granted, the hospital must: Notify patient that amendment was accepted. Inform relevant persons identified by patient. Amendment requests in our facility must be. referred to the privacy officer.")
154
Many deny request if PHI:
After reviewing Mr. Smith’s request, Dr. Goodcare denies the amendment. Many deny request if PHI: Was not created by the hospital (unless the originator is no longer available) Is not part of the designated record set Was not available for inspection Is accurate and complete
 Is not part of the designated record set. Was not available for inspection. Is accurate and complete.")
155
If the request for amendment is denied:
The hospital must give written notice to the patient, explaining: Reason for denial Right to submit written statement of disagreement or have request included with future disclosures Individual’s right to complain to the privacy officer or HHS

156
Mr. Smith’s wife requests a copy of his recors. She says Mr
Mr. Smith’s wife requests a copy of his recors. She says Mr. Smith wants to send it to another doctor who is treating him. The patient’s written authorization is necessary to give his wife a copy The records could be sent to another healthcare provider upon request, because this is covered as part of treatment, payment, and healthcare operations.

157
A few months later, Mr. Smith comes back for a follow-up visit
A few months later, Mr. Smith comes back for a follow-up visit. As he’s leaving, he overhears two staff members discussing his case in the hallway. Visibly upset, he returns to the information desk and says he wants to file a complaint. Patient discussions should never occur in a public area, where they may be overheard by others Patients have the right to file complaints if they believe their privacy has been violated, and we take these complaints very seriously The privacy officer should speak privately with the patient to better understand the situation and express concern

158
Penalties for Violations
We will take corrective action up to and including discharge of an employee Individuals may also be subject to criminal and prison time, for intentional violations

159
Guarding Ethics: False Claims and Corporate Compliance
Rev

160
Contact Ken Cunningham, Executive Vice-President (903)
")
161
Federal and State False Claims Laws
Laws to prevent and detect fraud, waste and abuse in federal and state health programs, such as Medicare and Medicaid. Civil lawsuits may be filed to recover damages and penalties from healthcare providers who submit false claims Any person may file a lawsuit who has knowledge of false claims

162
Federal and State False Claims Laws
Healthcare provider that commits fraud and abuse against Medicare/Medicaid may be fined $ $11,000 for each false claim May be liable for payment up to three times the government’s damages May be liable for payment of costs of civil action against the healthcare provider

163
Federal and State False Claims Laws
Individuals are encouraged to report misconduct under the “whistleblower” provision Individuals may bring a civil lawsuit on behalf of the US Government to recover funds paid by Medicare/Medicaid false claims Government may determine if the lawsuit has merit and may or may not join the lawsuit “Whistleblower” may receive reasonable expenses for attorney’s fees and percentage of amount recovered

164
Federal and False Claims Laws
“Whistleblower” discovered to be involved in false claims, the share of the recovered amount may be reduced “Whistleblower” convicted of criminal conduct related to the submission of the false claim will be dismissed from the lawsuit with no compensation “Whistleblowers” are protected from employer retaliation “Whistleblowers” subjected to retaliation may bring civil lawsuit in federal court and will be entitled to: Reinstatement of job with same seniority Two times the amount of back pay with interest Additional damages such as attorney’s fees

165
Federal and State False Claims Laws
What is Fraud? Fraud is knowingly and willfully executing, or attempting to execute, a scheme to defraud any federal or state health care program or obtain by false means or fraudulent pretenses any money or property owned by or under control of federal or state health care programs.

166
What is Abuse? Abuse may directly or indirectly result in unnecessary costs to Medicare/Medicaid, improper payments, or payments for services which fail to meet professional standards or care or that are medically unnecessary. Abuse involves payment for items or services when there is not legal entitlement payment, although the provider not knowingly or intentionally misrepresented facts to obtain payment.

