Download presentation
Presentation is loading. Please wait.

1
Respiratory Physiology
Gideon Daniel DVM

2
What are the LFT test you should know?
Compliance Resistance

3
Dynamic hyperinflation and what it means to you
\

4
Overview DEFINITONS SMALL AIRWAYS EFFECT ON LUNG MECHANICS DIAGNOSIS
THERAPY

5
Definitions Air-trapping Intrinsic (auto) PEEP Dynamic hyperinflation
 PEEP Dynamic hyperinflation")
6
Air-trapping/dynamic hyperinflation

7
Intrinsic (auto) PEEP Typically refers to ventilated patients
Inadequate time for exhalation (may or may not be pathologic) Small airway disease/mucus
 Small airway disease/mucus.")
8
What are negative effects of autoPEEP?
Potential for worsening cardiac pressure Barotrauma or hypoventilation if pressure limited ventilation

9
AutoPEEP Volume limited ventilator (increasing barotrauma and mean AWP) 35 cmH20
 35 cmH20")
10
Pressure limited ventilator (increasing risk of hypoventilation)
18 cmH20

11
Inadequate time for expiration
Inverted I: E ratio Short Te and fast rate Altered time constant

12
Time constant Lung volume changes are due to compliance of the lung and the pressure applied Lung volume = Compliance X ΔP When pressure is applied to the lung, there is a time lag until the volume change occurs The time point at which to inflate or deflate to 63% of volume is termed time constant Given also by compliance X resistance

13
Using time constant calculation to predict air-trapping
Need to permit 4-5 time constants for complete inhalation or exhalation Normal lungs, ARDS, emphysema/small airway disease Healthy dog – compliance 10 ml/cmH20; resistance 10 cmH20/L/sec ARDS dog- compliance 3 ml/cmH20; resistance 12 cmH20/L/sec COPD dog with air-trapping- compliance 25 ml/cmH20; 14 cmH20/L sec

14
Healthy Healthy dog – compliance 10 ml/cmH20; resistance 10 cmH20/L/sec Time constant Convert ml to liter (10 ml = 0.01 L) 0.01 l/cmH20 X 10 cmH20/L/sec= 0.1 seconds X 3-5 = normal inspiration/expiration should be fine in

15
ARDS ARDS dog- compliance 3 ml/cmH20; resistance 12 cmH20/L/sec
0.003 X 12= 0.036 X 5= 0.18 seconds

16
COPD COPD dog with air-trapping- compliance 25 ml/cmH20; 14 cmH20/L sec 0.025 X 14 = 0.35 X5 = 1.75 seconds

17
What are small airways? < 2 mm in diameter Conducting airways
Very small contribution to resistance

18
Small airway disease Asthma Bronchiolitis

19
When might we suspect air-trapping
Clinically, we would worry with COPD Ventilated animals * not so much ARDS

20
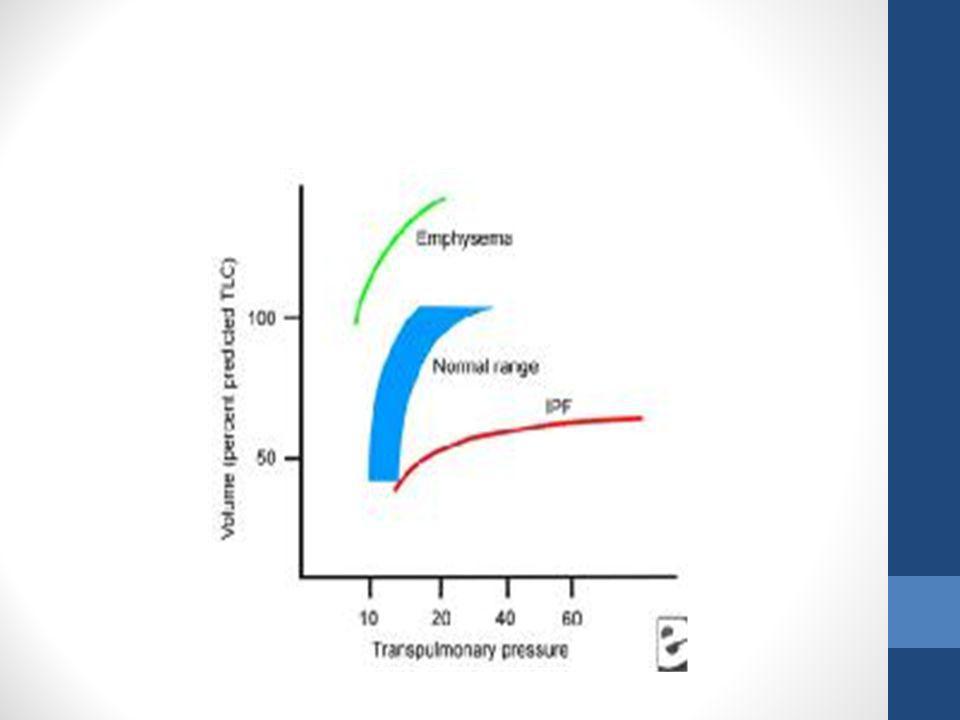
Effects of lung function
Increased lung volume Increased work of breathing since operating off the ideal P-V curve Increase WOB leads to exhaustion and respiratory fatigue

