Download presentation
Presentation is loading. Please wait.

1
Antiepleptic, neuropathic, antihypertensive medications
Tom McPharlin R.Ph. Harborview Medical Center June 2012 Introduce myself

2
Causative factors Structural damage to brain
Trauma Stroke: ischemia, hemorrhage Anoxia Toxins Tumors Metabolic disorders Prolonged seizures Infection Idiopathic – genetics (Channelopathy) Cryptogenic – no identifiable reason Ex. Of cryptogenic would be lennox-gastaut syndrome
 Cryptogenic – no identifiable reason. Ex. Of cryptogenic would be lennox-gastaut syndrome.")
3
Drugs that decrease seizure threshold
Penicillin’s (HD) Quinolones (HD) Disulfiram Dantrolene Antipsychotics chlorpromazine clozapine (titrate!) perphenazine Tramadol (renal fx!) Buproprion (OD) Anticonvulsants (OD) Clomipramine Ethanol withdrawal Benzo withdrawal Illicit street drugs Amphetamines Cocaine Ecstasy **all drug that affect the CNS have the potential of causing a sz. Obviously drugs taken in toxic doses also vary and cannot be completely listed.
 Quinolones (HD) Disulfiram. Dantrolene. Antipsychotics. chlorpromazine. clozapine (titrate!) perphenazine. Tramadol (renal fx!) Buproprion (OD) Anticonvulsants (OD) Clomipramine. Ethanol withdrawal. Benzo withdrawal. Illicit street drugs. Amphetamines. Cocaine. Ecstasy. **all drug that affect the CNS have the potential of causing a sz. Obviously drugs taken in toxic doses also vary and cannot be completely listed.")
4
Drugs that decrease seizure threshold

5
Drugs that decrease sz threshold

6
Drugs that decrease sz threshold

7
Treatments for epilepsy
Medication (AEDs) Surgery Electrical stimulation Ketogenic diet
 Surgery. Electrical stimulation. Ketogenic diet.")
8
AED treatment Select proper AED for type of epilepsy
Pharmacokinetic profile Drug/Disease state interaction Expected adverse effects Patient preference Use one agent until therapeutic effect OR toxicity If inadequate control with first medication then add second drug slowly to therapeutic dose then start SLOWLY decreasing the first agent

9
AEDs Broad Spectrum Agents Narrow Spectrum Agents Felbamate
Lamotrigine Levetiracetam Rufinamide Topiramate Valproate Zonisamide Carbamazepine Gabapentin Lacosamide Oxcarbazepine Phenytoin Pregabalin Tiagabine Ethosuximide (absence)
")
10
Pharmacology of AEDs GABA : Glutamate (NMDA, Kinate, AMPA) :
major inhibitory neurotransmitter underexcited Glutamate (NMDA, Kinate, AMPA) : major excitatory neurotransmitter overexcited Sodium, Calcium, Potassium ? Channel Serotonin system? Complex and multifactorial…but if you know these basic principles it will help in the understanding of how the drugs work. fine balance in the brain between factors that begin electrical activity and factors that restrict it, and there are also systems that limit the spread of electrical activity Tx: benzo bind to GABA receptor and increase GABA transmission Barbituates bind directly to GABA receptor
 : major excitatory neurotransmitter. overexcited. Sodium, Calcium, Potassium Channel. Serotonin system Complex and multifactorial…but if you know these basic principles it will help in the understanding of how the drugs work. fine balance in the brain between factors that begin electrical activity and factors that restrict it, and there are also systems that limit the spread of electrical activity. Tx: benzo bind to GABA receptor and increase GABA transmission. Barbituates bind directly to GABA receptor.")
11
Mechanism of action of AEDs

12
Status Epilepticus (SE)
Old definition: continuous seizure lasting > 30 min Newer definition: continuous, generalized, convulsive seizure lasting longer than 5 min (Lowenstein, 1999) Refractory SE: sz lasting > 2 hours OR doesn’t respond to first-line treatment (two drugs) Mortality: 8-32% Has been defined as a continuous seizure lasting 30 minutes or as two or more discrete seizures between which consciousness is not fully regained Newer thought has proposed that SE be defined as a continuous, generalized, convulsive seizure lasting longer than 5 min, or two or more seizures during which patient does not return to baseline consciousness. (Lowenstein, 1999) new def based on rationale that typical, generalized tonic-clonic sz rarely lasts > 5min, spontaneous termination becomes less likely in sz of >5 in, and that longer the seizure continues the more difficult the sz becomes to control and greater degree of neuronal damage - unreasonable to wait 30 minutes to start treat SE…. Metabolic demands of brain increase 3-5 fold when exhausted causes brain damage -sz recurrence is a significant risk -
 Refractory SE: sz lasting > 2 hours OR doesn’t respond to first-line treatment (two drugs) Mortality: 8-32% Has been defined as a continuous seizure lasting 30 minutes or as two or more discrete seizures between which consciousness is not fully regained. Newer thought has proposed that SE be defined as a continuous, generalized, convulsive seizure lasting longer than 5 min, or two or more seizures during which patient does not return to baseline consciousness. (Lowenstein, 1999) new def based on rationale that typical, generalized tonic-clonic sz rarely lasts > 5min, spontaneous termination becomes less likely in sz of >5 in, and that longer the seizure continues the more difficult the sz becomes to control and greater degree of neuronal damage. - unreasonable to wait 30 minutes to start treat SE…. Metabolic demands of brain increase 3-5 fold when exhausted causes brain damage. -sz recurrence is a significant risk. -")
13
Progression of SE Neuronal injury
1st phase – generalized tonic-clonic seizures Increase in autonomic activation Increase in cerebral blood flow 2nd phase – failure of cerebral autoregulation Decrease in cerebral blood flow Clinical manifestations restricted twitching Longer sz untreated, greater neurologic damage, more difficult to treat. Neuronal injuray 1st phase – generalized tonic-clonic sz Increase in autonomic activation – ie. Hypertension, hyperglycemia, sweating, salvation Increase in cerebral blood flow which incr the metabolic demands of the brain 2nd phase – 30 min later failure of cerebral autoreg Decrease in cerebral blood flow – which causes an increase in ICP and systemic decrease in BP Sz at this point cont but clinical manifestations are restricted to minor twitching (looks like a coma) Ends in brain death
 Ends in brain death.")
14
Complications Cardiac dysrhythmias Pulmonary edema Hyperthermia
Rhabdomyolysis Aspiration Pneumonia

15
Treatment of SE VA cooperative trial 1998 Refractory
SF Emergency Medical Service 2001 Recommend lorazepam as 1st-line Refractory Evidence more limited Drug of Choice (DOC): pentobarbital, midazolam and propofol continuous infusion Alternative drugs: Valproate , Levetiracetam , lacosamide IV infusions Mention potential of IV valproic acid and case studies and potential use of topamax Tx successful if clinical and electrical evidenc of sz activity stopped within 20 min after starte of tx and id not recur during the period fomr 20-60min.
: pentobarbital, midazolam and propofol continuous infusion. Alternative drugs: Valproate , Levetiracetam , lacosamide IV infusions. Mention potential of IV valproic acid and case studies and potential use of topamax. Tx successful if clinical and electrical evidenc of sz activity stopped within 20 min after starte of tx and id not recur during the period fomr 20-60min.")
16
Diazepam vs Lorazepam Drug Dose Onset Duration Points to remember
mg\kg 1 – 3 min. 15-30 min Redistributes out of CNS. Lipid soluble Lorazepam 0.1mg\kg 3-10 min. 12-24 hours Needs to be refrigerated. Water soluble, less likely to leave CNS. Diazepam: Rapid onset Can be given rectally Dis: short duration of action, depresses cons, active metabolite Lorazepam: Also has rapid onset of action but a longer duration than diazepam Dis: needs to be refrigerated therefore often not in Medic trucks

