Download presentation
Presentation is loading. Please wait.

1
Fungal Infections in HIV-patients
Hail M. Al-Abdely, MD Consultant, Infectious Diseases

2
Fungal Infections in HIV-patients
Cutaneous Seborrheic dermatitis Onychomycosis Skin dermatophyte infection Muco-cutaneous Candidiasis Invasive Cryptococcosis Histoplasmosis Aspergillosis Penicilliosis (Geographically restricted) Coccidioidomycosis Blastomycosis
 Coccidioidomycosis. Blastomycosis.")
3
Immunologic Status and Fungal Infections
Thrush Dermatophyte CD4 Seborrhea Cryptococcosis Histoplasmosis Aspergillosis Penicilliosis

4
Cutaneous Fungal Infections
More common More extensive Relatively more difficult to treat

9
Cutaneous candidiasis involving the moist skinfolds under the breasts
Cutaneous candidiasis involving the moist skinfolds under the breasts. The lesions are very red, and there are small red satellite lesions surrounding the main area of involvement. The typical location and the presence of satellite lesions make the gross image highly suggestive of cutaneous candidiasis. There is little tendency for deep tissue invasion with this type of lesion. (From Fitzpatrick et al.

11
Systemic Treatment of Cutaneous Fungal Infections
Fluconazole (Diflucan) Itraconazole (Sporanox) Terbinafine (Lamisil) Tinea corporis and cruris 150 mg once a week 3-4 weeks 200 mg qd 1-2 weeks 250 mg qd 2 weeks Tinea capitis 50 mg qd 3 weeks 3-5 mg/kg/day 4-6 weeks 125 mg qd (3-6 mg/kg/day) 4 weeks Onychomycosis 150 mg once a week 9 months 200 mg qd Fingernails -6 weeks Toenails - 12 weeks Pulse dosing 200 mg bid-- 1 week on, 3 weeks off, Toenails 3-4 months, Fingernails 2-3 months 250 mg qd Fingernails 6 weeks Toenails 12 weeks Tinea pedis 150 mg once a week 3-4 weeks 400 mg qd 4 weeks 250 mg qd 6 weeks Tinea versicolor 400 mg single dose 200 mg qd 5 or 7 days Studies ongoing
 Itraconazole (Sporanox) Terbinafine (Lamisil) Tinea corporis and cruris. 150 mg once a week 3-4 weeks. 200 mg qd 1-2 weeks. 250 mg qd 2 weeks. Tinea capitis. 50 mg qd 3 weeks. 3-5 mg/kg/day 4-6 weeks. 125 mg qd (3-6 mg/kg/day) 4 weeks. Onychomycosis. 150 mg once a week 9 months. 200 mg qd Fingernails -6 weeks Toenails - 12 weeks Pulse dosing 200 mg bid-- 1 week on, 3 weeks off, Toenails 3-4 months, Fingernails 2-3 months. 250 mg qd Fingernails 6 weeks Toenails 12 weeks. Tinea pedis. 150 mg once a week 3-4 weeks. 400 mg qd 4 weeks. 250 mg qd 6 weeks. Tinea versicolor. 400 mg single dose. 200 mg qd 5 or 7 days. Studies ongoing.")
12
Extensive pharyngeal candidiasis involving the soft palette and uvula of a patient with AIDS. Oral pharyngeal candidiasis can be a marker of T-cell immunosuppression. T cells are required to control candida growth on the mucosal surfaces. However, adequate neutrophil number and function are enough to prevent deep invasion, and there is surprisingly little tendency to develop disseminated candidiasis in patients who are T-cell deficient. (From Fitzpatrick et al.

