Download presentation
Presentation is loading. Please wait.

1
NRS 103 Thorax and Lungs Chapter 11
Nancy Sanderson MSN, RN Lecture 5

2
Concept Overview Oxygenation:
Processes that facilitate and impair oxygenation. Adequate perfusion is necessary to deliver oxygenated blood to tissues and remove metabolic waste. Intracranial regulation supports oxygenation. Adequate oxygenation needed to support intracranial function. Interrelationship necessary.

3
Anatomy and Physiology
The primary purpose of the respiratory system is to supply oxygen to cells and remove carbon dioxide . This purpose is accomplished using the process of ventilation and diffusion. Ventilation is the process of moving gases in and out of the lungs by inspiration and expiration. Diffusion is the process by which oxygen and carbon dioxide move from areas of high concentration to areas of lower concentration. After inspiration oxygen concentration is higher in the alveoli than in the pulmonary capillaries. This difference in concentration causes oxygen to move or diffuse from the alveoli across the alveoli-capillary membrane to the adjacent pulmonary capillaries. It is then carried by the erythrocytes (RBC’S) to the cells.
 to the cells.")
4
Structures in the Thorax: Mediastinum
Three main structures within thorax or chest: Mediastinum and right and left pleural cavities. Mediastinum positioned in middle of chest. Within it are: Heart Arch of aorta Superior vena cava Lower esophagus Lower part of trachea

5
Structures within the thorax:

7
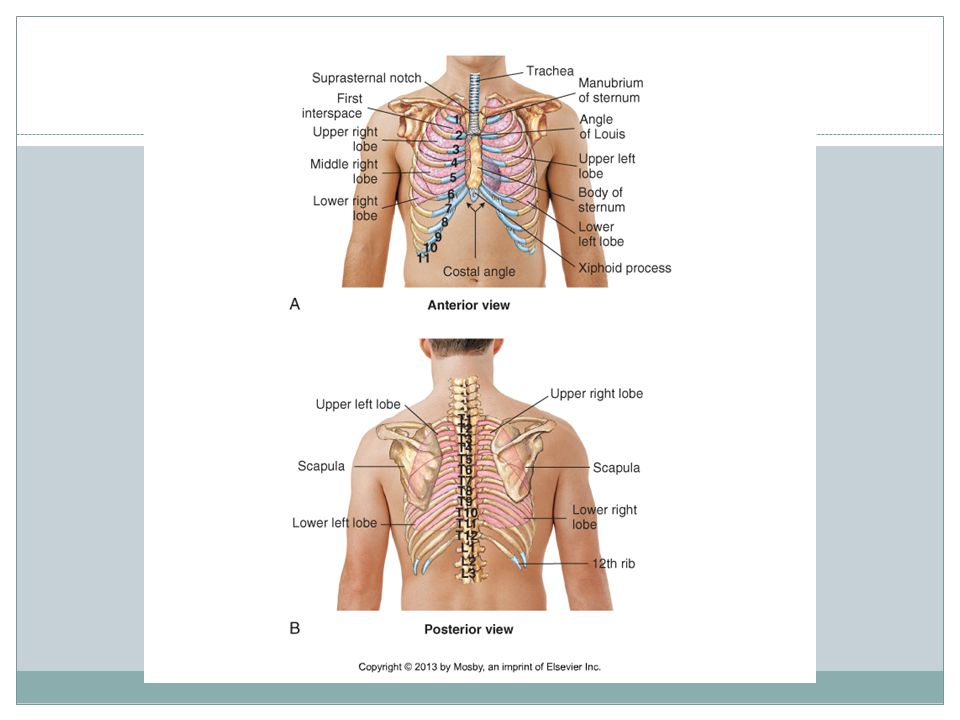
Structures of the Thorax: The lungs
Right lung has three lobes and left has two. Each lobe has a major, oblique fissure dividing upper and lower portions. However, right lung has a lesser horizontal fissure dividing upper lung into upper and middle lobes. Each lung extends anteriorly about 1.5 inches above first rib into base of neck in adults. Posteriorly, lungs’ apices rise to level of T1 (first thoracic vertebrae); lower borders expand down to T12 and, on expiration, rise to T9. Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
; lower borders expand down to T12 and, on expiration, rise to T9. Copyright © 2013 by Mosby, an imprint of Elsevier Inc.")
8
Structures in the Thorax: Pleural Cavities
Pleural cavities contain lungs. These cavities lined with two types of serous membranes: Parietal pleura Visceral pleura Chest wall and diaphragm are protected by parietal pleura, and lungs are protected by visceral pleura. Small amount of fluid lubricates space between pleurae to reduce friction as lungs move during inspiration and expiration.