17
Treatment algorithm 1st: Lorazepam 0.1 mg/kg
2nd: Phenytoin (fosphenytoin) 20mg/kg IV (monitor BP) Sz not controlled then: (+/- additional 5mg/kg Phenytoin?) Valproate 20-45mg/kg IV load or Levetiracetam mg IV x1 Lacosamide?? mg IV x1 - Intubation after this point – Midazolam bolus 0.2mg/kg: 0.1mg/kg/hr continuous drip Propofol Bolus 1-2mg: 2mg/kg/hr continuous drip (MAX 48 HR) Pentobarbital Bolus 5-15mg/kg: 1mg/kg/hr continuous drip 2 Hirsch, et al. Treatment of SE 2002/NCC guidelines
 20mg/kg IV (monitor BP) Sz not controlled then: (+/- additional 5mg/kg Phenytoin ) Valproate 20-45mg/kg IV load. or. Levetiracetam mg IV x1. Lacosamide mg IV x1. - Intubation after this point – Midazolam bolus 0.2mg/kg: 0.1mg/kg/hr continuous drip. Propofol Bolus 1-2mg: 2mg/kg/hr continuous drip (MAX 48 HR) Pentobarbital Bolus 5-15mg/kg: 1mg/kg/hr continuous drip. 2. Hirsch, et al. Treatment of SE 2002/NCC guidelines.")
18
SE and treatment

19
RSE treatment

20
FDA Indications for AEDs for seizure type
Partial (2nd generalized) Primary generalized PHENYTOIN X NO CARBAMAZEPINE OXCARBAZEPINE TIAGABINE GABAPENTIN PREGABALIN VALPROATE LAMOTRIGINE TOPIRAMATE ZONISAMIDE LEVETIRACETAM
 Primary generalized. PHENYTOIN. X. NO. CARBAMAZEPINE. OXCARBAZEPINE. TIAGABINE. GABAPENTIN. PREGABALIN. VALPROATE. LAMOTRIGINE. TOPIRAMATE. ZONISAMIDE. LEVETIRACETAM.")
21
Efficacy of newer AEDs Clincal comparability of new AEDs in refractory partial epilepsy:A systematic review and meta-analysis Epelpsia 2011

22
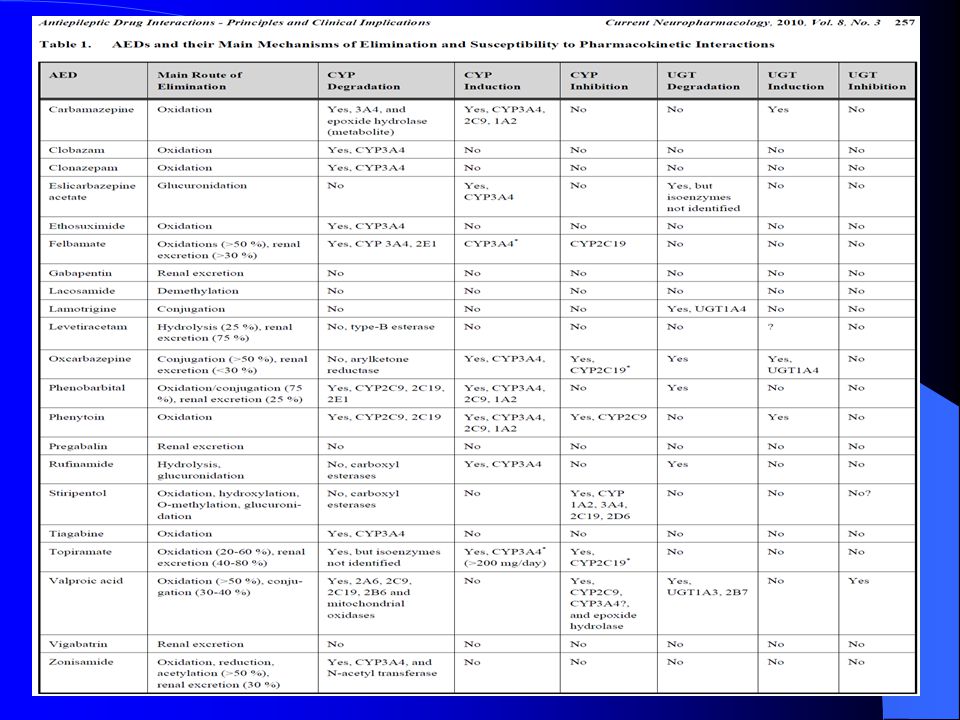
Drug Interactions Inducers (2-3 weeks for max effect):
Carbamazepine Phenytoin Phenobarbital Primidone (phenobarbital) Oxcarbazepine, topiramate (>200mg/day), Rufinamide (3A4) Inhibitors (mostly immediate): Valproate Felbamate Stiripentol Rufinamide?
 Oxcarbazepine, topiramate (>200mg/day), Rufinamide (3A4) Inhibitors (mostly immediate): Valproate. Felbamate. Stiripentol. Rufinamide")
24
Drug Interactions Protein Binding:
Phenytoin, Valproate, Carbamazepine, Tiagabine, Oxcarbazepine Drug transporters (Pgp, MRP2, MRP3): Induced by the AED inducers Increased secretion of agent (renal,gut,brain) Important interactions: Valproate with Lamotrigine (increase t1/2) Valproate and carbapenems (decrease vpa lvls)
: Induced by the AED inducers. Increased secretion of agent (renal,gut,brain) Important interactions: Valproate with Lamotrigine (increase t1/2) Valproate and carbapenems (decrease vpa lvls)")
25
Drug Interactions - OCPs
OCPs and Inducer AEDs Estrogen decreased by Inducers No effect: gabapentin, levetiracetam, zonisamide, lamotrigine, topiramate (dose <200mg/day) No effect on estrogen eluting IUDs High dose OCPs recommended (Ovral) OCPs effects on AED: Lamotrigine levels decreased by 50% with OCPs Estrogen component Rebound effect on the 7 days off OCPs = toxicity? Valproate levels (free and total) increased
 No effect on estrogen eluting IUDs. High dose OCPs recommended (Ovral) OCPs effects on AED: Lamotrigine levels decreased by 50% with OCPs. Estrogen component. Rebound effect on the 7 days off OCPs = toxicity Valproate levels (free and total) increased.")
26
Drug Interactions: Enzyme inducer AEDs