13
Oro-pharyngeal Candidiasis
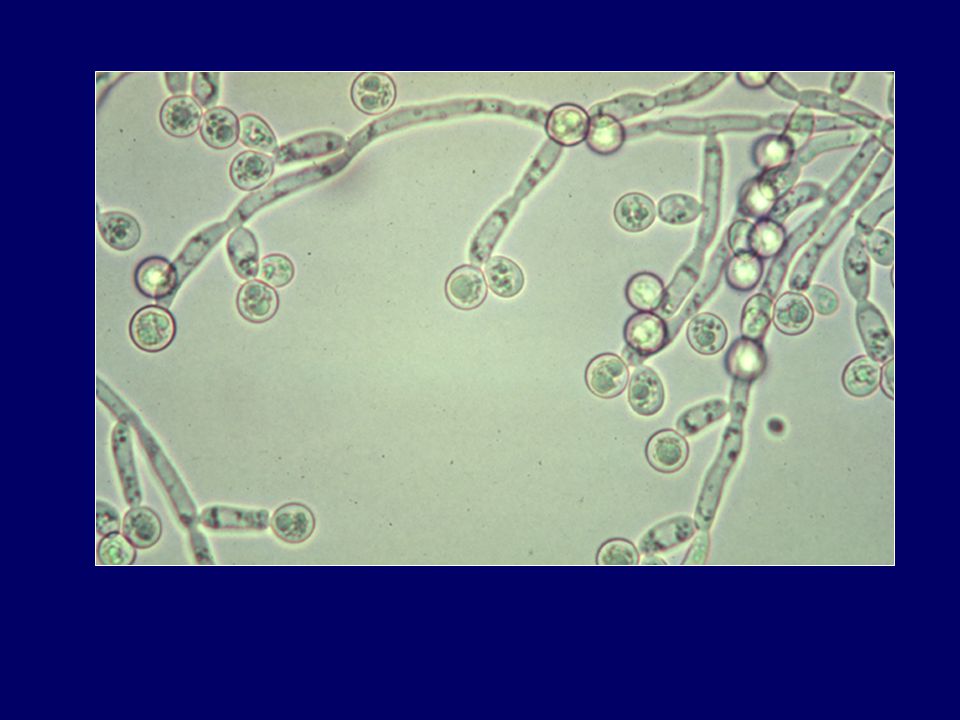
90% of HIV-patients develop OPC during their lifetime. Candida appears as part of the mouth flora in more than 80% of HIV-positive patients. Actual predisposing factors for progression from colonization to disease are not well characterized.

14
Treatment of OPC Topical agents Systemic agents
Clotrimazole, nystatin, Ampho B Systemic agents Fluconazole Itraconazole (Capsule, liquid) Ampho B
 Ampho B.")
15
Treatment of OPC Systemic treatment Strategies
Fluconazole is the most common agent. Faster action and less relapse than topical Rx. Major problem with increasing resistance. Higher dose. Switch to other agents. Strategies Treat each episode Continuous therapy

16
Esophageal Candidiasis
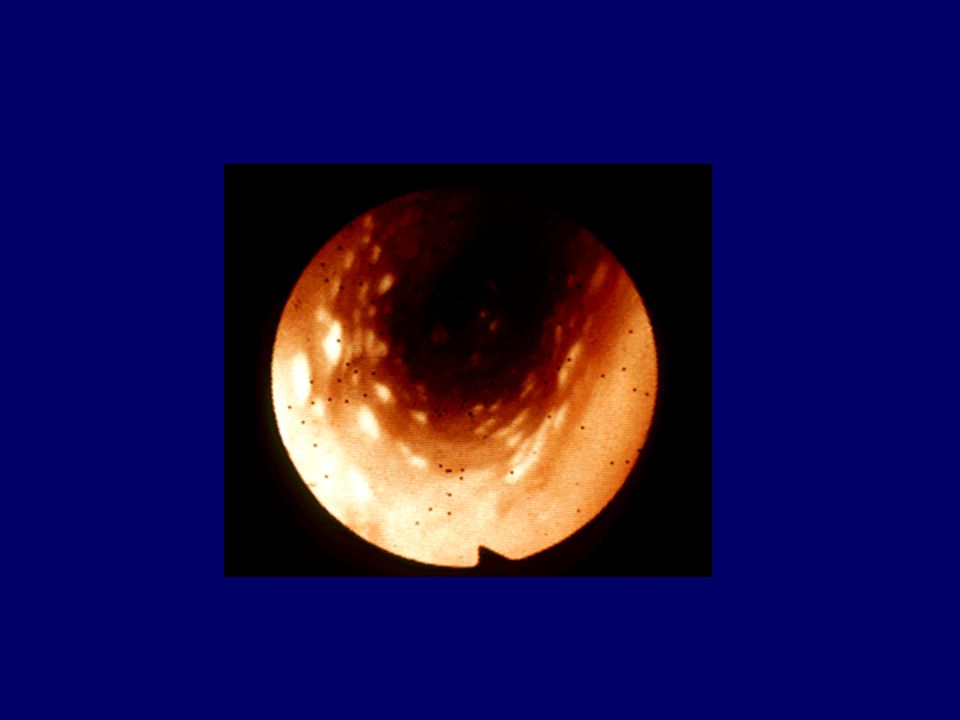
Reported in 20% to 40% of all AIDS patients. Characterized by pseudomembranes, erosions and ulcers. Presentation is mainly with odynophagia and dysphagia

