Download presentation
Presentation is loading. Please wait.

1
Mr. Ash Mukherjee Specialist Registrar Emergency Medicine
Back Pain Mr. Ash Mukherjee Specialist Registrar Emergency Medicine

3
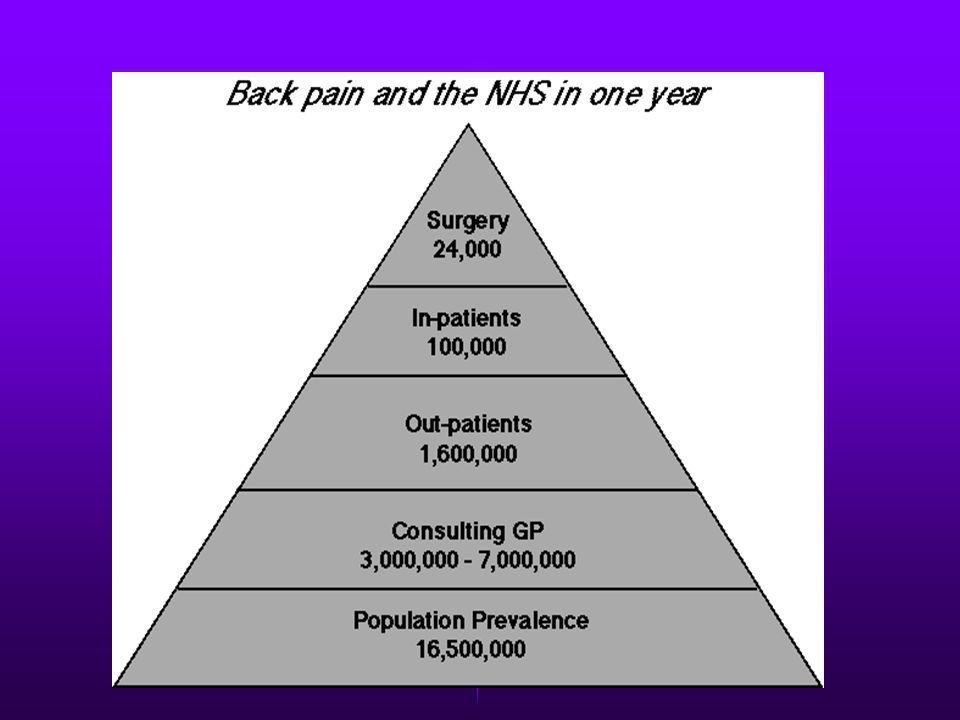
How Big Is the Problem?

5
Costs £481 million a year £197 million £1.4 billion £3.8 billion
£88,000 The estimated cost to the NHS is £481 million a year (min-max range £ million) Non NHS costs (such as private consultations and prescriptions) being an additional £197 million Costs of DSS benefits is estimated at about £1.4 billion Lost production estimated at £3.8 billion Annual NHS cost to a purchasing authority of 250,000 people of £2.2 million (range £1.6 - £2.9 million) A typical GP practice with five GPs and 10,000 patients would bear costs of about £88,000 (range £65,000 - £118,000)
 Non NHS costs (such as private consultations and prescriptions) being an additional £197 million. Costs of DSS benefits is estimated at about £1.4 billion. Lost production estimated at £3.8 billion. Annual NHS cost to a purchasing authority of 250,000 people of £2.2 million (range £1.6 - £2.9 million) A typical GP practice with five GPs and 10,000 patients would bear costs of about £88,000 (range £65,000 - £118,000)")
6
Physical Examination General observation of the patient.
Regional back exam. Neurologic screening. Testing for sciatic nerve root tension. The examination is mostly subjective since patient response or interpretation is required for all parts except reflex testing and circumferential measurements for atrophy.