27
AED blood levels Used as a guide Useful when:
Assessing compliance Drug interactions Phenytoin dosing?! (FREE level) Therapeutic/Toxic levels defined by patient
 Therapeutic/Toxic levels defined by patient.")
28
Most significant AED adverse effects
Phenytoin Sedation, hersutism, gum hyperplasia, drug interaction (DI), rash Carbamazepine Sedation, rash, DI, hyponatremia Tiagabine Dizziness Gabapentin Sedation, Weight gain Valproate Weight gain, teratogenesis Lamotrigine Rash Topiramate Cognitive slowing, weight loss, mood Zonisamide Cognitive slowing, weight loss Levetiracetam Mood change Pregabalin Weight gain, sedation Oxcarbazepine hyponatremia
, rash. Carbamazepine. Sedation, rash, DI, hyponatremia. Tiagabine. Dizziness. Gabapentin. Sedation, Weight gain. Valproate. Weight gain, teratogenesis. Lamotrigine. Rash. Topiramate. Cognitive slowing, weight loss, mood. Zonisamide. Cognitive slowing, weight loss. Levetiracetam. Mood change. Pregabalin. Weight gain, sedation. Oxcarbazepine. hyponatremia.")
29
AEDs and teratogenicity

30
HLA-B 1502 Majority of Asians with SJS/TEN had allele Frequency:
No association with Macro Papular Eruptions Frequency: 10-15% in China, Thailand, Malaysia, Indonesia, Philippines and Taiwan 2-4% in India <1% in Japan and Korea Asians should be screened prior to starting CBZ, Phenytoin and ?? Lamotrigine

31
HLA-A 3101 allele Japanese European descent Associated with SJS-TEN
High rate of hypersensitivity rxn including SJS-TEN

32
Specific AEDS in Depth

33
Phenytoin (Dilantin) Absorption: 100% ; nonlinear
Exception: tube feedings = 50% decrease absorption Distribution: highly protein bound (weakly) Metabolism: Hepatic Clearance: nonlinear kinetics (Michaelis-Menton); CYP2C9 (major); half-life hours; consider special population (elderly, nutritional). Lots of Drug Interactions!!! (Inducer) Can worsen absence and Juvenile Myoclonic seizures Gold standard in sz prophylaxis and treatment. …. Small change in dose or F can result in disproportionate change in steady-state Fosphenytoin (Cerebyx) – prodrug of Phenytoin unlike phenytoin higly soluble and stable in all IV solutions due to presence of a phosphate group lower need for reduction infusion rates, can be infused rapidly over minutes 150mg\min advantage: can be given IM but it still should be given IV for SE disadvantage, must be converted by liver to gain pharmacological activity Absorption: F~ 1 ; nonlinear; tube feedings Distribution: highly protein bound (consider following people renal failure, pregnancy, liver dx, alcoholics, ICU, elderly) Clearance: nonlinear kinetics (Michaelis-Menton); CYP2C9 (major); half-life hours; consider special pop. (hepatic failure, elderly(low metabolism need smaller dose/kg), children (high met: larger dose/kg)
 Metabolism: Hepatic. Clearance: nonlinear kinetics (Michaelis-Menton); CYP2C9 (major); half-life hours; consider special population (elderly, nutritional). Lots of Drug Interactions!!! (Inducer) Can worsen absence and Juvenile Myoclonic seizures. Gold standard in sz prophylaxis and treatment. …. Small change in dose or F can result in disproportionate change in steady-state. Fosphenytoin (Cerebyx) – prodrug of Phenytoin. unlike phenytoin higly soluble and stable in all IV solutions due to presence of a phosphate group. lower need for reduction infusion rates, can be infused rapidly over minutes 150mg\min. advantage: can be given IM but it still should be given IV for SE. disadvantage, must be converted by liver to gain pharmacological activity. Absorption: F~ 1 ; nonlinear; tube feedings. Distribution: highly protein bound (consider following people renal failure, pregnancy, liver dx, alcoholics, ICU, elderly) Clearance: nonlinear kinetics (Michaelis-Menton); CYP2C9 (major); half-life hours; consider special pop. (hepatic failure, elderly(low metabolism need smaller dose/kg), children (high met: larger dose/kg)")
34
Phenytoin Dosing Loading dose: 18-20mg/kg
If given orally: saturable absorption mg Dilute in 0.9% NaCl (will ppt in dextrose) Max rate 50mg/min (hypotension rate-dep.) Lower rate if elderly or multiple CV complications 25mg/min Maintenance: usually 300 – 400mg/day (5mg/kg/day) Therapeutic Index: 10-20mcg/mL free (1-2mcg/mL) Given q HS (max oral mg) infusion rate limited by cardiotoxic side effects (main advantage of fosphenytoin) max 50mg\min Some disadvantages: poorly soluble in water. Dissolved in propylene glycol and sodium hydroxide (lye). These are responsible fro pain during infusion, phlebitis, and skin sloughing after extravsation, and hypotension originally formulated to be an IM preparation rather than IV, however when given IM extremely painful and poorly absorbed (don’t give IM)
 Max rate 50mg/min (hypotension rate-dep.) Lower rate if elderly or multiple CV complications 25mg/min. Maintenance: usually 300 – 400mg/day (5mg/kg/day) Therapeutic Index: 10-20mcg/mL. free (1-2mcg/mL) Given q HS (max oral mg) infusion rate limited by cardiotoxic side effects (main advantage of fosphenytoin) max 50mg\min. Some disadvantages: poorly soluble in water. Dissolved in propylene glycol and sodium hydroxide (lye). These are responsible fro pain during infusion, phlebitis, and skin sloughing after extravsation, and hypotension. originally formulated to be an IM preparation rather than IV, however when given IM extremely painful and poorly absorbed (don’t give IM)")
35
Phenytoin Toxicity Plasma level related Non-dose related Nystagmus
(> 20mcg\mL) Ataxia (>30 mcg\mL) Confusion (> 40mcg\mL) Encephalopathy Seizure Hypotension (rate) Non-dose related GI toxicity Rash Gingival hyperplasia Hirsutism Folate deficiency and megaloblastic anemia Osteoporosis Hepatotoxicity Teratogenesis Plasma level related Nystagmus (> 20mcg\mL) – rapid involuntary movement of eyes Ataxia (>30 mcg\mL) – shaky movements and unsteady gait Confusion (> 40mcg\mL) Encephalopathy Non-dose related GI toxicity (give with food) Rash (Cross sensitivity with other agents???) Gingival hyperplasia Hirsutism Folate deficiency and megaloblastic anemia Osteoporosis – give with Ca/Vit D Hepatotoxicity – ass with rash and fever and lymphadenopathy Teratogenesis – fetal hydantoin syndrome cleft palate and enlarged facial bones
 Ataxia (>30 mcg\mL) Confusion (> 40mcg\mL) Encephalopathy. Seizure. Hypotension (rate) Non-dose related. GI toxicity. Rash. Gingival hyperplasia. Hirsutism. Folate deficiency and megaloblastic anemia. Osteoporosis. Hepatotoxicity. Teratogenesis. Plasma level related. Nystagmus (> 20mcg\mL) – rapid involuntary movement of eyes. Ataxia (>30 mcg\mL) – shaky movements and unsteady gait. Confusion (> 40mcg\mL) Encephalopathy. Non-dose related. GI toxicity (give with food) Rash (Cross sensitivity with other agents ) Gingival hyperplasia. Hirsutism. Folate deficiency and megaloblastic anemia. Osteoporosis – give with Ca/Vit D. Hepatotoxicity – ass with rash and fever and lymphadenopathy. Teratogenesis – fetal hydantoin syndrome cleft palate and enlarged facial bones.")
36
Tube Feedings Decreases Phenytoin (PTN) bioavailability
Binding to enteral feeding – ca, casinates Binding to actual tubing 50% decrease in bioavailability Pharmacotherapy 1998;18(3): and/or Neurology 1978: ….
: and/or Neurology 1978: ….")
37
Fosphenytoin (Cerebyx)
Prodrug (inactive) of phenytoin Advantages: Soluble and stable in all IV solutions Faster rate of infusion 150mg/min Can be given IM (still use IV for SE) Disadvantage Must be converted by liver to gain activity Units are expressed in PE (phenytoin equivalents)
 of phenytoin. Advantages: Soluble and stable in all IV solutions. Faster rate of infusion 150mg/min. Can be given IM (still use IV for SE) Disadvantage. Must be converted by liver to gain activity. Units are expressed in PE (phenytoin equivalents)")
38
Carbamazepine (CBZ) Absorption: 75%
Metabolism: hepatic – CYP3A4, 1A2,2C8 Epoxide – active metabolite Auto inducer: takes 4-6 weeks Dosing: 200mg BID; inc. q3-5days TI: 4-12 mcg/mL not useful for epoxide metabolite –NOT reflected Indications: GTC and partial sz disorders, trigeminal neuralgia, bipolar dx Prominent features: poor conc-dose relationship, active metabolite, and autoinducer Absorption: has low water solubility so absorption is low. Dissolution-rate dependent; food enhances F and suspension is abs faster than tablets