22
Diagnosis Ventilated patients Spontaneous breathing patients

23
Ventilated Increasing PEEP higher than set PEEP
Lower compliance (since at higher part of PVC curve) Breath-stacking at time
 Breath-stacking at time.")
24
Spontaneous breathing
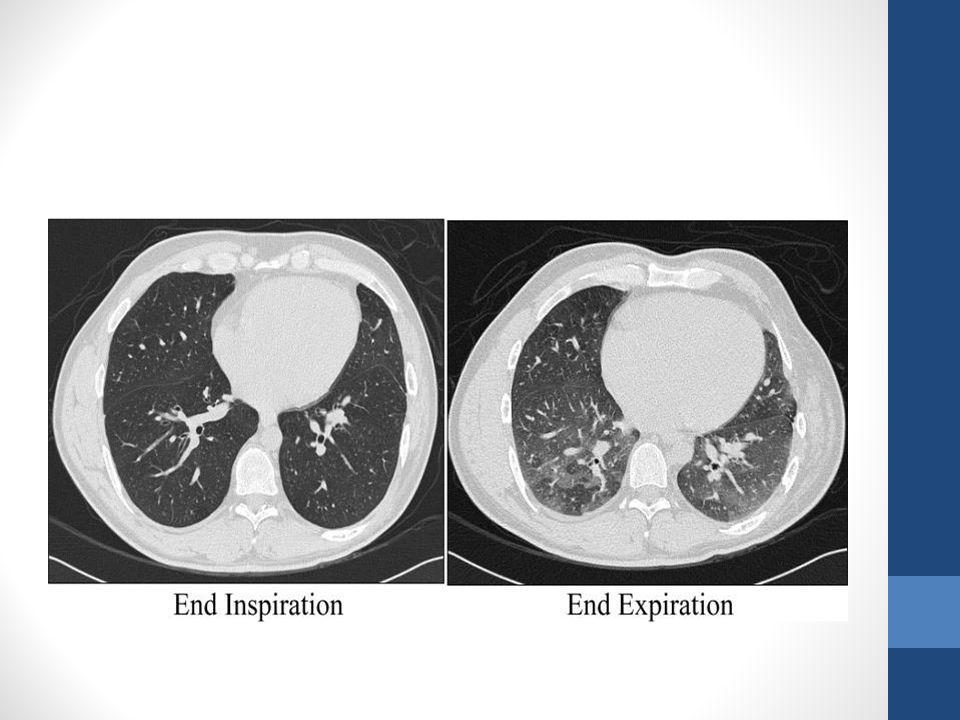
Chest shape (barrel shaped) Longer expiratory time/effort Imaging Radiographs Computed tomography
 Longer expiratory time/effort. Imaging. Radiographs. Computed tomography.")
26
Treatment Ventilated patients Spontaneous breathing patients BD
Adjust rates Spontaneous breathing patients Lung volume reduction Surgical Bronchoscopic