167
Examples of Health Care Abuse
Collecting more than the coinsurance or deductible allowed by Medicare/Medicaid. Using procedure or revenue codes that describe more extensive services than those provided Requiring a deposit or other payment from a Medicare beneficiary as a condition for admission, continued care, or provision of service Billing for services grossly in excess of those needed or required by the patient (EX: Billing for complete lab profiles when only a single diagnostic test is necessary)
")
168
Reporting Compliance Issues
Good Shepherd asks and encourages anyone to report suspected problems or issues dealing with fraud, waste and abuse in federal and state health care programs. Good Shepherd Compliance policy has detailed information for your use regarding these circumstances available on

169
Reporting Compliance Issues
Call the Compliance Officer: Ken Cunningham Place an anonymous call to the GSHS Compliance Hot Line (24/7) Send a letter to: Compliance Officer, Good Shepherd Health System 700 East Marshall Longview, Texas
 Send a letter to: Compliance Officer, Good Shepherd Health System. 700 East Marshall. Longview, Texas")
170
Reporting Concerns Through Joint Commission
The Joint Commission on Accreditation of Healthcare Organizations (Joint Commission) is an independent, not-for-profit, national body that oversees the safety and quality of healthcare and other services provided in accredited organizations. Employees and the public may report concerns about safety or the quality of healthcare being provided at GSHS to the Joint Commission at Concerns regarding accreditation and the accreditation performance on individual organizations can be obtained through the Joint Commission website at
 is an independent, not-for-profit, national body that oversees the safety and quality of healthcare and other services provided in accredited organizations. Employees and the public may report concerns about safety or the quality of healthcare being provided at GSHS to the Joint Commission at Concerns regarding accreditation and the accreditation performance on individual organizations can be obtained through the Joint Commission website at")
171
Corporate Compliance Rev

172
Corporate Compliance Ensures that Good Shepherd operations are conducted in compliance with its’ policies and procedures in an ethical manner Employees are expected to conduct themselves in accordance with the highest ethical standard and avoid wrong doing

173
Corporate Compliance Compliance is everyone’s job!
Examples of compliance policies are explained in your handbook, such as: Do not discuss cost of services with other hospitals Do not use GSHS tax-exempt status to purchase or for personal benefit Do not take equipment or supplies without authorization

174
Corporate Compliance Hotline: (903)315-5053 Employees should:
Receive a copy of the Compliance Handbook (yellow) upon hire Read, sign and acknowledge compliance with policies Report any compliance issues Hotline: (903)
 upon hire. Read, sign and acknowledge compliance with policies. Report any compliance issues. Hotline: (903)")
175
Corporate Compliance Handbook
Employees should: Complete the 2010 Compliance Handbook CBL and acknowledgement test on GSLS Report any compliance issues Hotline: (903)
")
176
Infection Prevention and Control

177
Contact Terry Smith: Infection Control Nurse (5166)
Cheryl Herbert, Infection Prevention Director (2662)
")
178
Goal of Infection Prevention
Prevent healthcare associated infections (HAI) through education, surveillance, observation and monitoring of infections/communicable diseases. Infection prevention applies to everyone, including patients, visitors, healthcare workers, volunteers, contract employees, physicians and others as needed. Infection prevention extends from inpatient care to outpatient, rehab, skilled care, home care…anywhere a patient receives care.
 through education, surveillance, observation and monitoring of infections/communicable diseases. Infection prevention applies to everyone, including patients, visitors, healthcare workers, volunteers, contract employees, physicians and others as needed. Infection prevention extends from inpatient care to outpatient, rehab, skilled care, home care…anywhere a patient receives care.")
179
Basic Principles of Infection Prevention
Infections cause by bacteria and viruses can be transmitted between patients & healthcare workers. To avoid infection comply with these practices: Hand hygiene – no artificial nails Care & cleaning of equipment Standard precautions and use of PPE Transmission based precautions (isolation) Immunizations Reporting needle sticks or blood/body fluid exposures Prevention is the key!!
 Immunizations. Reporting needle sticks or blood/body fluid exposures. Prevention is the key!!")
180
Basic Principles of Infection Prevention
Infection can be spread in the following ways: Direct contact: spread of infection or germs is person-to-person by direct touch or contact. Indirect contact: Spread of disease or germs is cause by the environment, or by equipment and medical devices that are not cleaned properly or become contaminated by improper handling. Airborne Route: Spread of disease by germs in the air.