39
CBZ Toxicity Diplopia Drowsiness Dizziness Blurred vision
Poor mental performance Nystagmus Ataxia Anticholinergic SE Antidiuretic hormone like activity Altered lipids Thrombocytopenia Hepatitis Rashes Osteoporosis Diplopia Drowsiness Dizziness Blurred vision Poor mental performance Nystagmus Ataxia Hyponatremia defined as sNa of <135. Potential mechanism is that it increases sensitivityo osmorecptors to ADH or have direct effect on receptors. Closely linked to age. Incidence increases with age. See it develop in first 90 days.

40
Phenobarbital Indicated for generalized onset myoclonic & partial/gen. onset tonic-clonic Not used commonly as sz prophylaxis or maintenance Studies have shown longer ICU\hospital stays Used more in practice in EtOH withdrawal and SE Load dose: 18mg/kg Maintenance: 120 – 180mg QD Half-Life: Approximately 3 days Water soluble and inexpensive Downside isCNS depression leading to respiratory compromise Side effects: rash/steven-johnson, blood dyscraias, angioedema Lot of Drug interactions

41
Valproic Acid (VA) Absorption: 100% Distribution: highly protein bound
Metabolism: Hepatic Clearance: hepatic glucuronidation/beta-oxidation, CYP450 (minor) Drug interactions: inhibitor and protein binding displacer Broad spectum anticonvulsant. Best for myoclonic jerking, absence. Also been used for migraines and psych illness such as bipolar. Also indicated for generalized myoclonic, partial/generalized onset Free level monitoring has been recommended since free is the active form however conc-effect relationship have shown to be variable fpr both free and total levels Many formulations Depacon – IV formulation Depakote – oral preparation
 Drug interactions: inhibitor and protein binding displacer. Broad spectum anticonvulsant. Best for myoclonic jerking, absence. Also been used for migraines and psych illness such as bipolar. Also indicated for generalized myoclonic, partial/generalized onset. Free level monitoring has been recommended since free is the active form however conc-effect relationship have shown to be variable fpr both free and total levels. Many formulations. Depacon – IV formulation. Depakote – oral preparation.")
42
VA Dosing Loading: 18-45mg/kg Maintenance: 500mg PO BID to TID
Pft/iv dose q8 h to q6 h TI: mcg/mL (free is active form but not measured) Available as: Divalproex sodium po (Depakote) 250, 500mg Valproic acid syrup pft (tid to qid) Valproic acid IV formulation (tid to qid) Start low to avoid GI Side effects and drowsiness. Increase 25-30% every 7 days until targe dose reached
 Available as: Divalproex sodium po (Depakote) 250, 500mg. Valproic acid syrup pft (tid to qid) Valproic acid IV formulation (tid to qid) Start low to avoid GI Side effects and drowsiness. Increase 25-30% every 7 days until targe dose reached.")
43
VA Toxicity GI effects Drowsiness/confusion Tremor Weight gain
Hyperammonemia (without LFT changes) Inhibition of platelets and lowering of count Hepatotoxic Pancreatitis Teratogenic GI effects – take with food Drowsiness/confusion Tremor Weight gain Hyperammoniemia – explain mechanism and antidote L-carnitine Inhibition of platelets and lowering of count Hepatoxic – Pancreatitis Teratogenic - spinal bifida
 Inhibition of platelets and lowering of count. Hepatotoxic. Pancreatitis. Teratogenic. GI effects – take with food. Drowsiness/confusion. Tremor. Weight gain. Hyperammoniemia – explain mechanism and antidote L-carnitine. Inhibition of platelets and lowering of count. Hepatoxic – Pancreatitis. Teratogenic. - spinal bifida.")
44
Ethosuximide (Zarontin)
Generalized absence Dose: 500 – 1500mg PO Qday TI: mcg/mL Absorption = 100 % Metabolized by liver (CYP450) Half-life hours
 Half-life hours.")
45
Ethosuximide Toxicity
GI: nausea/vomiting Headaches Psychotic episodes Rash EPS – parkinsonism, bradykinesia

46
Newer AED’s Gabapentin (1993) Lamotrigine (1994) Topiramate (1996)
Tiagabine (1997) Levetiracetam (1999) Oxcarbazepine (1999) Zonisamide (2000) Pregabalin (2001) Lacosamide (2009) Older agents can cause a lot of SE and also: narrow Therapeutic window Pharmacokinetic and pharmacetuical prop making administration difficult and complex Drug interactions Cross-reactivity between agents All these have lead to finding newer agents Problem with these agents. Research is poor in head to head trials with older agents. No IV formulations available. Gabapentin – not going to talk a whole lot about since we generally don’t use it on our service. Division between coasts opinion.
 Levetiracetam (1999) Oxcarbazepine (1999) Zonisamide (2000) Pregabalin (2001) Lacosamide (2009) Older agents can cause a lot of SE and also: narrow Therapeutic window. Pharmacokinetic and pharmacetuical prop making administration difficult and complex. Drug interactions. Cross-reactivity between agents. All these have lead to finding newer agents. Problem with these agents. Research is poor in head to head trials with older agents. No IV formulations available. Gabapentin – not going to talk a whole lot about since we generally don’t use it on our service. Division between coasts opinion.")
47
Lamotrigine (Lamictal)
Partial seizures and primary generalized Start low 25mg PO QDay and titrate slowly to 150mg PO Q Day (approximate max 400 mg) Different with inducer (50mg) or inhibitor (25 mg qod) on board Haven’t established definitive blood levels Toxicity Skin rash: erythematous, morbilliform rash occurring within 4-6 weeks. Enhanced by VPA; starting at higher doses and\or rapid dose escalation may increase toxicity Indicated for partial sz but also being used in other psych disorders, migraine, and pain Down side is that it can take weeks for beneficial effects to occur
 Different with inducer (50mg) or inhibitor (25 mg qod) on board. Haven’t established definitive blood levels. Toxicity. Skin rash: erythematous, morbilliform rash occurring within 4-6 weeks. Enhanced by VPA; starting at higher doses and\or rapid dose escalation may increase toxicity. Indicated for partial sz but also being used in other psych disorders, migraine, and pain. Down side is that it can take weeks for beneficial effects to occur.")
48
Topiramate (Topamax) Adjunctive for partial seizures and primary generalized Start at 25mg PO BID, increase weekly by 25-50mg to 200mg PO BID or more RSE: MUCH faster and higher! Drug levels do not correspond to efficacy Renally eliminated Also starting to be used as monotherapy for sz and in psych (bipolar), peripheral neuropathies, essential tremor and migraines.
, peripheral neuropathies, essential tremor and migraines.")
49
Topiramte Toxicity GI: diarrhea and weight loss
CNS: mental slowing, fatigue Psychosis Acidosis Kidney stone formation