27
Jack Cleary NOVA (arterial sample): pH 7.329 PCO2 58 PO2 105.2
Na 147.6 K 4.94 Cl 105 Ca 1.23 BG 74 Lac 3 Crea 13.6 (BUN did not register) TCO2 32.5 BE 4 Characterize the Acid-base disturbance Is the dog on supplemental oxygen, why or why not? Is this acute or chronic? Primary respiratory acidosis and metabolic alkalosis (as expected compensation in the acute setting is around 26.7 not 32.5)- HCO3 increase 0.15meq/L for every 1mmhg increase in PCO2 (vs 0.35 w/ chronic). If chronic would be a simple disorder- i.e respiratory acidosis with metabolic compensation. On supp oxygen Acute
 TCO BE 4. Characterize the Acid-base disturbance. Is the dog on supplemental oxygen, why or why not Is this acute or chronic Primary respiratory acidosis and metabolic alkalosis (as expected compensation in the acute setting is around 26.7 not 32.5)- HCO3 increase 0.15meq/L for every 1mmhg increase in PCO2 (vs 0.35 w/ chronic). If chronic would be a simple disorder- i.e respiratory acidosis with metabolic compensation. On supp oxygen. Acute.")
28
Alternatives to blood gas?
Preliminary evaluation of the utility of comparing SpO2/FiO2 and PaO2/FiO2 ratios in dogs. Calabro, et al. JVECC 2013. Numerous studies evaluated SF in people May also be an acceptable surrogate for PaO2/FiO2 in dogs Partial pressure of end-tidal CO2 sampled via an intranasal catheter as a substitute for partial pressure of arterial CO2 in dogs. Pang, et al. JVECC 2007. Dogs for sedated for intranasal catheter placement Maybe a substitute for blood gas analysis? Excluded dogs with SPO2 < 80, > 97. Showed that SF and PF in dogs spontaneously breathing room air had good correlation. Median SF was 435 and PF 334. Enrolled 38 dogs. SF < 315 corresponded w/ PF < 300 and SF < 235 corresponded w/ PF 200. Threshold of 315 was 91% Se and 56% Sp for ALI and threshold of 235 was 85% Se and 85% Sp for ARDS ---- In non-panting healthy dogs, as w/ previous study.

29
Variables to consider Effect of body position on the arterial partial pressures of oxygen and carbon dioxide in spontaneously breathing, conscious dogs in an intensive care unit. McMillian, et al. JVECC 2009. PaO2 was significantly higher when patients were sternal compared to lateral recumbency PaCO2 levels were not significantly different

30
What are the 5 causes of hypoxemia as outlined by WEST?

31
Inadequate FiO2 Hypoventilation Diffusion impairment Shunt V-Q mismatch

32
T or F CO2 can diffuse about 20x as rapidly as oxygen for a given difference in pressure. True Fick’s law Fick’s law: the rate of transfer of gas through a sheet of tissue is proportional to tissue area and difference in partial pressures b/w the two sides, and inversely related to the tissue thickness. In the lungs the tissue area is large (50-100m2) and thickness is small (0.3um). Rate of transfer is proportional to diffusion constant (D) which depends on properties of tissue and gas.
 and thickness is small (0.3um). Rate of transfer is proportional to diffusion constant (D) which depends on properties of tissue and gas.")
33
All of the following determine diffusion of oxygen across the respiratory membrane EXCEPT
Membrane thickness Diffusion coefficient (based on solubility and molecular wt) of the gas Membrane surface area Concentration of oxygen in the inspired air Partial pressure difference of gas on either side of the membrane 4
 of the gas. Membrane surface area. Concentration of oxygen in the inspired air. Partial pressure difference of gas on either side of the membrane. 4.")
34
What is Alveolar ventilation?
Is the rate at which new air reaches the gas exchange areas of the lungs During inspiration, some of the air never reaches the gas exchange areas but instead fills respiratory passages This air is called dead space air Alveolar ventilation can be increased by either (or both) Raising tidal volume More effective b/c it reduces the proportions of each breath occupied by anatomic dead space Increasing resp frequency
 Raising tidal volume. More effective b/c it reduces the proportions of each breath occupied by anatomic dead space. Increasing resp frequency.")
35
ALI/ARDS Is a syndrome of pulmonary inflammation and edema resulting in acute respiratory failure associated with critical injury/illness Major difference b/w ALI and ARDS is the degree of hypoxemia as defined by the ratio of arterial oxygen tension to fractional inspired oxygen concentration (PaO2:FiO2) Major difference b/w ALI and ARDS is the degree of hypoxemia as defined by the ratio of arterial oxygen tension to fractional inspired oxygen concentration (PaO2:FiO2)
 Major difference b/w ALI and ARDS is the degree of hypoxemia as defined by the ratio of arterial oxygen tension to fractional inspired oxygen concentration (PaO2:FiO2)")
36
Consensus in people Clinical criteria
Acute onset of respiratory distress Presence of bilateral pulmonary infiltrates on CXR Pulmonary artery wedge pressure ≤ 18mmHg No clinical evidence of left atrial hypertension