181
Standard Precautions Are intended to reinforce well established infection prevention principles such as hand hygiene Reduce the risk of spreading or acquiring bloodborne diseases such as HIV or Hepatitis B Apply to all patients and healthcare workers Food and drink should be in appropriate areas Use barriers to prevent transmission of germs (pathogens) from: Excretions (like stool) -- Blood All body fluids --nonintact skin Secretions (except sweat --mucous membranes (mouth, eyes)
 from: Excretions (like stool) -- Blood. All body fluids --nonintact skin. Secretions (except sweat --mucous membranes (mouth, eyes)")
182
Standard Precautions Gloves
Wear prior to touching blood, body fluids, secretions, excretions, contaminated items, and when performing vascular access procedures (IV catheters) Use clean gloves to touch mucous membranes and non-intact skin Change gloves between tasks and remove promptly after procedures to prevent environmental contamination Always perform hand hygiene before and after glove use
 Use clean gloves to touch mucous membranes and non-intact skin. Change gloves between tasks and remove promptly after procedures to prevent environmental contamination. Always perform hand hygiene before and after glove use.")
183
Standard Precautions Linen: Environmental Control:
Clean and disinfect environmental surfaces, beds, bed rails, bedside equipment, bathrooms and other frequently touched surfaces daily and when soiling occurs Clean all blood spills with an appropriate disinfectant per the Exposure Control Plan Linen: Contain and transport all linen in water-proof bags A second bag is required if outside contamination of the first bag occurs Soiled linen must never be placed on the floor Do not overfill the bag (more than 2/3 full for convenience of handling and proper closure Bags must be securely closed Bagged linen should be placed in specially designated areas for pick up. Environmental services will remove linen per procedure.

184
Standard Precautions Trash
Contain regular trash in a clear plastic bag Use the red biohazard bag or other designated biohazard container for items that are soiled with blood, that cannot be emptied of blood (e.g. chest tube bottles or blood transfusion bags), or that are caked with blood that could flake off. When in doubt, use a red bag A second bag/container is required if outside contamination of the first bag/container occurs Trash is placed in special containers in designated soiled locations Environmental Services will remove trash per procedure.
, or that are caked with blood that could flake off. When in doubt, use a red bag. A second bag/container is required if outside contamination of the first bag/container occurs. Trash is placed in special containers in designated soiled locations. Environmental Services will remove trash per procedure.")
185
Standard Precautions Sharps Laboratory Specimens:
Disposal containers are designated for proper disposal of needles, syringes, and scalpels. Never dispose of sharps in the regular trash Do not bend, recap, resheath, shear, or break used needles or other sharps; activate safety mechanism where applicable Do not overfill sharps container Safety devices (resheathing IVs, safety syringes and scalpels, etc) must be discarded in sharps containers! Safety mechanism must be activated prior to disposal Laboratory Specimens: All specimens are to be considered infectious at all times Transport in a clear plastic bag labeled with the biohazard symbol A second bag/container is required if outside contamination of the first bag/container occurs Secure specimens appropriately for Pneumatic Tube transport
 must be discarded in sharps containers! Safety mechanism must be activated prior to disposal. Laboratory Specimens: All specimens are to be considered infectious at all times. Transport in a clear plastic bag labeled with the biohazard symbol. A second bag/container is required if outside contamination of the first bag/container occurs. Secure specimens appropriately for Pneumatic Tube. transport.")
186
OSHA Standard on Bloodborne Pathogens
Bloodborne diseases like HIV or Hepatitis can be spread when infected fluids enter the body through: Needle stick or sharps injury Cuts, scrapes or other breaks in the skin Splashes of blood or body fluid in the mouth, nose or eyes Oral, vaginal or anal sex Sharing used needles Baby through birth process HIV (Human Immunodeficiency Virus) May start with mild flu-like symptoms and progress; will then weaken the immune system which increases the risk of infections or cancer and may eventually cause death Can lead to AIDS (Acquired Immunodeficiency Syndrome) Can be carried in the blood stream without symptoms – the person doesn’t know that they are infected
 May start with mild flu-like symptoms and progress; will then weaken the immune system which increases the risk of infections or cancer and may eventually cause death. Can lead to AIDS (Acquired Immunodeficiency Syndrome) Can be carried in the blood stream without symptoms – the person doesn’t know that they are infected.")
187
Bloodborne Diseases HBV (Hepatitis B Virus) can cause:
Active Hepatitis B: a flu like illness that can last for many months A chronic carrier state: the person may have no symptoms, but can pass HBV to others Cirrhosis, liver cancer and death Consider the HBV vaccine. It is your best protection against Hepatitis B and is provided free of charge in Employee Health HCV (Hepatitis C Virus): The HCV also attacks the liver and is similar to HBV. There is currently no vaccine available to protect you Patients may not have symptoms of the disease, but can still transmit the infection. The only way to consistently protect yourself is to follow Standard precautions (face protection, gloves, gowns, mouth-to-mouth resuscitation device) every time you expect to have exposure to blood or body fluids A copy of the OSHA Standard on Bloodborne Pathogens is available on request by calling Infection Prevention at x2662
: The HCV also attacks the liver and is similar to HBV. There is currently no vaccine available to protect you. Patients may not have symptoms of the disease, but can still transmit the infection. The only way to consistently protect yourself is to follow Standard precautions (face protection, gloves, gowns, mouth-to-mouth resuscitation device) every time you expect to have exposure to blood or body fluids. A copy of the OSHA Standard on Bloodborne Pathogens is available on request by calling Infection Prevention at x2662.")
188
Transmission-Based Isolation Precautions
Transmission-Based Isolation Precautions are used for patients who have highly contagious diseases/conditions. In addition, these precautions can be used “empirically” based on signs/symptoms of disease before a firm diagnosis is made It is very important to be consistent with hand hygiene, use of gloves, care of the environment, and cleaning of equipment. Germicidal wipes are available for use on surfaces such as keyboards, stethoscopes, and electronic thermometers These additional precautions are necessary to interrupt the chain of transmission.