50
Levetiracetam (Keppra)
Adjunctive for partial seizures and primary generalized Case reports in SE – IV formulation Start dose at 500mg PO BID, inc. q2wk to 1500mg PO BID (possibly more) Drug levels do not correspond to efficacy Few DI – not metabolized by CYP or UGT Renally cleared – Dose adjust r/t GFR!! SE: Drowsiness, dizziness, agitation IV formulation – add on therapy or transitional mediation
 Drug levels do not correspond to efficacy. Few DI – not metabolized by CYP or UGT. Renally cleared – Dose adjust r/t GFR!! SE: Drowsiness, dizziness, agitation. IV formulation – add on therapy or transitional mediation.")
51
Oxcarbazepine (Trileptal)
Similar to CBZ Used successfully as monotherapy for partial and sec generalized tonic/clonic seizures. NOT primary generalized. Dose: mg PO BID ADR: similar to CBZ, increased hyponatremia – cross sensitivity rxn occurs in 25% of pts who had rash from CBZ Does not work on absence or myoclonic sz hyponatremia more common with OXC vs CBZ Leudopenia is less common with OX Unlike CBZ there is no autoinduction Seems to be equally effective with CBZ in tx of partial and sec generalized sz with fewer SE and fewer DI Best if used in tx of localization related epilepsy

52
Zonisamide (Zonegran)
Adjunctive for partial seizures Start at 50mg PO BID, inc. q1-2wks to 200mg PO BID (or more) Few drug interactions SE: somnolence, headache, fatigue, rash Long half-life: 63 hours Sulfa compound ---- cross-reactivity with sulfa drugs??? Some- Studies in partial and sec generalized tonic/clonic sz ADRs: infrequent. But 2% of pts have been found to have renal calculi, dizziness and mental slowing depending on rate of escalation Renally excreted after conjugation Half life of 2-3 days as monotherapy or days with enzyme inducers
 Few drug interactions. SE: somnolence, headache, fatigue, rash. Long half-life: 63 hours. Sulfa compound ---- cross-reactivity with sulfa drugs Some- Studies in partial and sec generalized tonic/clonic sz. ADRs: infrequent. But 2% of pts have been found to have renal calculi, dizziness and mental slowing depending on rate of escalation. Renally excreted after conjugation. Half life of 2-3 days as monotherapy or days with enzyme inducers.")
53
Lacosamide (Vimpat) FDA approved for adjunctive treatment of partial-onset seizures (and diabetic neuropathic pain) Both IV and PO Works on slow inactivation Na channel Schedule V BID dosing ( mg/day) IV/po New….limited formulary.
 IV/po. New….limited formulary.")
54
Special populations