18
Esophageal Candidiasis
Treatment Commonly empiric therapy. Endoscopy is indicated if the patient is not responding to antifungal therapy Drugs Fluconazole Itraconazole (Capsule, liquid) Ampho B
 Ampho B.")
19
Candidiasis and HAART Since the advent of HAART, the incidence of new Candida infections has decreased by as much as 60% to 80%

20
Vaginal Candidiasis Vulvo-vaginal candidiasis occurs in approximately 30% to 40% of HIV-infected women. ? Candidiasis more common in women with HIV infection when other important risk factors for vaginal infection (sexual activity, racial and ethnic background). HIV infection influences the severity and persistence of vulvo-vaginal Candida infection.
. HIV infection influences the severity and persistence of vulvo-vaginal Candida infection.")
21
Cryptococcosis Cryptococcus neoformans is an encapsulated yeast.
5% of HIV-infected patients in the Western World develop disseminated cryptococcosis CD4+ lymphocyte counts, less than 50 cells/mm3.

22
Cryptococcal Meningitis
Cryptococcosis typically presents as a subacute meningitis Cryptococcal meningitis rarely presents as an obvious meningitis. Initial symptoms are commonly more subtle and may just include fever and headache.

23
Symptoms of Cryptococcal Meningitis

25
Diagnosis of Cryptococcal Meningitis
Symptoms and Signs. 70% of patients with cryptococcal meningitis have positive blood cultures Serum cryptococcal antigen is a useful screening test. 1:8 is regarded as evidence of cryptococcal infection. India ink (CSF): 50% sensitive, needs experience. CSF cryptococcal antigen is rapid, sensitive and specific. Histopathological stains CSF culture.
: 50% sensitive, needs experience. CSF cryptococcal antigen is rapid, sensitive and specific. Histopathological stains. CSF culture.")
26
Treatment of Cryptococcal Meningitis
Induction amphotericin B, 0.7 mg/kg IV daily for 14 days or equivalent consider 5-flucytosine (5-FC) 25 mg/kg PO q6 hours measure opening pressure; consider means to reduce pressure if raised (>25 cms/water)
 25 mg/kg PO q6 hours. measure opening pressure; consider means to reduce pressure if raised (>25 cms/water)")
27
Treatment of Cryptococcal Meningitis
Consolidation fluconazole, 400 mg PO bid for 2 days, then daily for 8 weeks; or itraconazole, 200 mg PO tid for 3 days, then bid for 8 weeks (appears to be slightly less active) repeat lumbar puncture, with measurement of opening pressure, if patients remain symptomatic (especially persistent headache)
 repeat lumbar puncture, with measurement of opening pressure, if patients remain symptomatic (especially persistent headache)")
28
Treatment of Cryptococcal Meningitis
Maintenance fluconazole mg daily amphotericin B 1 mg/kg/week (less effective than fluconazole) itraconazole mg PO bid (less effective than fluconazole) there is no value to routine measurement of serum cryptococcal antigen
 itraconazole mg PO bid (less effective than fluconazole) there is no value to routine measurement of serum cryptococcal antigen.")
29
Treatment of Cryptococcal Meningitis
Mild presentation Fluconazole + 5-flucytosine High dose fluconazole 800 mg QD Close monitoring