189
Transmission-Based Isolation Precautions
Airborne Isolation Precautions Used for diseases that are transmitted through the air by tiny particles that can travel long distances on normal air currents. Examples of airborne disease include tuberculosis (TB), rubella (measles), and varicella (chickenpox) Patients who are suspected of or are diagnosed with these diseases are placed in a private, separately ventilated, negative pressure room
, rubella (measles), and varicella (chickenpox) Patients who are suspected of or are diagnosed with these diseases are placed in a private, separately ventilated, negative pressure room.")
190
Transmission-Based Isolation Precautions
Airborne Isolation Precautions (cont’d): The door must be kept closed to maintain negative pressure (air in the room won’t flow out) Anyone entering the room must wear a N-95 respirator as respiratory protection. These are not regular surgical masks, but rather a fit-checked respirator required by CDC – annual fit testing and medical evaluation required If the patient must be transported, place a surgical mask on the patient or provide tissues to cover cough Supplies outside the room would include a posted Airborne Isolation sign, a box of small and regular sized N-95 respirator masks and germicidal wipes to disinfect small pieces of equipment coming out of the room
: The door must be kept closed to maintain negative pressure (air in the room won’t flow out) Anyone entering the room must wear a N-95 respirator as respiratory protection. These are not regular surgical masks, but rather a fit-checked respirator required by CDC – annual fit testing and medical evaluation required. If the patient must be transported, place a surgical mask on the patient or provide tissues to cover cough. Supplies outside the room would include a posted Airborne Isolation sign, a box of small and regular sized N-95 respirator masks and germicidal wipes to disinfect small pieces of equipment coming out of the room.")
191
Transmission-Based Isolation Precautions
Droplet Isolation Precautions: Used for diseases which are transmitted by large respiratory droplets Coughing, talking and suctioning create these droplets. They are so large, they “rain down” (fall out of the air) within 2-3 feet of the patient Examples of droplet spread diseases include the flu, meningitis caused by Neisseria meningitis, pertussis (whooping cough) and streptococcal respiratory disease A private room is necessary A negative pressure room is not indicated Wear an isolation mask(ear loop) when entering the room The patient should wear a surgical mask during transport and cover cough Supplies outside the room would include a posted Droplet Isolation Precaution sign, a box of isolation masks (yellow ear loop masks) and germicidal wipes to be used to disinfect small pieces of equipment coming out of the room
 within 2-3 feet of the patient. Examples of droplet spread diseases include the flu, meningitis caused by Neisseria meningitis, pertussis (whooping cough) and streptococcal respiratory disease. A private room is necessary. A negative pressure room is not indicated. Wear an isolation mask(ear loop) when entering the room. The patient should wear a surgical mask during transport and cover cough. Supplies outside the room would include a posted Droplet Isolation Precaution sign, a box of isolation masks (yellow ear loop. masks) and germicidal wipes to be used to disinfect small. pieces of equipment coming out of the room.")
192
Transmission-Based Isolation Precautions
Contact Isolation Precautions Used for diseases/conditions which are transmitted by physical contact with the patient or the patient’s environment Examples of contact spread diseases or conditions include MRSA, VRE and RSV A private room is necessary Wear gloves when entering the room Wear a gown when entering the room for contact with the patient or environmental surfaces/patient care equipment Remove the gown and gloves before leaving the room and perform hand hygiene Supplies outside the room would include a posted Contact Isolation Precaution sign, a cart to store the gowns, gloves and germicidal wipes to disinfect small pieces of equipment coming out of the room