55
Epilepsy and Women Reproductive Health Osteoporosis Cosmetic Reasons
Catamenial Epilepsy Infertility (ie. PCOS) Contraception (ie. drug interactions) Pregnancy (ie. frequency of seizures to mom) Fetal Malformations Osteoporosis Cosmetic Reasons Many sex-specific concerns. Sz have been linked to menarche, menstrrual cycles, and menopause. Family planning is affected by both seizures and AEDs Sex hormones alter neuronal excitability Estorgen inhibits aminobutyric acid and potentiates glutamate resulting in heightened excitability (pro-convulsive) Progesterone (anti-convulsive) has opposite effect; its metoboites potentiate barbiturate-like ligands at the aminobutyric acid channel resulting in increased inhibition with reduced epileptiform discharges and fewer sz. Consequentely sz frequency can be altered at puberty, during a menstrual cycle, pregnancy, and menopause CBZ, PHT, PB and VA all alter endogenous steroid hormones. Newer drugs like lamotrigine and GABA do not and thus have been advantageous. Contraception: higher failure rate of hormonal contraception, esp with enzyme inducing AED: ie. Barbs, PTN, CBZ, OBZ, lesser extent felbamate and topiramate. Can still use OCP but must use higher does with 50mcg of estradiol rather than typical 20-35mcg. Hormonal contraceptives have not been reported to interfere with sz control Good alternative agents to use with OCP are VA, gabapentin, lamotrigine, levetiracetam or benzoslow dose tiagabine does not interact but may with higher doses Pregnancy: goal is to remain sz-free. 2-3 fold increase in common complications of preganacy occurs in women with eopilepsy. High rate of spontaneous abortions and lower fertility rates. Generalized tonic-clonic sz are harmful to devleoping fetus…causing alterations in blood pressure, oxygenation, and electrolytes. Effects of preg on epilepsy: 25% will experience inc in sz. Most commonly seen by the end of 1st trimester or beginninf of second trimester. Reasons are multifactorial: med compliance, lowered AED levels , sleep deprivation and stress decline in levels due to accelerated hepatic metobolism, N/V, changes in plasma volume, absorption, and protein binding. Although total levels decline, free levels may increase b/c of lowered serum albumin. Thus both free and total levels should be checked Folic acid def: PTN, CBZ, and barbs interfere with absorption/metabolism of folate. Needed to prevent neural tube defects and cleft palate Fetal Malformation: major defects include fetal hydantion syndrome cleft palate and enlarged facial bones. , cardiac defects, cleft lip, skeletal malforamtion. AR are greater with polytherapy vs monotherapy, higher vs lower AED levels, and AED-treated vs untreated women. Osteoporosis – women are already at a higher risk than men for issues of osteo. But AEDs can cause additive damage by inducing the metabolism of vitamin D. ie PTN, PB, CBZ and primadone. Reports of valproic acid causing decrease in bone mass. Mech still uncertain but may be associatate with an increase in ionized calcium which via negative feedback mechanisms reduces secratio of PTH and suprersses formatino of vitamin d.
 Contraception (ie. drug interactions) Pregnancy (ie. frequency of seizures to mom) Fetal Malformations. Osteoporosis. Cosmetic Reasons. Many sex-specific concerns. Sz have been linked to menarche, menstrrual cycles, and menopause. Family planning is affected by both seizures and AEDs. Sex hormones alter neuronal excitability. Estorgen inhibits aminobutyric acid and potentiates glutamate resulting in heightened excitability (pro-convulsive) Progesterone (anti-convulsive) has opposite effect; its metoboites potentiate barbiturate-like ligands at the aminobutyric acid channel resulting in increased inhibition with reduced epileptiform discharges and fewer sz. Consequentely sz frequency can be altered at puberty, during a menstrual cycle, pregnancy, and menopause. CBZ, PHT, PB and VA all alter endogenous steroid hormones. Newer drugs like lamotrigine and GABA do not and thus have been advantageous. Contraception: higher failure rate of hormonal contraception, esp with enzyme inducing AED: ie. Barbs, PTN, CBZ, OBZ, lesser extent felbamate and topiramate. Can still use OCP but must use higher does with 50mcg of estradiol rather than typical 20-35mcg. Hormonal contraceptives have not been reported to interfere with sz control. Good alternative agents to use with OCP are VA, gabapentin, lamotrigine, levetiracetam or benzoslow dose tiagabine does not interact but may with higher doses. Pregnancy: goal is to remain sz-free. 2-3 fold increase in common complications of preganacy occurs in women with eopilepsy. High rate of spontaneous abortions and lower fertility rates. Generalized tonic-clonic sz are harmful to devleoping fetus…causing alterations in blood pressure, oxygenation, and electrolytes. Effects of preg on epilepsy: 25% will experience inc in sz. Most commonly seen by the end of 1st trimester or beginninf of second trimester. Reasons are multifactorial: med compliance, lowered AED levels , sleep deprivation and stress. decline in levels due to accelerated hepatic metobolism, N/V, changes in plasma volume, absorption, and protein binding. Although total levels decline, free levels may increase b/c of lowered serum albumin. Thus both free and total levels should be checked. Folic acid def: PTN, CBZ, and barbs interfere with absorption/metabolism of folate. Needed to prevent neural tube defects and cleft palate. Fetal Malformation: major defects include fetal hydantion syndrome cleft palate and enlarged facial bones. , cardiac defects, cleft lip, skeletal malforamtion. AR are greater with polytherapy vs monotherapy, higher vs lower AED levels, and AED-treated vs untreated women. Osteoporosis – women are already at a higher risk than men for issues of osteo. But AEDs can cause additive damage by inducing the metabolism of vitamin D. ie PTN, PB, CBZ and primadone. Reports of valproic acid causing decrease in bone mass. Mech still uncertain but may be associatate with an increase in ionized calcium which via negative feedback mechanisms reduces secratio of PTH and suprersses formatino of vitamin d.")
56
Women and contraceptives (drug interactions)
Oral Contraceptives Pills (OCP’s) Interacts with lamotrigine by 40-50% reduction of lamotrigine blood levels Patient on Enzyme inducing AED’s: Use at least mcg of estrogen (older OCP’s) Tricycle (3 month consecutive cycle without 7 day placebo) with 4 days placebo between tricycles Does not apply to Depot forms (use normal dose)
 Interacts with lamotrigine by 40-50% reduction of lamotrigine blood levels. Patient on Enzyme inducing AED’s: Use at least mcg of estrogen (older OCP’s) Tricycle (3 month consecutive cycle without 7 day placebo) with 4 days placebo between tricycles. Does not apply to Depot forms (use normal dose)")
57
Pregnancy Planned pregnancy important!! 50% are unplanned pregnancies
Use mono therapy with lowest dose Avoid if possible: Use of valproic acid (Depakote) Dose effect?: High dose > 1000 mg more likely than lower doses Possibly carbamazepine? Risk of birth defects is 2-3% in general population Monotherapy has odds ratio (OR) of 2.8 Poly therapy has OR of 4.2 Folic Acid supplements ~ 5 mg/day
 Dose effect : High dose > 1000 mg more likely than lower doses. Possibly carbamazepine Risk of birth defects is 2-3% in general population. Monotherapy has odds ratio (OR) of 2.8. Poly therapy has OR of 4.2. Folic Acid supplements ~ 5 mg/day.")
58
Cosmetic Considerations
Phenytoin – Gingival hyperplasia, hirsutism, coarse facial features Changes in Weight: Weight Gain Neutral Weight Loss Valproic acid Lamotrigine Topiramate Gabapentin Levetiracetam Zonisamide Carbamazepine Phenytoin Felbamate Tiagabine Vigabatrin Weight gain: VPA, Gabapentin – have the highest maximal within 6 mo. CBZ, tiagabine, vigabatrin – have been associated Weight loss: Topiramate, Zonisamide, Felbamate Asconape JJ. Seminars in Neurology