37
ALI vs ARDS A PaO2/FiO2 ratio of 500 is considered normal
What ratio for ALI? What ratio for ARDS? < 200

38
Risk factors Pulmonary – direct injury Extra pulmonary
Pneumonia Contusion Toxin NCPE Extra pulmonary Poly-trauma Sepsis/SIRS Sepsis and pneumonia most common etiology Common sequeal of bacterial pneumonia, aspiration pneumonia, sepsis or shock. Although specfici criteria has not been identified in cats, severe sepsis has been associated w/ necropsy findings consistent with ALI/ARDS

39
Clinical signs May be delayed for 1-4 days Progressive hypoxemia
Tachypnea Respiratory distress Cyanosis Productive cough- actually rare May be delayed for 1-4 days after the inciting event triggers the pulmonary infalmmatory response PE: harsh lung sounds, progressing to crackles, orthopena, utilization of auxiliary resp muscles and foamy pink expectorate in severe cases.

40
Mechanism of lung injury
Increase in endothelial permeability, allowing leakage of protein-rich serum into the alveolar spaces Alveolar infiltrates impaired gas exchange and decreased lung compliance Relatively surfactant deficiency contributes to alveolar collapse Inflammatory response may represent an overzealous response on the part of both cellular and humoral immune system MR as high as 40-60% in humans (animals surviving rare)- most die w/in first 2wks following diagnosis. For patients that have recvoery or resolution of their pulmonary lesions, there is complete or nearly complete recovery of pulmonary fnc and QOL
- most die w/in first 2wks following diagnosis. For patients that have recvoery or resolution of their pulmonary lesions, there is complete or nearly complete recovery of pulmonary fnc and QOL.")
41
Stages of lung injury Exudative – reflects presence of protein-rich edema fluid, hyaline membranes and wbc infiltrates Proliferative - As ALI/ARDS progress – proliferation of type II pneumocytes (attempts to restore the damaged epithelium) Fibrotic phase- as dz resolves Exudative phase- pul vacular leakage and inflammatory cell infiltration; loss of capillary integrity, alveolar epithelial damage, accumulation of protien-rich fluid and dev of pulmonary edema are char feactures; Lung architecture beocmes altered as type I alveolar pneumocyte which are responsible for gas exchange are irrversibly damaged; b/c type I are unable to replicate, type II abandan their normal fnc of surfactant production to repair the denuded areas. -- type I death and alterred II fnc leads to formation of hylanine membranes, def of surfactant and collapse of alveoli; Proliferative phase- organization of exudate and dev of fibrosis char the proliferative phase; Type II proliferates in an effort to repair the denuded epithelial surfaces; Fibroblastic proliferation, initally in the pulmoanry interstitium and later in the alveolar lumen, lead to narrowing and collapse of the airspaces and pulmonary hypertension. Fibrotic- clinical manifestations of fibrosis are considered a late stage of ALI/ARDS, initiation of fibrosis actually begins much earlier in the syndrome. Magnitude- variable- from minimal to severe. Involves collagen deposition in the alveolar, vascular and intersitital beds. In humans, fibrosis is a key predictor of survival. Experimentally, can occur w/in 40d after induction of lung injury in dogs.
 Fibrotic phase- as dz resolves. Exudative phase- pul vacular leakage and inflammatory cell infiltration; loss of capillary integrity, alveolar epithelial damage, accumulation of protien-rich fluid and dev of pulmonary edema are char feactures; Lung architecture beocmes altered as type I alveolar pneumocyte which are responsible for gas exchange are irrversibly damaged; b/c type I are unable to replicate, type II abandan their normal fnc of surfactant production to repair the denuded areas. -- type I death and alterred II fnc leads to formation of hylanine membranes, def of surfactant and collapse of alveoli; Proliferative phase- organization of exudate and dev of fibrosis char the proliferative phase; Type II proliferates in an effort to repair the denuded epithelial surfaces; Fibroblastic proliferation, initally in the pulmoanry interstitium and later in the alveolar lumen, lead to narrowing and collapse of the airspaces and pulmonary hypertension. Fibrotic- clinical manifestations of fibrosis are considered a late stage of ALI/ARDS, initiation of fibrosis actually begins much earlier in the syndrome. Magnitude- variable- from minimal to severe. Involves collagen deposition in the alveolar, vascular and intersitital beds. In humans, fibrosis is a key predictor of survival. Experimentally, can occur w/in 40d after induction of lung injury in dogs.")