193
Transmission-Based Isolation Precautions
Contact Special Isolation Precautions Used with patients known or suspected to have Clostridium difficle (C. diff) This organism is spread through contamination of the environment by C. diff spores or by unwashed hands of healthcare workers A private room is necessary Wear gloves when entering the room Wear a gown when entering the room for contact with the patient or environmental surfaces/patient care equipment Remove the gown and gloves before leaving the room and wash your hands with soap and water. Hand sanitizer does not kill C. diff spores
 This organism is spread through contamination of the environment by C. diff spores or by unwashed hands of healthcare workers. A private room is necessary. Wear gloves when entering the room. Wear a gown when entering the room for contact with the patient or environmental surfaces/patient care equipment. Remove the gown and gloves before leaving the room and wash your hands with soap and water. Hand sanitizer does not kill C. diff spores.")
194
Transmission-Based Isolation Precautions
Contact Special Isolation Precautions (cont’d): Environmental Services will clean these rooms with a special cleaning solution to help kill the spores Supplies outside the room would include a posted Contact Special Isolation Precaution sign, a cart to store the gowns, gloves and germicidal wipes to disinfect small pieces of equipment coming out of the room A reminder sign will be posted in the room at the door, to remind you to wash your hands with soap and water before you leave the room
: Environmental Services will clean these rooms with a special cleaning solution to help kill the spores. Supplies outside the room would include a posted Contact Special Isolation Precaution sign, a cart to store the gowns, gloves and germicidal wipes to disinfect small pieces of equipment coming out of the room. A reminder sign will be posted in the room at the door, to remind you to wash your hands with soap and water before you leave the room.")
195
Transmission-Based Isolation Precautions
Multi Drug Resistant Organisms (MDRO): Several common germs or bacteria like Methicillin Resistant Staphylococcus Aureus (MRSA) and Vancomycin Resistant Enterococcus (VRE) have become resistant to many antibiotics. This means the usual antibiotics prescribed will not kill these germs and so they are called Multi-Drug Resistant Organisms (MDRO). While these germs should not cause an illness in healthcare workers, if a patient gets an infection from one of these resistant organisms, the doctor may not be able to cure the infection. MDRO can be spread by direct contact from the hands of a healthcare worker to a patient. Contact Isolation precautions, when used correctly, will prevent the patient-to-patient spread of MDRO.
: Several common germs or bacteria like Methicillin Resistant Staphylococcus Aureus (MRSA) and Vancomycin Resistant Enterococcus (VRE) have become resistant to many antibiotics. This means the usual antibiotics prescribed will not kill these germs and so they are called Multi-Drug Resistant Organisms (MDRO). While these germs should not cause an illness in healthcare workers, if a patient gets an infection from one of these resistant organisms, the doctor may not be able to cure the infection. MDRO can be spread by direct contact from the hands of a healthcare worker to a patient. Contact Isolation precautions, when used correctly, will prevent the patient-to-patient spread of MDRO.")
196
A Healthy Workplace Cover Your Cough
Cover your mouth and nose with a tissue when you cough or sneeze OR Cough or sneeze into your upper sleeve, not your hands Put your used tissue into the trash Clean your hands by washing with soap and water or by using hand sanitizer Get a flu shot every year Protect yourself and our patients! Notify your supervisor prior to beginning work shift of any potentially infectious conditions. Non-intact skin / skin infections GI illness Fever Respiratory illness