9
Health History: Tobacco use (amount, duration, Pack year index) ½ pack/day x 30 years = 15 year smoking history 3rd hand smoke exposure 2nd hand smoke exposure Occupation/Exposure to pulmonary irritants Chemicals, vapors, dust, allergens, animals, smoke, asbestos, arsenic, coal dust, radiation) PMH/FH of respiratory illness/disease/cancer or allergies Pneumonia, TB, COPD, asthma, lung cancer Pneumonia or influenza vaccine received?
 PMH/FH of respiratory illness/disease/cancer or allergies. Pneumonia, TB, COPD, asthma, lung cancer. Pneumonia or influenza vaccine received")
10
Health History: TB Risk factors for TB:
HIV, substance abuse, low income or homeless, resident of nursing home, shelter or prison, immigrant from country with high TB rate

11
Health History cont. : Do you have any shortness of breath? (Dyspnea)
rest, with exercise, lying flat? Have you heard any wheezing? Do you have a cough? Dry, productive, barking, etc.. Amount, color,& consistency of sputum. Presence of odor. Hemoptysis- coughing up blood (varies from blood streaked phlegm to frank blood) Do you have chest pain with breathing? Have you recently had any pain in calves or been on any long car or plane rides?
 Do you have chest pain with breathing Have you recently had any pain in calves or been on any long car or plane rides")
12
Inspection: Observe symmetry, rate, rhythm, depth and effort of breathing Symmetry: Chest wall movement equal bilaterally Rate: Adult resp/min is normal Bradypnea: Slow (<12 per minute) Tachypnea: Rapid (>20 per minute) Rhythm: Regular vs. irregular Cheyne-Stokes, Kussmaul’s respirations, Biot’s Depth Hypoventilation–rate slow, depth Hyperventilation–rate rapid, depth deep Respirations 16/min, symmetrical,relaxed and even
 Tachypnea: Rapid (>20 per minute) Rhythm: Regular vs. irregular. Cheyne-Stokes, Kussmaul’s respirations, Biot’s. Depth. Hypoventilation–rate slow, depth. Hyperventilation–rate rapid, depth deep. Respirations 16/min, symmetrical,relaxed and even.")
13
Inspection cont.: Observe symmetry, rate, rhythm, depth and effort of breathing Symmetry: Chest wall movement equal bilaterally Rate: Adult resp/min is normal Bradypnea: Slow (<12 per minute) Tachypnea: Rapid (>20 per minute) Rhythm: Regular vs. irregular Cheyne-Stokes, Kussmaul’s respirations, Biot’s Depth Hypoventilation–rate slow, depth Hyperventilation–rate rapid, depth deep Respirations 16/min, symmetrical,relaxed and even
 Tachypnea: Rapid (>20 per minute) Rhythm: Regular vs. irregular. Cheyne-Stokes, Kussmaul’s respirations, Biot’s. Depth. Hypoventilation–rate slow, depth. Hyperventilation–rate rapid, depth deep. Respirations 16/min, symmetrical,relaxed and even.")
14
Inspection cont.: Body position Color of skin, lips, nail beds
Relaxed vs. Upright/Tripod position Color of skin, lips, nail beds Even skin tone vs. cyanotic Presence of clubbing Patient relaxed. Skin and mucous membrane pink. Nail beds pink without clubbing in upper and lower extremities. Pictures of finger clubbing pg. 108

15
Inspect/Palpate Trachea Position
Should be midline Palpate For tracheal shift Place finger in sternal notch and slip to each side. Trachea midline.

16
Inspection Documentation:
Wounds, scars, drains, tubes, dressings Documentation must include location, size, amount of drainage and discharge if present, and signs of inflammation. Additional terms to describe location: Supraclavicular- Above the clavicles Infraclavicular- Below clavicles Interscapular- Between scapula Infrascapular- Below scapula Midaxillary line- Along line of armpit Midclavicular- Along line in middle of clavicle No wounds, scars, drains, tubes, or dressings. Or- No lesions.

17
Inspection: Shape of Thorax
Shape of Chest : Deformities Symmetrical vs. asymmetrical Pectus carniatum, Pectus excavatum, Spinal deformitiies Normal AP diameter vs.. increased AP diameter Oval vs. barrel chest Ribs slope downward vs. more horizontal Barrel chest appears as if patient in continuous inspiratory position Chest symmetrical without deformities. AP < transverse. Refer to pictures on pg. 207 for examples of the above deformities and abnormals.