7
Initial Assessment Potentially serious spinal condition Tumour
Infection Spinal fracture Cauda equina syndrome

8
From physical examination
Possible fracture Possible tumor or infection Possible cauda equina syndrome From medical history Major trauma, such as vehicle accident or fall from height Minor trauma or even strenuous lifting (in older or potentially osteoporotic patient) Age under 20 or over 50. History of cancer. Constitutional symptoms Risk factors for spinal infection Pain that worsens when supine Severe pain at night Saddle anaesthesia. Recent onset of bladder dysfunction, such as urinary retention, increased frequency, or overflow incontinence. Severe or progressive neurological deficit in the Lower extremity From physical examination Unexpected laxity of the anal sphincter. Perianal/perineal sensory loss. Major motor weakness Possible fracture Possible tumor or infection Possible cauda equina syndrome From medical history Major trauma, such as vehicle accident or fall from height. Minor trauma or even strenuous lifting (in older or potentially osteoporotic patient). Age over 50 or under History of cancer. Constitutional symptoms, such as recent fever or chills or unexplained weight loss. Risk factors for spinal infection: recent bacterial infection (e.g., urinary tract infection); IV drug abuse; or immune suppression (from steroids, transplant, or HIV). Pain that worsens when supine; severe nighttime pain. Saddle anesthesia. Recent onset of bladder dysfunction, such as urinary retention, increased frequency, or overflow incontinence. Severe or progressive neurologic deficit in the lower extremity. From physical examination Unexpected laxity of the anal sphincter. Perianal/perineal sensory loss. Major motor weakness: quadriceps (knee extension weakness); ankle plantar flexors, evertors, and dorsiflexors (foot drop).
 Age under 20 or over 50. History of cancer. Constitutional symptoms. Risk factors for spinal infection. Pain that worsens when supine. Severe pain at night. Saddle anaesthesia. Recent onset of bladder dysfunction, such as urinary retention, increased frequency, or overflow incontinence. Severe or progressive neurological deficit in the Lower extremity. From physical examination. Unexpected laxity of the anal sphincter. Perianal/perineal sensory loss. Major motor weakness. Possible fracture. Possible tumor or infection. Possible cauda equina syndrome. From medical history. Major trauma, such as vehicle accident or fall from height. Minor trauma or even strenuous lifting (in older or potentially osteoporotic patient). Age over 50 or under 20. History of cancer. Constitutional symptoms, such as recent fever or chills or unexplained weight loss. Risk factors for spinal infection: recent bacterial infection (e.g., urinary tract infection); IV drug abuse; or immune suppression (from steroids, transplant, or HIV). Pain that worsens when supine; severe nighttime pain. Saddle anesthesia. Recent onset of bladder dysfunction, such as urinary retention, increased frequency, or overflow incontinence. Severe or progressive neurologic deficit in the lower extremity. From physical examination. Unexpected laxity of the anal sphincter. Perianal/perineal sensory loss. Major motor weakness: quadriceps (knee extension weakness); ankle plantar flexors, evertors, and dorsiflexors (foot drop).")
9
Waddel Criteria Tenderness Simulation Distraction Regional
Overreaction Discussion: Waddel determined 5 findings on PE which correlated w/ non organic LBP known as the 5 Waddell criteria; - he noted that most patients w/ documented organic LBP had one or none of Waddell criteria, and that patients who had 3/5 Waddell criteria were much more likely have non organic LBP; cc .70; Five Criteria: - Tenderness superficial (light pinch) non anatomic (tender to palpation over LS, Pelvis, and TS) - Simulation Axial Loading (should not cause LBP) Rotation - Distraction SLR - Regional Weakness Sensory - Overreaction (most important Waddell criteria)
 - non anatomic (tender to palpation over LS, Pelvis, and TS) - Simulation - Axial Loading (should not cause LBP) - Rotation - Distraction - SLR - Regional - Weakness - Sensory - Overreaction (most important Waddell criteria)")
10
Straight Leg Raise/Sciatic Nerve
Myogenic pain Ischial bursitis Annular tear Hamstring tightness Herniated disc Sciatic stretch test Reverse sciatic tension test - Discussion: straight leg raising, by itself, can produce pain from a variety of sources, including myogenic pain, ischial burisitis, annular tear, and hamstring tightness, as well as herniated disc; - the critical distinction is made by the sciatic stretch test; - this test is performed after a straight leg raising test by lowering the affecting leg a few degrees below the point ... popliteal compression:- applying compression to the popliteal fossa helps tethether the sciatic nerve and should help provoke symptoms with a lesser degree of a SLR (removing hamstring irritation as a cause of symptoms); reverse sciatic tension test; - performed by plantar flexing rather than dorsiflexing the foot; - if this results in increased complaints of pain, then pt is malingerer
; reverse sciatic tension test; - performed by plantar flexing rather than dorsiflexing the foot; - if this results in increased complaints of pain, then pt is malingerer.")
11
Hoover Test Test determines whether the patient is malingering when he states that he cannot raise his leg When a patient is genuinely trying to raise his leg, he puts pressure on the calcaneus of his opposite leg to gain leverage

12
Nerve Root Decompression
Sciatica is both severe and disabling. Persists without improvement for longer than 4 weeks or with extreme progression. Strong physiologic evidence of dysfunction of a specific nerve root with intervertebral disc herniation confirmed at the corresponding level and side by findings in an imaging study.