197
Influenza: Protect Your Patients. Protect Yourself.
Common Flu Symptoms: Fever (usually high) Headache Tiredness Cough Sore throat Runny or stuffy nose Body aches Influenza Transmission: Flu spreads person to person in respiratory droplets when people who are infected cough or sneeze Healthy adults may be able to infect others 1 day before getting symptoms and up to 5 days after getting sick.
 Headache. Tiredness. Cough. Sore throat. Runny or stuffy nose. Body aches. Influenza Transmission: Flu spreads person to person in respiratory droplets when people who are infected cough or sneeze. Healthy adults may be able to infect others 1 day before getting symptoms and up to 5 days after getting sick.")
198
Influenza: Protect Your Patients. Protect Yourself.
Healthy Tips to Prevent the Flu: Wash your hands Don’t cover sneezes and coughs with your hands Don’t touch your face Clean your ‘shared spaces’ Get enough sleep Drink more water Continue a moderate exercise program Eat healthy Limit alcohol intake Listen to your body

199
Tuberculosis Symptoms:
Tuberculosis (TB) is a serious lung infection caused by a tiny germ called a mycobacterium. When an infected person sneezes, coughs or speaks, the germs are expelled into the air and can be inhaled by another person Symptoms: Severe, prolonged cough (may cough up blood) Fever and night sweats Tiredness Weight loss
 is a serious lung infection caused by a tiny germ called a mycobacterium. When an infected person sneezes, coughs or speaks, the germs are expelled into the air and can be inhaled by another person. Symptoms: Severe, prolonged cough (may cough up blood) Fever and night sweats. Tiredness. Weight loss.")
200
Tuberculosis TB can be easily controlled by following these guidelines: Initiate Airborne isolation Precautions as described earlier under Transmission-Based isolation Precautions Use caution when doing cough inducing procedures, like suctioning or bronchoscopy A portable air treatment machine is available for use in areas without a separately ventilated, negative pressure room. Refer to the Infection Prevention Manual for directions in obtaining the unit, if needed. New employees receive a skin test called a TST (Tuberculin Skin Test). A small amount of fluid (PPD) is injected under the skin on the forearm. A raised, red area on the forearm where the test is placed means the test is positive and you may have been exposed to TB. A thorough physical examination including a chest x-ray would be done to check for infection.
. A small amount of fluid (PPD) is injected under the skin on the forearm. A raised, red area on the forearm where the test is placed means the test is positive and you may have been exposed to TB. A thorough physical examination including a chest x-ray would be done to check for infection.")
201
Infection Prevention and Patient Safety Initiatives
Hand Hygiene Reducing drug resistant organisms Eliminating bloodstream infections caused by central lines (large catheters inserted close to the heart) Eliminating urinary bladder infections caused by catheters Reduce and eliminate infections from surgery
 Eliminating urinary bladder infections caused by catheters. Reduce and eliminate infections from surgery.")
202
Remember: Infection prevention is important for you and particularly for our patients. Everyone is responsible for following the basic principles for hand hygiene, cover your cough, standard precautions and transmission-based isolation precautions. Report any exposure concerns and Infection Prevention will communicate any exposure issues. If you need more information, please refer to the Infection Prevention Manual (available online on GSnet) or contact the Department of Infection Prevention at x2662.
 or contact the Department of Infection Prevention at x2662.")
203
Ready, Set, Go! Rev

Similar presentations











 AGENT SUSCEPTIBLE HOST RESERVOIR.>")







>")