42
Cellular mechanism Macrophages Neutrophils Soluble mediators TNFa
IL-1B TGF-B PAF IL 6 CXCL-8 Eicosanoids IL-10 macropahges- are the earliest effector cells of the pulmonary inflammatory response – produce cytokines and chemokines include TNFa, IL1B and ROS. Activation and elaboration of proinflammatory mediators to promote neutrophil migration and directly injure alveolar epithelial cells through induction of apoptosis Neutrophils: accumulate in the early stage and predominate in the BAL fluid. Release mediators that leads to dysfunction and death of alveolar epithelial cells and decreased surfactant production. Exact role is not completely understood. DO they help macrophage initiate ALI/ARDS are simply responding to commands from macrophage? TNFa and IL-1B- predominantly form activated macrophages. Trigger additional production of inflammatory mediators- play essential role in neutrophil recruitment and activation. IL-1B also stimulates inflammatory and fibroproliferative processes. TNFa and IL1B are the earliest soluble mediators in ALI/ARDS with increased concentrations 30-90min post injury. There is sign higher concentrations of both mediators in dogs w/ ALI/ARDS form direct injury vs systemic injury TGFB- key mediator of tissue fibrosis, can be produced by every cell type. Promotes fibroproliferative response during latter phase of ALI/ARDS. Although late-stage mediator, expression is markedly increased as early as 2d after induction of injury. So likely has other roles, such as promoting pulmonary edema during the exudative phase. Also a chemoattract for macrophage/No and stimulates macrophage production of TNFa, IL-1B and PAF PAF: macrophage, No and EC produce PAF. In addition to activating plts, PAF is a potent pro-inflammatory mediator that acts also as a VD and BC. Much of the vascular endothelial effects of No are mediated through secretion of PAF. IL5- a wide range of cells can produce IL5. Induces syn of APP; excellent predictor of ALI/ARDS severity in human patients with conditions such as spesis and pancreatitis. Critical mediator of fiborblast activation and proliferation and likely plays a role in the fibroproliferative phase. CXCL8 (IL8)- derived from many cells; stimulates No recruitment and activates neutrophils, causing granule and leukotriene release and stimulates the resp burst. Severity of pulmonary neutrophila and mortality in human ALI/ARDS seem to correlate w/ CXCL-8. Eicosanoids- grp of hormones produced from arachadonic acid that include PG, TX and LK. IL10- anti-inflammatory- in humans with ~ risk factors, those who develop ALI/ARDS have lower circulating conc of IL10 and in additional, corresponds w/ poor outcome. In general immunomodulation is tricky as some mediations (like IL1-B and COX2) are initially proinflammatory mediators but then promote repair in later stages.
- derived from many cells; stimulates No recruitment and activates neutrophils, causing granule and leukotriene release and stimulates the resp burst. Severity of pulmonary neutrophila and mortality in human ALI/ARDS seem to correlate w/ CXCL-8. Eicosanoids- grp of hormones produced from arachadonic acid that include PG, TX and LK. IL10- anti-inflammatory- in humans with ~ risk factors, those who develop ALI/ARDS have lower circulating conc of IL10 and in additional, corresponds w/ poor outcome. In general immunomodulation is tricky as some mediations (like IL1-B and COX2) are initially proinflammatory mediators but then promote repair in later stages.")
43
Is this normal or abnormal?
A patient breathing room air has an arterial P02 of 49mmHg, PCO2 48mmHg and respiratory exchange ratio of 0.8. What is the approximate alveolar-arterial difference for PO2 in this patient? 41mmHg Is this normal or abnormal? Abnormal; normal A-a gradient should be < 10. Cause? Likely NOT hypoventilating –that is the the role of the A-a gradient to exclude! Indicates venous admixture PI x 0.21 = 150mmhg PAO2 = PIO2 – PaCo2/ R 150 – 60 90 A-a: 41

44
Which of the following is NOT considered a criteria for dx of ALI/ARDS?
Acute onset of respiratory distress Left atrial hypertension Decreased PaO2:FiO2 ratio Known risk factors (sepsis, pneumonia, etc) 2
 2.")
45
Regarding ALI/ARDS, which of the following statement is true?
Neutrophils are generally the first effector cells of the pulmonary response Coughing is frequently the first CS associated with these syndromes Radiographic signs are generally more unilateral than bilateral Patients with ALI have a PaO2:FiO2 ratio < 300 and those w/ ARDS have a ratio < 200mmHg 4