13
Direct and Indirect Nerve Root Decompression for Herniated Discs
Laminotomy Microdiscectomy Laminectomy Chemonucleolysis Percutaneous discectomy Direct and indirect nerve root decompression for herniated discs. Direct methods of nerve root decompression include laminotomy (expansion of the interlaminar space for access to the nerve root and the offending disc fragments), microdiscectomy (laminotomy using a microscope), and laminectomy (total removal of laminae). Methods of indirect nerve root decompression include chemonucleolysis, the injection of chymopapain or other enzymes to dissolve the inner disc. Such chemical treatment methods are less efficacious than standard or microdiscectomy and have rare but serious complications. Any of these methods is preferable to percutaneous discectomy (indirect, mechanical disc removal through a lateral disc puncture).
, microdiscectomy (laminotomy using a microscope), and laminectomy (total removal of laminae). Methods of indirect nerve root decompression include chemonucleolysis, the injection of chymopapain or other enzymes to dissolve the inner disc. Such chemical treatment methods are less efficacious than standard or microdiscectomy and have rare but serious complications. Any of these methods is preferable to percutaneous discectomy (indirect, mechanical disc removal through a lateral disc puncture).")
14
Many patients with strong clinical findings of nerve root dysfunction due to disc herniation recover activity tolerance within 1 month No evidence indicates that delaying surgery for this period worsens outcomes With or without an operation, more than 80 percent of patients with obvious surgical indications eventually recover. Surgery seems to be a luxury for speeding recovery of patients with obvious surgical indications but benefits fewer than 40 percent of patients with questionable physiologic findings. Moreover, surgery increases the chance of future procedures with higher complication rates. Overall, the incidence of first-time disc surgery complications, including infection and bleeding, is less than 1 percent. The figure increases dramatically with older patients or repeated procedures.

15
Bed Rest for Acute Low Back Pain and Sciatica
Bed rest compared to staying active will at best have small effects, and at worst might have small harmful effects on acute LBP Differences in effects of advice to stay in bed compared with advice to stay active are small for patients with low back pain with or without sciatica. There is not an important difference in the effects of bed rest compared with exercises in the treatment of acute low back pain, or seven days compared with two to three days of bed rest in patients with low back pain of different duration with and without radiating pain. Nine trials with a total of 1435 patients were included. Five trials met all four validity criteria and were assessed to have low risk of bias, while four trials were assessed to have moderate to high risk of bias. Four trials compared bed rest with advice to stay active, and overall the results were heterogeneous. Overall results from two high quality studies indicate no difference in pain intensity at three weeks follow-up [Standardized Mean Difference 0.0 (95%CI: -0.3, 0.2)], and a small difference in functional status in favour of staying active [Weighted Mean Difference 3.2 (on a scale) (95%CI 0.6, 5.8)]. Two high quality trials reported no differences in pain intensity between two to three days of bed rest and seven days of bed rest. Another two high-quality trials found no differences between bed rest and exercises in pain intensity or functional status.
], and a small difference in functional status in favour of staying active [Weighted Mean Difference 3.2 (on a scale) (95%CI 0.6, 5.8)]. Two high quality trials reported no differences in pain intensity between two to three days of bed rest and seven days of bed rest. Another two high-quality trials found no differences between bed rest and exercises in pain intensity or functional status.")
16
Injection Therapy for sub acute and Chronic Benign Low Back Pain
Convincing evidence is lacking on the effects of injection therapies for low back pain Only 11 studies compared injection therapy with placebo injections (explanatory trials). The methodologic quality of many studies was low: only 8 studies had a methodologic score of 50 or more points. There were only three well designed explanatory clinical trials: one on injections into the facet joints with a short-term RR of 0.89 (95% CI: ) and a long-term RR of 0.90 (95% CI: ); one on epidural injections with a short-term RR of 0.94 (95% CI: ) and a long-term RR of 1.00 (95% CI: ); and one on local injections with a long-term RR of 0.79 (95% CI: ). Within the 6 subcategories of explanatory studies the pooled RRs with 95% confidence intervals were: facet joint, short-term: RR=0.89 ( ); facet joint, long-term: RR=0.90 ( ); epidural, short-term: RR=0.93 ( ); epidural, long-term: RR=0.92 ( ); local, short-term: RR=0.80 ( ); local, long-term: RR=0.79 ( ).
. The methodologic quality of many studies was low: only 8 studies had a methodologic score of 50 or more points. There were only three well designed explanatory clinical trials: one on injections into the facet joints with a short-term RR of 0.89 (95% CI: ) and a long-term RR of 0.90 (95% CI: ); one on epidural injections with a short-term RR of 0.94 (95% CI: ) and a long-term RR of 1.00 (95% CI: ); and one on local injections with a long-term RR of 0.79 (95% CI: ). Within the 6 subcategories of explanatory studies the pooled RRs with 95% confidence intervals were: facet joint, short-term: RR=0.89 ( ); facet joint, long-term: RR=0.90 ( ); epidural, short-term: RR=0.93 ( ); epidural, long-term: RR=0.92 ( ); local, short-term: RR=0.80 ( ); local, long-term: RR=0.79 ( ).")
17
Lumbar Supports for Prevention and Treatment of Low Back Pain
There is still a need for high quality randomised trials on the effectiveness of lumbar supports Only four of the thirteen studies scored positive on 50% or more of the the internal validity items. There was moderate evidence that for primary prevention lumbar supports are not more effective than other types of treatment or no intervention. No evidence was found on the effectiveness of lumbar supports for secondary prevention : One reviewer extracted data from the trials considering characteristics of the study population, characteristics of the interventions and the final results for each outcome measure. The reviewer compared these findings to data regarding the same characteristics of the same studies published already in other reviews. The methodological quality was independently assessed by two reviewers. Because it was not possible to perform a quantitative analysis, a qualitative meta-analysis was performed in which the strength of evidence on the effectiveness of lumbar supports was classified as being strong, moderate, limited or conflicting, and no evidence. Main results: Five randomized and two nonrandomized controlled preventive trials and six randomized therapeutic trials were included in our review. Overall the methodological quality of the studies included in our review was rather low. Only four of the thirteen studies scored positive on 50% or more of the the internal validity items. There was moderate evidence that for primary prevention lumbar supports are not more effective than other types of treatment or no intervention. No evidence was found on the effectiveness of lumbar supports for secondary prevention. The systematic review of therapeutic trials showed that there is limited evidence that lumbar supports are more effective than no treatment, while it is still unclear if lumbar supports are more effective than other interventions for treatment of low back pain.