18
Palpation Assess for masses, tenderness, or crepitus
Subcutaneous emphysema- air escapes form lungs into subcutaneous tissue Assess chest expansion Posteriorly place thumbs at level of 10th rib & place palms on posterolateral chest. Approx 2 inches apart before inspiration. Feel thoracic expansion during quiet & deep inspiration. Look for symmetry. Chest expansion symmetrical. No masses or tenderness.

19
Palpation Tactile Fremitus
Palpable vibrations transmitted through bronchopulmonary tree to chest when patient speaks Have patient repeat 99 or 1, 1, 1 while palpate with ulnar surface or ball of hand Decreased or absent when vibration impeded by obstructed bronchus, tumor, or separation of pleural surfaces by fluid (pleural effusion), fibrosis (pleural thickening), or air (pneumothorax) Increased with gross compression or consolidation (lobular pneumonia) without bronchus obstruction Tactile fremitus equal bilaterally.
, fibrosis (pleural thickening), or air (pneumothorax) Increased with gross compression or consolidation (lobular pneumonia) without bronchus obstruction. Tactile fremitus equal bilaterally.")
20
Percussion Tapping of an chest to set chest wall and underlying tissues into motion Helps to establish if underlying tissue air-filled, fluid-filled, or solid Normal sound is resonance Resonant to percussion over all lung fields. Review pictures on pg. 204 for locations for percussion and auscultation: Anterior, Posterior and Lateral views.

21
Percussion

22
Auscultation Use diaphragm of stethoscope and
have patient breath out of their mouth. Peds- use smaller pediatric diaphragm Place stethoscope firmly on skin. Avoid movement because it may produce confusing sounds (i.e. clothing) Auscultate at least one complete respiration Move from one side to the other Observe for hyperventilation, allow to rest if needed Peds- transmission of sounds enhanced, harder to localize sounds
 Auscultate at least one complete respiration. Move from one side to the other. Observe for hyperventilation, allow to rest if needed. Peds- transmission of sounds enhanced, harder to localize sounds.")
23
Auscultation (con’t) Hairy chest men: Put stethoscope on skin
Hold stethoscope firmly over chest hair Prevents moving over and giving false sounds Put stethoscope on skin (seasoned nurses and MD’s may put over light shirt because of expert status)
")
24
Auscultation: Anterior

25
Auscultation Adventitious Breath Sounds Wheezes (Sibilant wheeze)
High pitched, musical sound heard during inhalation or exhalation Mild, moderate, severe Rhonchi (Sonorous wheeze) Low pitch snoring sound during inspiration or exhalation, but louder on exhalation May clear with coughing Asthma
 Low pitch snoring sound during inspiration or exhalation, but louder on exhalation. May clear with coughing. Asthma.")
26
Auscultation Crackles/Rales Popping sounds heard on inhalation Fine
High pitched fine, short, interrupted crackling sounds heard during end of inspiration Medium Lower, more moist sounds heard during middle of inspiration Course Loud, bubbly sounds heard during inspiration

27
Auscultation Stridor High pitched, harsh sound heard on inspiration when trachea or larynx is obstructed Croup, foreign body, large airway tumor

28
Auscultation Cont.: Voice Sounds Bronchophony Whispered Pectoriloquy
Normal- Muffled Abnormal- Clear Whispered Pectoriloquy Whisper “1,2,3” Normal- faint and indistinct Abnormal- clear and distinct Egophony “eeeeeeee” Normal Abnormal “aaaaaa”

29
Auscultation Documentation:
Breath sounds vesicular without adventitious sounds. Or- Lungs sounds CTA in all lung fields without wheezes, rales, rhonchi, or rubs

30
Auscultation: Abnormal
Pneumonia Atelectasis

31
pneumothorax Also known as collapsed lung Treatment is Chest tube:
Spontaneous Traumatic Tension Treatment is Chest tube:

32
Summary: Bringing it all together
Important to get good history If smokes offer smoking cessation classes History asthma What is current treatment? If has c/o chronic cough ask about history and exposure so MD can rule out (r/o): Birds including chickens r/o TB Smoker r/o cancer Chemicals/asbestos r/o cancer
: Birds including chickens r/o TB. Smoker r/o cancer. Chemicals/asbestos r/o cancer.")
33
Summary (continued) Shortness of breath and recent travel:
Pulmonary embolism Swelling of legs: DVT Proper auscultation Percussion Multiple problems & concerns

34
Summary Continued Asthma Atelectasis Bronchitis Cancer Croup Emphysema
Hemothorax Pleural Effusion Pneumonia Pneumothorax Tuberculosis

Similar presentations











 into the atmosphere Filter, moisten,>")