30
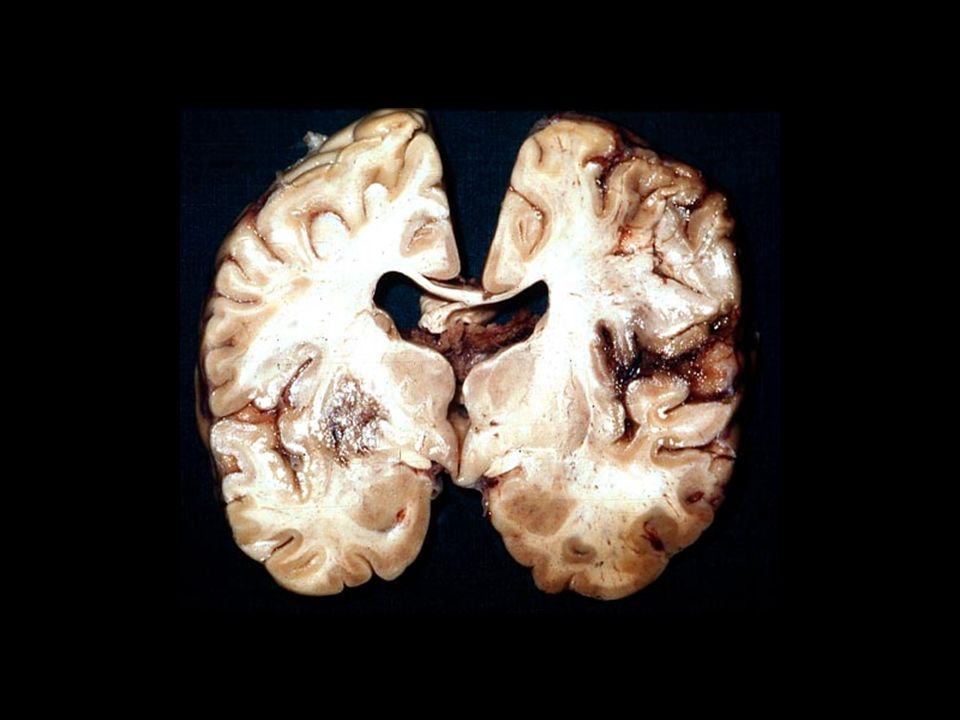
Complications of Cryptococcal Meningitis
Acute mortality happens due to cerebral edema, which may be diagnosed by a raised opening pressure of the CSF. Hydrocephalus

31
Dimorphic Fungi (Endemic Mycoses)
Histoplasmosis Coccidioidomycosis Penicilliosis marnefiei Blastomycosis Sporotrichosis

32
Histoplasmosis Coccidioidomycosis Penicilliosis

33
Characteristics of the Endemic Mycoses
Histoplasmosis Coccidioidomycosis Penicilliosis Appearance of organism on biopsy 1-5 mcm round to oval 30-80 mcm round spherules containing 2-5 mcm endospores 1-8 mcm pleomorphic elongated Method of duplication Budding Fission Clinical Features: Fever 95% 99% Weight loss 90% 60% 75% Anemia 70% 50% Pulmonary disease Lymphadenopathy 20% 10% 40-50% Skin lesions 5-10% 5% Hepatosplenomegaly 25% 10-20% Meningitis <1% Very rare

35
Aspergillosis Tends to occur in the very late stages of HIV infection, typically in patients with a history of other AIDS-defining illnesses. Two main presentations respiratory tract disease central nervous system infection

40
Conclusion Fungal infections remain an important cause of morbidity and mortality in patients with HIV disease. Epidemiology is changing with the advent of HAART. High index of suspicion is important to make a diagnosis of some of the invasive mycoses. Multiple opportunistic fungal infections can exist in the same patient on presentation.

Similar presentations


















 can be both superficial and systemic. Superficial infections (Oral and vulvovaginal candidiasis, Dermatophytosis,>")