46
Which of the following is not a part of the consensus definition of VetALI/VetARDS?
Acute onset (< 24hrs) of tachypnea and labored breathing Known risk factors are SIRS, near-drowning, smoke inhalation Evidence of pulmonary capillary leak without increased pulmonary capillary pressure Evidence of inefficient gas exchange Evidence of diffuse pulmonary inflammation Actually 72hrs 3) i.e bilateral/diffuse infiltrates 4) Hypoexima w/o PEEP i.e ≤300 or 200 5) BAL- neutrophila
 of tachypnea and labored breathing. Known risk factors are SIRS, near-drowning, smoke inhalation. Evidence of pulmonary capillary leak without increased pulmonary capillary pressure. Evidence of inefficient gas exchange. Evidence of diffuse pulmonary inflammation. Actually 72hrs. 3) i.e bilateral/diffuse infiltrates. 4) Hypoexima w/o PEEP i.e ≤300 or ) BAL- neutrophila.")
47
Which of the following describes the proliferative phase of ALI/ARDS?
Organization of exudates and development of fibrosis with increasing numbers of Type II pneumocytes Collagen deposition in the alveolar, vascular and interstitial beds with development of microcysts in the pulmonary parenchyma Pulmonary vascular leakage and inflammatory cell infiltration with loss of capillary integrity, alveolar epithelial damage, accumulation of protein-rich fluid and development of pulmonary edema 1 2) Fibrotic 3) Exudative phase
 Fibrotic. 3) Exudative phase.")
48
Which of the following statements is false?
The exudative phase is the first phase of ALI/ARDS, and is characterized by pulmonary vascular leakage and inflammatory cell infiltration During the exudative phase, type II pneumoncytes are replaced with type I pneumoncytes The proliferative phase is the 2nd phase of ALI/ARDS, and is characterized by proliferation of type II pneumoncytes The fibrotic phase of ALI/ARDS involves collagen deposition in the alveolar, vascular and interstitial beds 2) Type I is replaced with type II
 Type I is replaced with type II.")
49
Which of the following does NOT occur in the proliferative phase of ALI/ARDS?
Collapse of alveoli Development of microcysts in pulmonary parenchyma Alerted function of type II pneumocytes Pulmonary hypertension Fibrin filled alveoli 2- this occurs in fibrotic phase

50
All are pathologic changes associated with ALI/ARDS EXCEPT?
Ventilation-perfusion mismatch Decreased compliance Increased intra-pulmonary shunt Decreased dead space relative to tidal volume 4

51
Which of the following does NOT act as a pro-inflammatory mediator in the pathogenesis of ALI/ARDS?
IL-6 TNF-alpha IL-10 PAF TGF-beta IL10

52
All of the following are known risk factors of developing ALI/ARDS except?
Pancreatitis GDV Sepsis L CHF DIC 4

53
What is another role of platelet activating factor (PAF) other than activation of platelets?
Signals the release of pro-inflammatory cytokines Causes vasodilation and bronchoconstriction Impairs the vascular endothelial effects of neutrophils Decreases development of lung injury Promotes neutrophil migration 2

54
Which mediators plays a major role in neutrophils recruitment and activation?
PAF TNF alpha TGF beta IL1b 2 and 4

55
What would be the typical BAL result from a dog with ALI/ARDS?
Proteinaceous background, neutrophils Pyogranulomatous effusion Suppurative and septic Lymphoplasmacytic 1

56
Which of the following is a key mediator in tissue fibrosis during the late stages of ALI/ARDS?
PAF Alveolar macrophages TGF-beta IL-6 3

57
Which eicosanoids are suspected to be the major players in the pathogenesis of ALI/ARDS?
Prostaglandins Prostacyclins TXA2 Leukotrienes 1 and 3 5