18
Acupuncture for Back Pain?
Effects of acupuncture on short-term outcomes in back pain Type of study Number of trials Improved with acupuncture (%) Improved with control (%) Relative benefit (95% CI) NNT (95%CI) Blind 4 73/127 (57) 61/123 (50) 1.2 (0.9 to 1.5) 13 (5 to no benefit) Non-blind 5 78/117 (67) 33/87 (38) 1.8 (1.3 to 2.4) 3.5 (2.4 to 6.5) Fifty-seven percent of patients improved with acupuncture and 50% with control, a relative benefit of 1.2 (95% confidence interval 0.9 to 1.5). The number needed to treat with acupuncture for one patient with back pain to achieve a short-term improvement was 13 (95% confidence interval 5 to no benefit). Five non-blinded studies did show a difference from control, with 67% improved with acupuncture and 38% with control. Here the relative benefit was significant at 1.8 (1.3 to 2.4) and the NNT was 3.5 (2.4 to 6.5). Acupuncture trials are often difficult to assess. There are issues of whether the acupuncture has been done correctly, about the appropriateness of control interventions, whether trials can be truly blinded, and about the relevance of outcomes. Ernst & White have examined these in their review, and make thoughtful comments on all of them. Perhaps the biggest problem is that these trials, as a group, have avoided the hard question of longer-term outcomes. Even if acupuncture provides short-term relief, its place in management of back pain remains unknown. The question is whether this review provides evidence of lack of effect, or lack of evidence of effect. The inability of the four highest quality blinded trials to show a statistically significant short-term improvement must be worrying for those providing acupuncture services, and for the health services or individual who purchase acupuncture. A sceptical view seems to be most appropriate until trials of high quality prove that to be wrong.
 Improved with control (%) Relative benefit (95% CI) NNT (95%CI) Blind /127 (57) 61/123 (50) 1.2 (0.9 to 1.5) 13 (5 to no benefit) Non-blind /117 (67) 33/87 (38) 1.8 (1.3 to 2.4) 3.5 (2.4 to 6.5) Fifty-seven percent of patients improved with acupuncture and 50% with control, a relative benefit of 1.2 (95% confidence interval 0.9 to 1.5). The number needed to treat with acupuncture for one patient with back pain to achieve a short-term improvement was 13 (95% confidence interval 5 to no benefit). Five non-blinded studies did show a difference from control, with 67% improved with acupuncture and 38% with control. Here the relative benefit was significant at 1.8 (1.3 to 2.4) and the NNT was 3.5 (2.4 to 6.5). Acupuncture trials are often difficult to assess. There are issues of whether the acupuncture has been done correctly, about the appropriateness of control interventions, whether trials can be truly blinded, and about the relevance of outcomes. Ernst & White have examined these in their review, and make thoughtful comments on all of them. Perhaps the biggest problem is that these trials, as a group, have avoided the hard question of longer-term outcomes. Even if acupuncture provides short-term relief, its place in management of back pain remains unknown. The question is whether this review provides evidence of lack of effect, or lack of evidence of effect. The inability of the four highest quality blinded trials to show a statistically significant short-term improvement must be worrying for those providing acupuncture services, and for the health services or individual who purchase acupuncture. A sceptical view seems to be most appropriate until trials of high quality prove that to be wrong.")
19
Physiotherapy Exercises for Back Pain