59
Drug Interactions 1A2 2C9 2C19 2D6 3A4 UGT PHT Inducer PB CBZ VPA
Inhibitor inhibitor LTG Wk inducer TPM Wk inhibitor GBP LEV OXC inducer Enzyme Induction: results in an increase in rate of metabolism of affected drug, decrease in serum conc of parent drug, and poss loss of efficacy. If the affected drug has an active metabolite, induction can cause an increase in drug therapeutic effect or cause toxicity. Takes about 1-2 weeks to see inductive effect and the same amount when discontinuing med. Enzyme inhibition: usually occurs b/c of competition at the enzyme site. Most abundant isoenzyme is 3A4; involved in metabolism of more than 50% of all drugs Protein-binding displacement interactions: clinically sig interactions occur only in highly protein-bound drugs. PTN and VA are the most important in these reactions. Phenytoin: increases met of CYP2C AND CYP3A subfamilies and UGT enzymes - warfarin: see an initial increase in INR due to competitively inhibits metabolism of warfarin and displaces warfarin from albumin-binding sites. After 1-2 weeks induction of 2C9 occurs and INR drops. PB: Pharmacokinetic interactions between antiepileptic drugs. Clinical considerations. CBZ: also induces it own metabolism through 3A4 to CBZ-10,11-epoxide Riva R, Albani F, Contin M, Baruzzi A. Epilepsy Center, University Department of Neurology, Bologna, Italy. Antiepileptic drug interactions represent a common clinical problem which has been compounded by the introduction of many new compounds in recent years. Most pharmacokinetic interactions involve the modification of drug metabolism; the propensity of antiepileptic drugs to interact depends on their metabolic characteristics and action on drug metabolic enzymes. Phenobarbital, phenytoin, primidone and carbamazepine are potent inducers of cytochrome P450 (CYP), epoxide hydrolase and uridine diphosphate glucuronosyltransferase (UDPGT) enzyme systems; oxcarbazepine is a weak inducer of CYP enzymes, probably acting on a few specific isoforms only. All stimulate the rate of metabolism and the clearance of the drugs which are catabolised by the induced enzymes. Valproic acid (valproate sodium) inhibits to different extents many hepatic enzyme system activities involved in drug metabolism and is able to significantly displace drugs from plasma albumin. Felbamate is an inhibitor of some specific CYP isoforms and mitochondrial beta-oxidation, whereas it is a weak inducer of other enzyme systems. Topiramate is an inducer of specific CYP isoforms and an inhibitor of other isoforms. Ethosuximide, vigabatrin, lamotrigine, gabapentin and possibly zonisamide and tiagabine have no significant effect on hepatic drug metabolism. Apart from vigabatrin and gabapentin, which are mainly eliminated unchanged by the renal route, all other antiepileptic drugs are metabolised wholly or in part by hepatic enzymes and their disposition may be altered by metabolic changes. Some interactions are clinically unremarkable and some need only careful clinical monitoring, but others require prompt dosage adjustment. From a practical point of view, if valproic acid is added to lamotrigine or phenobarbital therapy, or if felbamate is added to phenobarbital, phenytoin or valproic acid therapy, a significant rise in plasma concentrations of the first drug is expected with a corresponding increase in clinical effects. In these cases a concomitant reduction of the dosage of the first drug is recommended to avoid toxicity. Conversely, if a strong inducer is added to carbamazepine, lamotrigine, valproic acid or ethosuximide monotherapy, a significant decrease in their plasma concentrations is expected within days or weeks, with a possible reduction in efficacy. In these cases a dosage increase of the first drug may be required. Anderson GD. Annuals of Pharm 1998
, epoxide hydrolase and uridine diphosphate glucuronosyltransferase (UDPGT) enzyme systems; oxcarbazepine is a weak inducer of CYP enzymes, probably acting on a few specific isoforms only. All stimulate the rate of metabolism and the clearance of the drugs which are catabolised by the induced enzymes. Valproic acid (valproate sodium) inhibits to different extents many hepatic enzyme system activities involved in drug metabolism and is able to significantly displace drugs from plasma albumin. Felbamate is an inhibitor of some specific CYP isoforms and mitochondrial beta-oxidation, whereas it is a weak inducer of other enzyme systems. Topiramate is an inducer of specific CYP isoforms and an inhibitor of other isoforms. Ethosuximide, vigabatrin, lamotrigine, gabapentin and possibly zonisamide and tiagabine have no significant effect on hepatic drug metabolism. Apart from vigabatrin and gabapentin, which are mainly eliminated unchanged by the renal route, all other antiepileptic drugs are metabolised wholly or in part by hepatic enzymes and their disposition may be altered by metabolic changes. Some interactions are clinically unremarkable and some need only careful clinical monitoring, but others require prompt dosage adjustment. From a practical point of view, if valproic acid is added to lamotrigine or phenobarbital therapy, or if felbamate is added to phenobarbital, phenytoin or valproic acid therapy, a significant rise in plasma concentrations of the first drug is expected with a corresponding increase in clinical effects. In these cases a concomitant reduction of the dosage of the first drug is recommended to avoid toxicity. Conversely, if a strong inducer is added to carbamazepine, lamotrigine, valproic acid or ethosuximide monotherapy, a significant decrease in their plasma concentrations is expected within days or weeks, with a possible reduction in efficacy. In these cases a dosage increase of the first drug may be required. Anderson GD. Annuals of Pharm")
60
Epilepsy and Elderly Sedation, behavioral disturbances, and cognitive impairment significantly accentuated More sensitive and s/e can develop at levels not considered to be high. Pharmacokinetics: Metabolism: slower (both CBZ and VA converted to active metabolite) Renal clearance: lower Lower albumin affecting binding of AED; more free levels Drug Interactions: 2/3 of pts over 60 are taking 7 medications Osteoporosis Classically sz disorders were thought to have the highest occurance in infancy and childhood. As people are starting to live longer seeng a trend increasing in the elderly. Condiation at greatest risk were Alzheimers, cerebrovascular dx and brain tumors. Post-traumatic epil has highest incidenct in yr age group; up to 50% of individ with head injury will develop sz (Jennett, 1975) important prognositc factors include prolonged period of unconsciousness, evidnce of contusion or penetrating head injuries Pt over 65, vascular dx is most common reason and depends on area or stucture in CNS injured. Highest incidence of sz is associated with embolic strokes, AVM, ICH, and arteritis (Foster and Booker, 1983) Some association with degenerative dementias causeing sz And as we age renal and hepatic medical disordesr are common leading to sz Drug overdoses more susceptible to neruotoxic effects of AED including gait disturbance, sedation, tremor
 Renal clearance: lower. Lower albumin affecting binding of AED; more free levels. Drug Interactions: 2/3 of pts over 60 are taking 7 medications. Osteoporosis. Classically sz disorders were thought to have the highest occurance in infancy and childhood. As people are starting to live longer seeng a trend increasing in the elderly. Condiation at greatest risk were Alzheimers, cerebrovascular dx and brain tumors. Post-traumatic epil has highest incidenct in yr age group; up to 50% of individ with head injury will develop sz (Jennett, 1975) important prognositc factors include prolonged period of unconsciousness, evidnce of contusion or penetrating head injuries. Pt over 65, vascular dx is most common reason and depends on area or stucture in CNS injured. Highest incidence of sz is associated with embolic strokes, AVM, ICH, and arteritis (Foster and Booker, 1983) Some association with degenerative dementias causeing sz. And as we age renal and hepatic medical disordesr are common leading to sz. Drug overdoses. more susceptible to neruotoxic effects of AED including gait disturbance, sedation, tremor.")
61
Discontinue? Factors: Type of seizure Age at onset
Primary generalized sz (except JME) Age at onset > 2 yrs of seizure freedom on AED (>60% success) No prior attempt being unsuccessful Etiology Normal Neurologic exam Control of seizure (frequency, duration, severity) Normal EEG’s
 Age at onset. > 2 yrs of seizure freedom on AED (>60% success) No prior attempt being unsuccessful. Etiology. Normal Neurologic exam. Control of seizure (frequency, duration, severity) Normal EEG’s.")
62
QUESTIONS?

63
Neuropathic pain and drug therapy
TCAs AEDs SNRIs Lidocaine patch 5% Botulinum toxin Capsaicin Patch IMPORTANT 4-8 week trial for efficacy!

64
Agents in neuropathy

65
Studies

66
NNT and NNH

67
Side effects TCAs (amitriptyline > nortrip, desipramine)
Drowsiness, confusion (caution elderly=falls) Dry mouth Orthostatic hypotension Weight gain Urinary retention EKGs for patients over 40 (screen & routine) CAUTION in patients with cardiac disease Increase risk of MI, sudden cardiac death >100mg\/day
 Dry mouth. Orthostatic hypotension. Weight gain. Urinary retention. EKGs for patients over 40 (screen & routine) CAUTION in patients with cardiac disease. Increase risk of MI, sudden cardiac death >100mg\/day.")
68
Side effects AEDs (gabapentin, pregabalin) Drowsiness
Dizziness, cognitive or gait impairment Peripheral edema

69
Side effects SNRIs (duloxetine, venlafaxine) Nausea Dizziness
Dry mouth Sexual dysfunction EKG in patients with CV risk (venlafaxine) Blood pressure increase at high doses (venlafaxine)
 Blood pressure increase at high doses (venlafaxine)")
70
Specific agents Nortriptyline, desipramine: Duloxetine:
Start 25 mg qhs increase q3-5 days Maximum 150 mg Drug level????? Duloxetine: Start 30 mg qhs increase in a week Target dose 60 mg qd (60mg qd = 60mg bid) Max 60 mg bid
 Max 60 mg bid.")
71
Specific agents Venlafaxine: Gabapentin:
Start XR 37.5 mg qd increase 75 mg q week Maximum 225 mg qd Efficacy at mg/day Gabapentin: Start mg qhs OR mg q8h Increase q day to week depending on tolerance Max dose 3600 mg qd (1200mg q8 h) RENALLY ELIMINATED
 RENALLY ELIMINATED.")
72
Specific agents Pregabalin: Lidocaine patch 5%
50 mg tid or 75 mg bid increase 3-7 days as tolerated Target 200 mg tid or 300 mg q12 h Efficacy 300mg/day = 600 mg/day?? Increase s/e RENALLY eliminated Lidocaine patch 5% Qday off for 12 hours Maximum of 3 patches