58
Matching- Which receptors?
Responsible for bronchodilator? B2 Responsible for bronchoconstriction? Muscarinic

59
Matching Definitions Two major lung volume categories- dynamic and static. Dynamic- tidal volume, inspiratory and expiratory reserve volume and vital capacity; Static- functional residual capacity and residual volume Inspiratory reserve volume: the maximum extra volume of air that can be inspired over and above the normal tidal volume Maximum voluntary expiration Expiratory reserve volume: the maximum extra volume of air that can be expired by forceful expiration after the end of a normal tidal expiration Residual volume: the volume of air remaining in the lungs after the most foreceful expiration Vital capacity: inspiratory resrve volume + tidal volume + expiratory reserve volume; the max amt of air a person can expel from the lugs after first filling the lungs to their maximum extent and then expiring to the maximum extent Functional residual capacity: expiratory reserve volume + residual volume; the amt of air that remains in the lungs at the end of normal expiration Total lung capacity: vital capacity + residual volume; maximum volume to which the lungs can be expanded with the greatest possible effort Tidal volume: the volume of air inspired or expired with each normal breath

60
Matching Definitions Two major lung volume categories- dynamic and static. Dynamic- tidal volume, inspiratory and expiratory reserve volume and vital capacity; Static- functional residual capacity and residual volume Inspiratory reserve volume: the maximum extra volume of air that can be inspired over and above the normal tidal volume Maximum voluntary expiration Expiratory reserve volume: the maximum extra volume of air that can be expired by forceful expiration after the end of a normal tidal expiration Residual volume: the volume of air remaining in the lungs after the most foreceful expiration Vital capacity: inspiratory resrve volume + tidal volume + expiratory reserve volume; the max amt of air a person can expel from the lugs after first filling the lungs to their maximum extent and then expiring to the maximum extent Functional residual capacity: expiratory reserve volume + residual volume; the amt of air that remains in the lungs at the end of normal expiration Total lung capacity: vital capacity + residual volume; maximum volume to which the lungs can be expanded with the greatest possible effort Tidal volume: the volume of air inspired or expired with each normal breath

61
T or F In health, the greatest resistance to airflow occurs in small terminal bronchioles False False: greatest resistance to airflow occurs in the lrg bronchi. This is b/c there are relatively few bronchi in comparison w/ abt 65K parallel terminal bronchioles, through each of which only a minute amt of air must pass. In dz conditions, the smaller broncioles often do play a greater role in determining airflow resistance for 2 reasons: 1) b/c their small size they are easily occluded 2) b/c they have a greater % of smooth muscle in the walls, they constrict easily
 b/c their small size they are easily occluded 2) b/c they have a greater % of smooth muscle in the walls, they constrict easily.")
62
The most important factor limiting flow rate during most of a forced expiration from total lung capacity is: Rate of contraction of expiratory muscles Action of diaphragm Constriction of bronchial smooth muscle Elasticity of chest wall Compression of airways 5

63
What is the difference b/w anatomic and physiologic dead space?
Anatomic dead space: represents the volume of conducting airways Physiologic dead space: the part of the tidal volume which does not participate in gas exchange

64
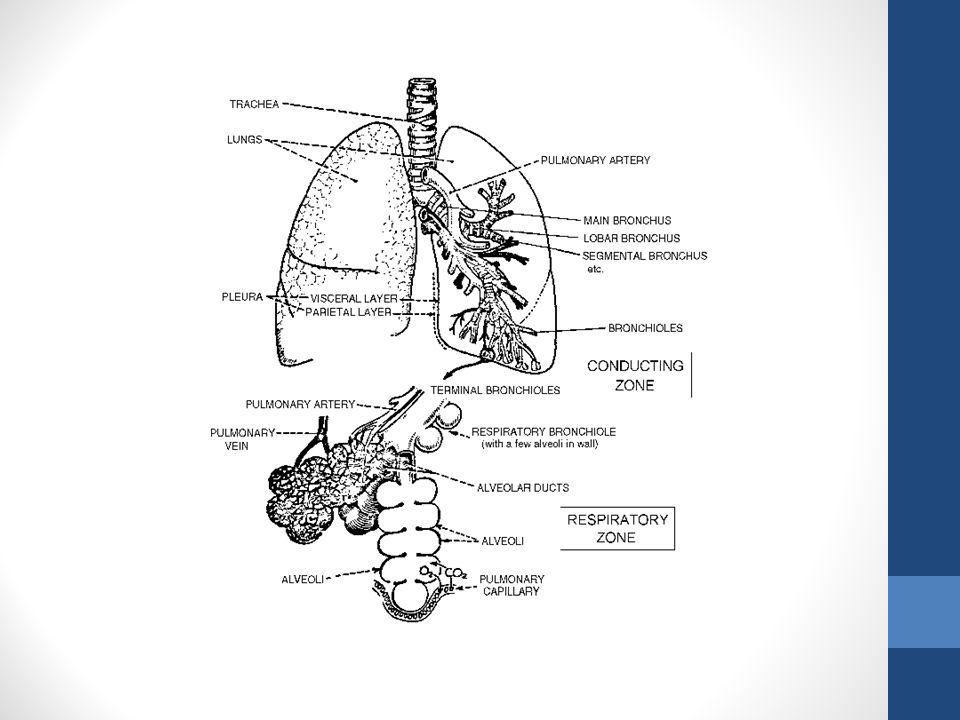
Which of the following are components of the conducting airways?
Trachea, bronchioles, alveolar ducts, and bronchi Bronchi, resp bronchioles and alveolar sacs Bronchi, bronchioles, terminal bronchioles and respiratory bronchioles Trachea, bronchi, bronchioles, and terminal bronchioles 4: the components of the resp airways/zones are resp bronchioles, alveolar ducts and alveolar sacs