Trials are of insufficient quality to draw a clear conclusion 16 trials included, most were of poor methodological quality Four trials compared exercise therapy with no therapy or placebo therapy Seven trials compared exercise therapy with other conservative treatments Eight trials compared different types of exercise therapy It is not clear whether physiotherapy is better than other conservative treatments, or whether it is better than no treatment. It is not possible to establish which types of exercises are the most effective Of the 16 trials included, most were of poor methodological quality, and trials were generally not adequately designed to assess the intervention - small group sizes, high rates of loss-to-follow-up, internal sensitivity, poor statistical analysis. Type of exercise, control interventions and length of intervention varied between trials. Ten trials had negative conclusions and six had positive conclusions. Reviewers note that there is a general trend for higher quality trials to have positive results. Blinding status was unclear, but ten of sixteen appeared to be evaluator-blind. Inactive/placebo comparisons Four trials compared exercise therapy with no therapy or placebo therapy. One of four trials showed a benefit of exercise therapy for pain and activity at four and 12 weeks, but this did not persist to three months. The remaining trials showed no benefit for acute pain, sciatic symptoms and chronic low back pain. Active comparisons Seven trials compared exercise therapy with other conservative treatments. Two of seven trials showed significant benefit compared with hot packs and rest and with mini back school (i.e. one session). The second study showed benefit was still present at one year. Five of seven trials showed no benefit when compared with manual therapy, home care instructions, non-steroidal anti-inflammatory drugs, manipulation, manipulation and mobilisation or short wave diathermy. Different exercise therapies compared Eight trials compared different types of exercise therapy - mainly isometric flexion exercises compared with extension exercises. Four of eight trials showed no difference (although all were flawed). Four showed some benefit - one favouring three months of intensive dynamic back extensor exercises over a less intensive treatment plus massage and heat, one favoured extension over flexion exercises, and two favoured flexion exercises over mobilisation plus other exercises and, in one trial, massage and heat. Adverse effects Reviewers did not report on adverse effects
. The second study showed benefit was still present at one year. Five of seven trials showed no benefit when compared with manual therapy, home care instructions, non-steroidal anti-inflammatory drugs, manipulation, manipulation and mobilisation or short wave diathermy. Different exercise therapies compared. Eight trials compared different types of exercise therapy - mainly isometric flexion exercises compared with extension exercises. Four of eight trials showed no difference (although all were flawed). Four showed some benefit - one favouring three months of intensive dynamic back extensor exercises over a less intensive treatment plus massage and heat, one favoured extension over flexion exercises, and two favoured flexion exercises over mobilisation plus other exercises and, in one trial, massage and heat. Adverse effects. Reviewers did not report on adverse effects.")
22
AND REMEMBER

23
Simple Backache Specialist Referral Not Required
Presentation years Lumbosacral, buttocks and thighs "Mechanical" pain Patient well

24
Nerve Root Pain Specialist Referral Not Generally Required Within First 4 Weeks, Provided Resolving
Unilateral leg pain worse than low back pain Radiates to foot or toes Numbness & paraesthesia in same direction SLR reproduces leg pain Localised neurological signs

25
Red flags for possible serious spinal pathology consider prompt referral
Presentation under age 20 or over 55 Non-mechanical pain Thoracic pain Past history - carcinoma, steroids, HIV Unwell, weight loss Widespread neurological symptoms or signs Structural deformity

26
Cauda Equina Syndrome Immediate Referral
Sphincter disturbance Gait disturbance Saddle anaesthesia

Similar presentations








 Symposium 13 th May 2004 Carol Coole Occupational Therapist NOTTINGHAM BACK TEAM.>")




 Case 3: Karen.>")
 - Lumbar>")