73
Specific agents Opoids: Tramadol Methadone ???
Start 50 mg qid based off tolerance max 400 mg/day Less efficacious than opioids? RENALLY eliminated = seizures

74
Combination therapy LOW threshold to start!
No one medication is effective for all Adverse effects limit dose Combos studied: Gabapentin + MS Pregabalin + oxycodone Nortriptylene + gabapentin Pregabalin + lidocaine patch Valproate + glyceryl trinitrate spray

75
Tom’s tips

76
Antibiotics Vancomycin: Zosyn: Weight based
load mg/kg (max 2 to 2.5G load) then 15 mg/kg (actual wt.) q 12h (q8 h dosing?) Zosyn: Dosing for pseudomonas is 4.5 G q6 h Dose based off GFR Possible use Cefepime due to increase resistance
 then 15 mg/kg (actual wt.) q 12h (q8 h dosing ) Zosyn: Dosing for pseudomonas is 4.5 G q6 h. Dose based off GFR. Possible use Cefepime due to increase resistance.")
77
Antibiotics Acyclovir: Cipro (fluroquinalones) NOT pft
10 mg/kg based off IDEAL body wt. ALWAYS IV fluids ~ 80 mL/h Cipro (fluroquinalones) NOT pft Dexamethasone for pneumococcal meningitis?? I say YES! Dex 10 mg iv/po q6 h for 4 days
 NOT pft. Dexamethasone for pneumococcal meningitis I say YES! Dex 10 mg iv/po q6 h for 4 days.")
78
Phenytoin or phosphenytoin
Dose mg/kg (guess wt) 1mg/kg = 1 point in total level (little less than) Monitor free levels especially in ICU About $1-2 more with total at HMC and UW Normal ratio 1:10 but can change based off: Albumin Other bound drugs BUN and Tb
 1mg/kg = 1 point in total level (little less than) Monitor free levels especially in ICU. About $1-2 more with total at HMC and UW. Normal ratio 1:10 but can change based off: Albumin. Other bound drugs. BUN and Tb.")
79
Phenytoin or phosphenytoin
Dose: x mg IV = x mg PO = x mg BID pft Osteoporosis: use IU Vit D with Ca Phenytoin rate = 50mg/min OR 25mg/min Cardiovascular patients or elderly Hypotension….SLOW rate! Phosphenytoin rate = 150 mg/min

80
More AEDs ! Valproate: Carbamazepine drug levels: Phenobarbital:
Check NH4 levels if altered mental status Decrease l-carnitine stores Carbamazepine drug levels: Do NOT reflect active metabolite 10,11 epoxide Roughly 10% of parent drug unless inducer on. Phenobarbital: GREAT for AWS! Binding difference!

81
Drug Interactions! Aspirin with NSAID reduced effectiveness of ASA
Plavix + ASA: unless stent should use ASA 81 mg – decrease risk for GI bleed Plavix + PPI = CONTROVERSIAL..avoid??...unless of course GI bleed then Pantoprazole Meropenem + valproate = 60% decrease in valproate levels

82
Treatment of hypertension

83
What’s in store? CHEP 2009 guidelines Combination therapy
Treatment of resistant hypertension Hypertension in the old – therapy? Blood pressure variability and risk Thiazide is a thiazide? NO!!

84
CHEP guidelines 2009

85
CHEP guidelines 2009

86
CHEP guidelines 2009

87
CHEP guidelines 2009

89
C = Calcium Channel Blockers D = Diuretic
Combination therapy A = ACEI or ARB B = B-Blockers C = Calcium Channel Blockers D = Diuretic

90
Combination therapy Complementary classes are 5-times more effective in lowering bp than increasing 1 drug AB-CD system Combination therapy with lower doses Antihypertensive produce dose dependant s/e Adherance: Kaiser study showed adherence inversely related to number of medications; 77%, 70%, 63%, 55% Drops with increasing number of doses; 71%, 61%, 50%, 31%.

91
Combination therapy RAAS inhibitor (ACEI, ARB) + Diuretic
Additive blood pressure reduction Diuretics reduce intravascular volume Activates RAAS = vasoconstriction, Na/H2O retention RAAS inhibitor – attenuates diuretic s/e RAAS inhibitor + CCB RAAS inhibition improves s/e of CCB (edema) CCB=arteriolar dilation, RAAS inhibition = venodilation
 CCB=arteriolar dilation, RAAS inhibition = venodilation.")
92
Treatment of resistant htn
Definition: Failure to reach goal bp despite full doses of an appropriate 3 drug regimen including diuretics Incidence not known ALLHAT 27% required 3 or more medications Potential causes: Longstanding htn Secondary htn Non-adherance to therapy Interfering medications (NSAID, Sympathomimetics) Lifestyle factors (Na intake, etoh, obesity, SA)
 Lifestyle factors (Na intake, etoh, obesity, SA)")
93
Combination therapy Studies have shown at least 75% require combination therapy: ALLHAT = 26% monotherapy HOT = 33% monotherapy LIFE = 10% monotherapy High blood pressure is usually multifactorial Volume, Cardiac performance, vascular resistance RAAS Meta-analysis shows monotherapy reduced bp by 9.1/5.5 mm Hg Little differences between classes VALUE trial showed better outcomes throughout 5 yr f/u in those that reached goal within first 6 months of tx

94
Blood pressure variability
Patients with episodic hypertension have increased risk of vascular events Benefits of medication may partly be due to reduced variability in blood pressure. Acute ischemic stroke, variability linked to hemorrhagic transformation Moderate to high SBP variability showed increased white matter disease SD of SBP was shown to be independent predictor of stroke after adjustment for mean SBP.

95
Blood pressure variability
ALLHAT trial: Small differences in mean SBP between groups Large differences in SD of SBP Paralleled group differences in stroke risk Amlodipine < chlorthalidone < lisinopril ASCOT-BPLA Mean SBP were similar Large difference in SD of SBP correlated to primary outcome amlodipine < atenolol MRC trail showed b-blockers had no effect on stroke risk despite reduction in mean sbp. Diuretic group had effect. Correlated to SD of SBP

96
Thiazide is a thiazide? Accomplish trial: Mr Fit trial:
“The data leading to the protocol change indicated that in the nine clinic whose staff prescribed hydrochlorothiazide predominantly, the trend of mortality was unfavorable for SI men compared with UC men, whereas it was favorable in the six clinics whose staff primarily used chlorthalidone. “ Accomplish trial: “A possible explanation for the difference between the outcomes of this trial and those of ALLHAT is that chlorthalidone (which was used in ALLHAT) may differ from hydrochlorothiazide (which was used in the ACCOMPLISH trial) in its effect on outcomes independently of its effect on blood pressure.”
 may differ from hydrochlorothiazide (which was used in the ACCOMPLISH trial) in its effect on outcomes independently of its effect on blood pressure.")
97
Thiazide is a thiazide? HCTZ: Chlorthalidone: Indapamide:
T1/2 = hrs Duration = 6-12 hrs Chlorthalidone: T1/2 = hrs Duration = hrs Indapamide: T1/2 = hr Duration = <36 hrs

98
Questions???

99
THANKS!!

Similar presentations