66
Which of the following is NOT true about surfactant?
Surfactant decreases alveolar surface tension Surfactant is secreted primarily by type I pneumocytes as well as goblet cells Surfactant is spread over the alveolar surface and reduces the surface tension to 1/12 to ½ of the surface tension of a pure water surface As an alveolus becomes smaller, the surfactant molecules on the alveolar surface are squeezed together, increasing their concentration Answer: 2- surfactant is made of type II alveolar epithelial cells

67
Which of the following statements is FALSE? Pulmonary surfactant:
Reduces the surface tension of the alveolar lining liquid Is secreted by type II alveolar epithelial cells Contains dipalmitoyl phosphatidylcholine Increases the work required to expand the lung Helps to prevent transudation of fluid from the capillaries into the alveolar spaces 4

68
References/Additional reading
Preliminary evaluation of the utility of comparing SpO2/FiO2 and PaO2/FiO2 ratios in dogs. Calabro, et al. JVECC 2013. Partial pressure of end-tidal CO2 sampled via an intranasal catheter as a substitute for partial pressure of arterial CO2 in dogs. Pang, et al. JVECC 2007. Effect of body position on the arterial partial pressures of oxygen and carbon dioxide in spontaneously breathing, conscious dogs in an intensive care unit. McMillian, et al. JVECC 2009. Evaluation of respiratory parameters at presentation as clinical indicators of the respiratory localization in dogs and cats with respiratory distress. Sigrist, et al. JVECC 2011. Acute lung injury and acute respiratory distress syndromes in veterinary medicine: consensus definitions: the Dorothy Russell Havemeyer Working Group on ALI and ARDS in Veterinary Medicine. Wilkins, et al JVECC 2007. Acute respiratory distress syndrome in dogs and cats: a review of clinical findings and pathophysiology. DeClue, et al. JVECC 2007. Acute lung injury and Acute respiratory distress syndrome. Carpenter, et al Compendium 2001. Respiratory physiology 8th edition. West Ch 3-6. Textbook of respiratory disease in dogs and cats. King Ch 68, 23, 24.

69
Airway physiology and clinical function testing. Hoffman
Airway physiology and clinical function testing. Hoffman. Vet Clinics 2007 Small animal critical care medicine. Silverstein, Hopper, 1st edition. Chapters 34, 15. Ettinger and Feldman. “Textbook of veterinary internal medicine, 7th edition, Chapter 143, 124, 73. A case-based review of a simplified quantitative approach to acid-base analysis. Hopper, Haskins. JVECC 2008. Pulmonary abnormalities in dogs with renal azotemia. Boedec et al. JVIM 2012. Indications for and outcome of positive-pressure ventilation in cats: 53 cases ( ). Lee, et al. JAVMA 2005. Comparison of two fluid-management strategies in acute lung injury. Weidemann, et al. NEJM 2006. Comparison of the SPO2/FIO2 ratio and the PAO2/FIO2 ratio in patients with acute lung injury or ARDS. Rice, et al Chest 2007.
. Lee, et al. JAVMA Comparison of two fluid-management strategies in acute lung injury. Weidemann, et al. NEJM Comparison of the SPO2/FIO2 ratio and the PAO2/FIO2 ratio in patients with acute lung injury or ARDS. Rice, et al Chest")
Similar presentations






 Mostly covered in Lab; Control.>")










 Dr. Meg-angela Christi Amores.>")

